From Centerlines to Hemodynamics: Anisotropic RBF Decoders for Coronary Arteries
pith:RDZZYKVKreviewed 2026-06-29 14:41 UTCmodel grok-4.3open to challenge →
The pith
A transformer encoder paired with an anisotropic RBF decoder predicts coronary pressure and wall shear stress from centerlines and inlet flow more accurately than neural-operator baselines at far lower cost.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
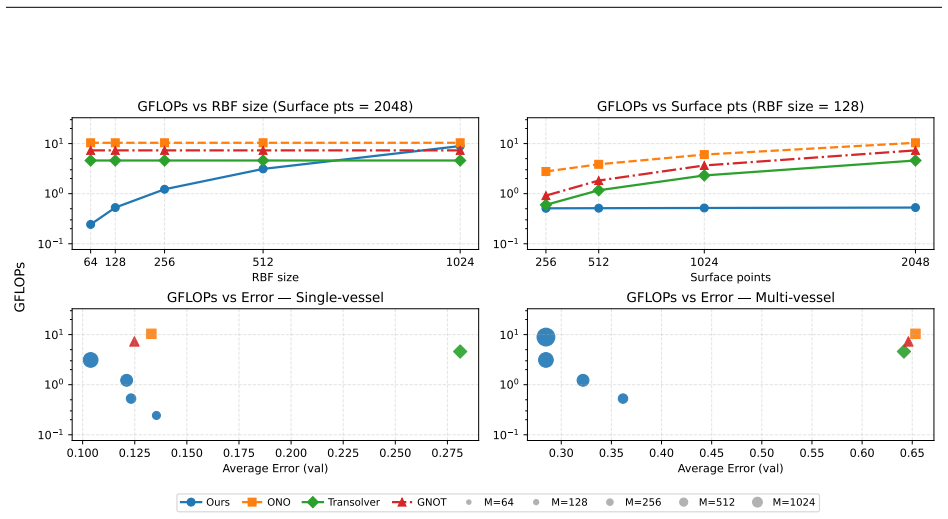
The model encodes 1D vessel centerlines together with inlet flow rate using a transformer-based encoder, and predicts continuous wall-based fields via an anisotropic Radial Basis Function (RBF) decoder aligned with vessel morphology; across both introduced datasets the approach achieves lower pressure and WSS errors than GNOT, Transolver, and ONO at a fraction of CFD cost, with the stated 52 percent error reduction and 13.8 times FLOP reduction on the multi-vessel data.
What carries the argument
Anisotropic Radial Basis Function decoder aligned with vessel morphology, which reconstructs continuous pressure and wall shear stress fields from a modest number of morphology-aware centers.
If this is right
- Hemodynamic fields can be obtained in real time from routine imaging centerlines without repeated CFD runs.
- The same encoder-decoder structure works for both single-vessel and multi-vessel coronary trees.
- Computational expense drops by more than an order of magnitude relative to GNOT while accuracy improves.
- The released single-vessel dataset enables standardized benchmarking of future centerline-to-hemodynamics models.
- Steady-state assumptions suffice for the reported accuracy gains on the generated stenosis distributions.
Where Pith is reading between the lines
- If the mapping holds on real angiograms, the framework could supply rapid non-invasive FFR estimates in clinical pipelines.
- The morphology-aligned decoder could be tested on pulsatile rather than steady inlet conditions with only minor input changes.
- Analogous centerline-to-field prediction might transfer to cerebral or peripheral arteries if the geometric encoding proves domain-agnostic.
- Further ablation of center count below 128 could map the accuracy-cost curve for deployment on limited hardware.
Load-bearing premise
Steady-state OpenFOAM simulations on randomly stenosed synthetic and ImageCAS-derived geometries supply a training distribution representative enough for the learned centerline-to-wall mapping to generalize to real patient coronary hemodynamics.
What would settle it
Comparison of the model's predicted pressure and wall shear stress against either invasive patient measurements or independent high-fidelity CFD on real clinical geometries absent from the training sets.
Figures








read the original abstract
Accurate and rapid estimation of hemodynamic metrics, such as pressure and wall shear stress (WSS), is important for assessing the severity of Coronary Artery Disease (CAD). Existing approaches, including invasive Fractional Flow Reserve (FFR) measurements and computationally expensive Computational Fluid Dynamics (CFD) simulations, face challenges in invasiveness, cost, and speed. We present a framework for fast, non-invasive coronary hemodynamics prediction. The model encodes 1D vessel centerlines together with inlet flow rate using a transformer-based encoder, and predicts continuous wall-based fields via an anisotropic Radial Basis Function (RBF) decoder aligned with vessel morphology. To support training and evaluation, we introduce two datasets with paired steady-state OpenFOAM simulations: (i) a synthetic benchmark of 4,200 single-vessel geometries with controlled anatomical variations, and (ii) a multi-vessel dataset derived from ImageCAS including 4,800 cases spanning both right and left coronary arteries, generated by randomly introducing stenoses and varying physiologically plausible flow rates. Across both datasets, our method achieves lower pressure and WSS errors than strong neural-operator baselines (GNOT, Transolver, and ONO) at a fraction of the computational cost of CFD. On the multi-vessel dataset, using 1,024 anisotropic RBF centers our model reduces the mean relative L2 error by 52% compared to the best neural-operator baseline, while at 128 centers it requires 13.8x fewer FLOPs than GNOT and still outperforms all baselines. The single-vessel dataset is publicly available at https://huggingface.co/datasets/angioinsight/single-vessel-flow.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript introduces a transformer-based encoder that processes 1D coronary artery centerlines together with inlet flow rates, paired with an anisotropic RBF decoder to predict continuous wall pressure and wall shear stress fields. Two synthetic datasets are generated via steady-state OpenFOAM simulations: a public single-vessel benchmark with controlled variations and a multi-vessel set derived from ImageCAS centerlines with randomly inserted stenoses and varied flow rates. On held-out splits from these datasets the proposed model reports lower mean relative L2 errors than GNOT, Transolver and ONO baselines (52 % reduction at 1 024 centers on the multi-vessel set) while requiring substantially fewer FLOPs at lower center counts (13.8× reduction versus GNOT at 128 centers).
Significance. If the reported error reductions on the synthetic data hold, the anisotropic RBF decoder supplies an efficient centerline-to-wall surrogate that could accelerate hemodynamic assessment relative to full CFD. The public release of the single-vessel dataset is a concrete contribution that enables reproducibility and follow-on work.
major comments (2)
- [§4 and §5.2] §4 (Model) and §5.2 (Ablation experiments): the central performance claims rest on the anisotropy of the RBF centers, yet no ablation isolating anisotropic versus isotropic RBFs is presented; without this comparison it is impossible to attribute the 52 % error reduction specifically to the anisotropy mechanism rather than to the overall architecture or center count.
- [§3 and §6] §3 (Dataset generation) and §6 (Discussion): the multi-vessel dataset is produced by random stenosis insertion on ImageCAS centerlines followed by steady-state OpenFOAM runs with non-patient-specific flow rates; the manuscript provides no external validation against in-vivo measurements or pulsatile patient-specific CFD, which directly bears on the claim that the framework constitutes a practical non-invasive alternative.
minor comments (2)
- [Abstract and §5.1] Abstract and §5.1: the headline 52 % and 13.8× figures are stated without accompanying standard deviations or test-set sizes, reducing interpretability of the quantitative improvements.
- [Figure 3 and Table 1] Figure 3 and Table 1: axis labels and color scales for the predicted versus ground-truth WSS fields are not described in the caption, making visual assessment of local error patterns difficult.
Simulated Author's Rebuttal
We thank the referee for the constructive feedback. We address the major comments point by point below.
read point-by-point responses
-
Referee: [§4 and §5.2] §4 (Model) and §5.2 (Ablation experiments): the central performance claims rest on the anisotropy of the RBF centers, yet no ablation isolating anisotropic versus isotropic RBFs is presented; without this comparison it is impossible to attribute the 52 % error reduction specifically to the anisotropy mechanism rather than to the overall architecture or center count.
Authors: We agree that demonstrating the specific contribution of anisotropy is important. In the revised version, we will include an ablation experiment that replaces the anisotropic RBF decoder with an isotropic one while keeping the encoder, number of centers, and all other hyperparameters identical. This will allow us to quantify the performance difference attributable to anisotropy alone. revision: yes
-
Referee: [§3 and §6] §3 (Dataset generation) and §6 (Discussion): the multi-vessel dataset is produced by random stenosis insertion on ImageCAS centerlines followed by steady-state OpenFOAM runs with non-patient-specific flow rates; the manuscript provides no external validation against in-vivo measurements or pulsatile patient-specific CFD, which directly bears on the claim that the framework constitutes a practical non-invasive alternative.
Authors: We acknowledge the limitation highlighted. Our work is based on synthetic steady-state data to provide a controlled and reproducible benchmark for the proposed method. Providing in-vivo validation or pulsatile simulations would require new datasets and experiments that are outside the scope of the current manuscript. We will revise the Discussion section to more clearly articulate the assumptions, limitations, and intended scope of the synthetic validation, and suggest pathways for future clinical translation. revision: partial
Circularity Check
No circularity: standard ML training/evaluation on held-out simulated data
full rationale
The paper trains a transformer+RBF model on two generated datasets (synthetic single-vessel and ImageCAS-derived multi-vessel with random stenoses + steady-state OpenFOAM) and reports relative L2 errors on test splits drawn from the identical generation pipeline. No equations, parameters, or self-citations are shown that reduce the reported performance numbers to a fitted constant or input by construction. The derivation chain consists of standard supervised learning with independent test evaluation; the central claim (error reduction vs. baselines) is not forced by redefinition or self-referential fitting.
Axiom & Free-Parameter Ledger
free parameters (2)
- number of anisotropic RBF centers
- inlet flow rate distribution
axioms (2)
- domain assumption Steady incompressible Navier-Stokes equations solved by OpenFOAM provide accurate ground-truth pressure and WSS for the generated geometries.
- domain assumption Random stenosis placement on ImageCAS centerlines produces flow fields representative of real CAD cases.
Reference graph
Works this paper leans on
-
[1]
URLhttps://api.semanticscholar.org/CorpusID:257232579. Hrvoje Jasak. Openfoam: Open source CFD in research and industry.International Journal of Naval Architecture and Ocean Engineering, 1(2):89–94, 2009. doi: 10.2478/IJNAOE-2013-0011. URLhttps:// www.sciencedirect.com/science/article/pii/S2092678216303879. DOI ambiguity: many secondary sources cite 10.37...
-
[2]
URLhttps://api.semanticscholar.org/CorpusID:276106855. James K. Min, Charles A. Taylor, Stephan Achenbach, Bon-Kwon Koo, Jonathon A Leipsic, Bjarne Linde Nørgaard, Nico H.J. Pijls, and Bernard de Bruyne. Noninvasive fractional flow reserve derived from coronary ct angiography: Clinical data and scientific principles.JACC. Cardiovascular imaging, 8 10: 120...
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.