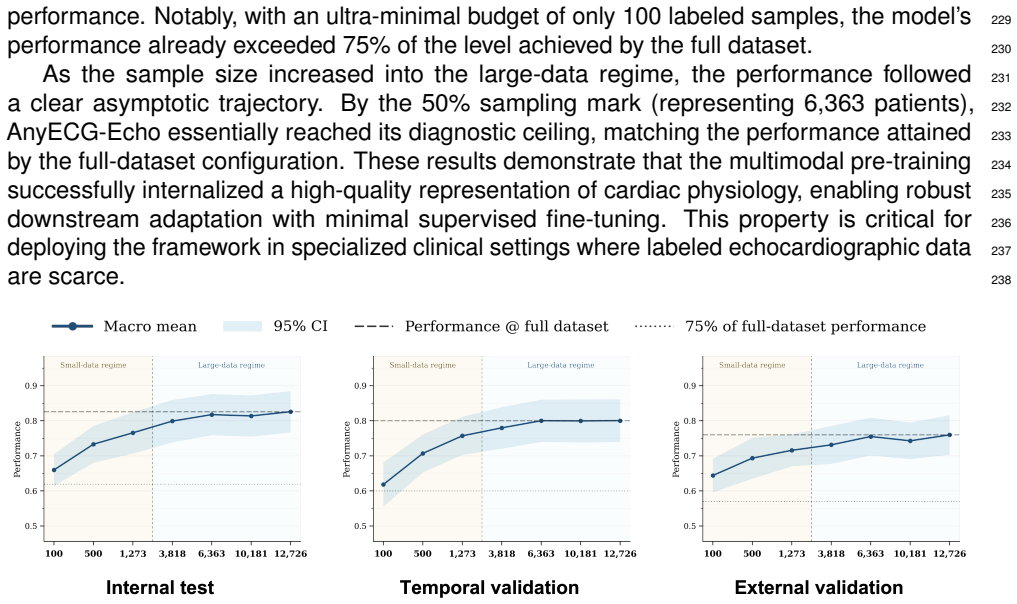
Wearable Single-Lead ECG Detects Fine-Grained Structural Heart Disease Through Echo-Report Supervision
Pith reviewed 2026-06-27 15:41 UTC · model grok-4.3
The pith
Single-lead ECGs from wearables detect 13 fine-grained structural heart disease subtypes when trained with echocardiography report supervision.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
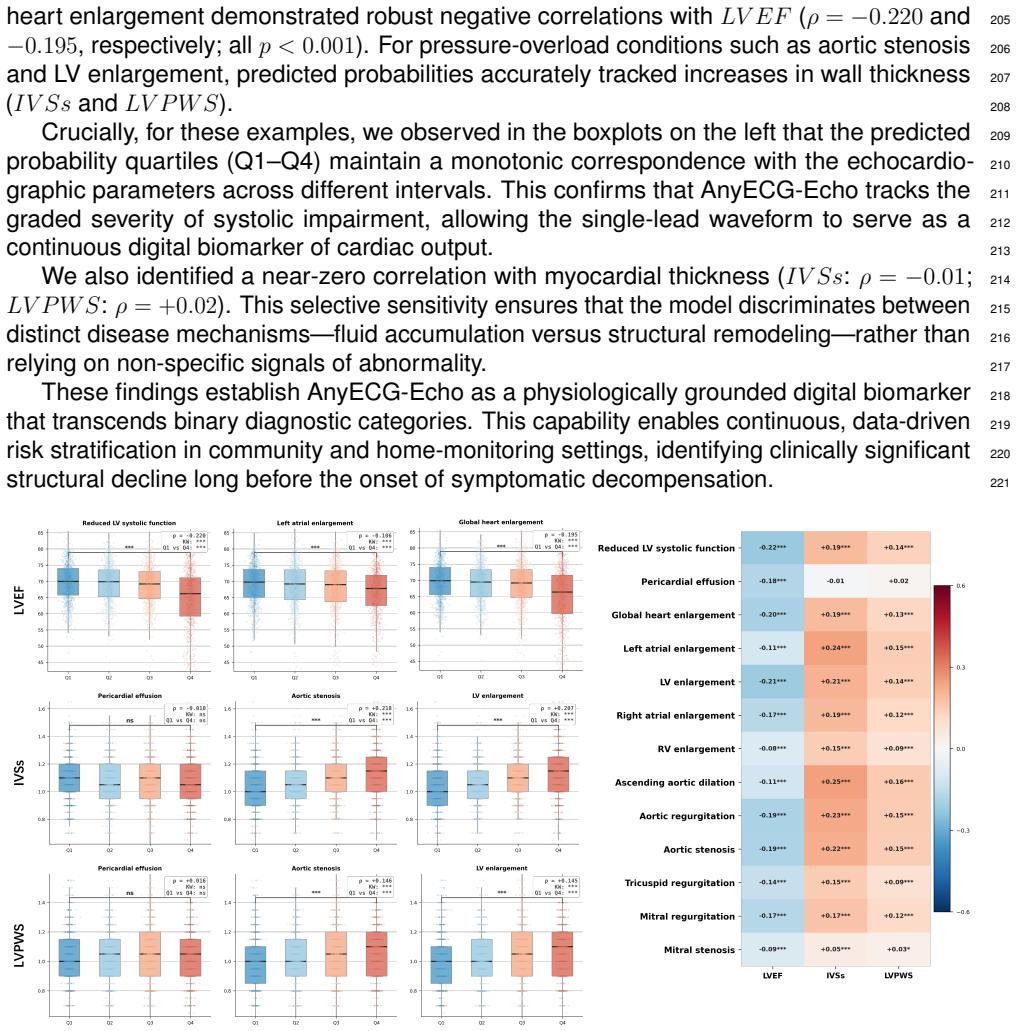
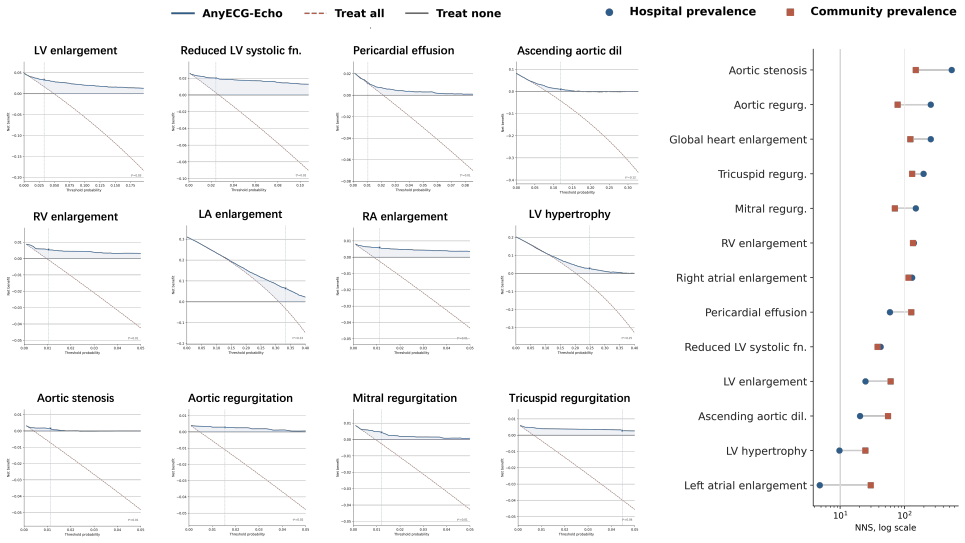
AnyECG-Echo advances single-lead ECG to echo-report supervision by demonstrating high AUROC across 13 SHD subtypes in a total of 25,222 patients, successful transfer to an external cohort, and model outputs that function as physiologically grounded digital biomarkers tracking objective metrics such as LVEF and myocardial wall thickness.
What carries the argument
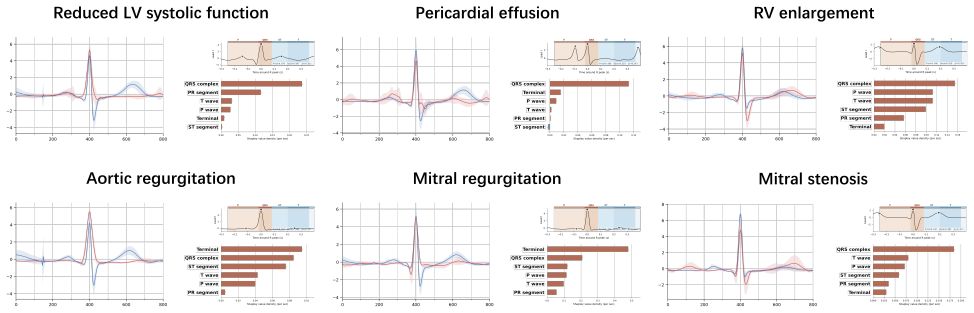
AnyECG-Echo framework that trains single-lead ECG models under supervision from echocardiography reports to classify 13 SHD subtypes, paired with dual-axis interpretability that combines electrophysiology-grounded Shapley attribution and emergent correlations to quantitative echo measurements.
If this is right
- The model achieves AUROC 0.866-0.924 for reduced left ventricular systolic function and 0.877-0.931 for global heart enlargement across validation cohorts.
- Diagnostic coverage spans 13 subtypes across myocardial, chamber, valvular, and great-vessel pathologies.
- Model outputs align with established physiological traits and track quantitative measurements including LVEF and myocardial wall thickness.
- External cohort validation supports generalization beyond the training health system.
Where Pith is reading between the lines
- Wearable single-lead ECG could support continuous rather than snapshot screening, allowing earlier detection before overt heart failure symptoms appear.
- The same supervision approach might transfer to other ECG-derived tasks if comparable report labels become available at scale.
- Population-level deployment would shift initial cardiac evaluation away from imaging centers toward consumer devices.
Load-bearing premise
Echo reports supply accurate fine-grained labels for the 13 SHD subtypes that transfer to a new geographic cohort without major domain shift or label noise.
What would settle it
Direct comparison of AnyECG-Echo predictions against independent echocardiography labels in a fresh external population that yields AUROC below 0.75 for several high-impact subtypes such as reduced LV systolic function or mitral stenosis.
Figures

read the original abstract
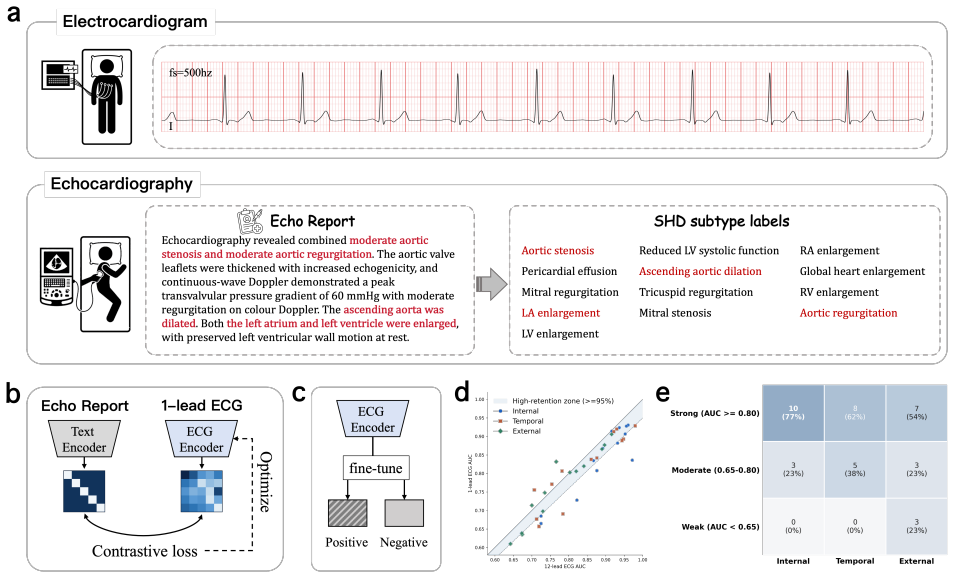
Structural heart disease (SHD) is a primary driver of heart failure and cardiovascular mortality, yet early detection remains constrained by the limited accessibility of echocardiography. While single-lead electrocardiogram (ECG) is ubiquitous through wearables, existing AI screening models often depend on 12-lead inputs, generalize poorly across institutions, or require massive, condition-specific labeled datasets. Recent work has demonstrated the feasibility of contrastive pre-training between single-lead ECGs and echocardiography reports within a single health system. Here, we present AnyECG-Echo, a framework that advance this paradigm toward clinical translation through three key developments: (1) evaluation in a geographically independent external cohort (n = 16,621); (2) diagnostic coverage of 13 fine-grained SHD subtypes spanning myocardial, chamber, valvular, and great-vessel pathologies; and (3) dual-axis mechanistic interpretability combining electrophysiology-grounded Shapley attribution with emergent correlations to quantitative measurements. Across validation cohorts totaling n = 25,222, the model demonstrated high AUROC for high-impact subtypes, including reduced left ventricular systolic function (AUROC 0.866-0.924), global heart enlargement (0.877-0.931), and mitral stenosis (0.836-0.906). Furthermore, we successfully validated the alignment of model outputs with established medical physiological traits, thereby enhancing interpretability. Notably, we discovered that AnyECG-Echo's outputs function as physiologically grounded digital biomarkers that accurately track objective metrics such as LVEF and myocardial wall thickness. These findings prove that wearable single-lead ECGs can effectively detect fine-grained structural heart disease, offering a practical solution for population-scale screening.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper introduces AnyECG-Echo, a framework that uses contrastive pre-training on single-lead ECGs paired with echocardiography reports to detect 13 fine-grained structural heart disease (SHD) subtypes (myocardial, chamber, valvular, great-vessel). It evaluates performance on internal and geographically independent external cohorts (total n=25,222), reporting AUROCs of 0.866-0.924 for reduced LV systolic function, 0.877-0.931 for global enlargement, and 0.836-0.906 for mitral stenosis, plus correlations between model outputs and quantitative echo metrics such as LVEF and wall thickness.
Significance. If the central results hold after addressing label validation, the work would be significant for demonstrating that ubiquitous wearable single-lead ECGs can screen for multiple SHD subtypes at population scale, extending prior single-institution contrastive work via external validation and dual-axis interpretability (Shapley attribution plus physiological correlations). External cohort testing and coverage of 13 subtypes are clear strengths.
major comments (2)
- [Abstract/Methods] Abstract and Methods: The central claim that echo-report supervision yields reliable fine-grained labels for 13 SHD subtypes (and transfers to the external cohort of n=16,621) is load-bearing for all reported AUROCs, yet the manuscript supplies no quantitative validation of label fidelity such as NLP extraction accuracy, inter-annotator agreement on report parsing, or comparison against re-read echocardiograms.
- [Abstract] Abstract: No information is provided on model architecture, training loss, data filtering rules, or class-imbalance handling; without these details it is impossible to determine whether the AUROCs reflect true ECG–pathology signal or post-hoc choices.
minor comments (1)
- [Abstract] Abstract: The phrasing 'These findings prove that wearable single-lead ECGs can effectively detect...' overstates an empirical result; 'support the feasibility of' would be more proportionate.
Simulated Author's Rebuttal
We thank the referee for their constructive and detailed feedback. The comments highlight important areas for improving transparency and rigor. We respond point-by-point below and have revised the manuscript accordingly where feasible.
read point-by-point responses
-
Referee: [Abstract/Methods] Abstract and Methods: The central claim that echo-report supervision yields reliable fine-grained labels for 13 SHD subtypes (and transfers to the external cohort of n=16,621) is load-bearing for all reported AUROCs, yet the manuscript supplies no quantitative validation of label fidelity such as NLP extraction accuracy, inter-annotator agreement on report parsing, or comparison against re-read echocardiograms.
Authors: We agree this is a substantive point. The manuscript describes the NLP-based label extraction from echo reports in Methods but does not include quantitative fidelity metrics. In revision we will add a new Methods subsection reporting NLP validation on a held-out set of reports (including extraction accuracy and inter-annotator agreement) together with a supplementary table correlating extracted labels against quantitative echo measurements. This directly addresses label reliability for both internal and external cohorts. revision: yes
-
Referee: [Abstract] Abstract: No information is provided on model architecture, training loss, data filtering rules, or class-imbalance handling; without these details it is impossible to determine whether the AUROCs reflect true ECG–pathology signal or post-hoc choices.
Authors: We accept that the abstract should supply sufficient methodological context. Although full details appear in Methods, we will revise the abstract to include a concise description of the dual-encoder contrastive architecture, InfoNCE loss, ECG quality filtering criteria, and class-balanced sampling. This change improves immediate assessability of the reported AUROCs without altering the abstract's length constraints. revision: yes
Circularity Check
No circularity; external validation independent of training labels
full rationale
The derivation chain consists of standard supervised/contrastive training on echo-report labels followed by AUROC evaluation on a geographically independent held-out cohort (n=16,621). No equations, fitted parameters, or self-citations reduce the reported performance metrics to the training inputs by construction. The framework cites prior feasibility work but does not rely on author-overlapping uniqueness theorems or ansatzes for its central claims. Performance is measured against external labels rather than being defined in terms of the model's own outputs or fitted values.
Axiom & Free-Parameter Ledger
free parameters (1)
- neural network parameters
axioms (1)
- domain assumption Echocardiography reports constitute accurate fine-grained labels for 13 SHD subtypes
Reference graph
Works this paper leans on
-
[1]
Dhingra, L.S., Aminorroaya, A., Sangha, V., Pedroso, A.F ., Shankar, S.V., Coppi, A., 453 Foppa, M., Brant, L.C., Barreto, S.M., Ribeiro, A.L.P . et al. (2025). Ensemble deep 454 learning algorithm for structural heart disease screening using electrocardiographic 455 images: Present shd. Journal of the American College of Cardiology85, 1302–1313.456
2025
-
[2]
Aminorroaya, A., Dhingra, L.S., Pedroso, A.F ., Shankar, S.V., Coppi, A., Khunte, A., 457 Foppa, M., Brant, L.C., Barreto, S.M., Ribeiro, A.L.P . et al. (2025). Development and 458 multinational validation of an ensemble deep learning algorithm for detecting and pre- 459 dicting structural heart disease using noisy single-lead electrocardiograms. European...
2025
-
[3]
Taggart, C., Ferry, A., Barker, S., Williams, K., Souter, G., Bularga, A., Wereski, R., 462 McDermott, M.J., Williams, M.C., Boeddinghaus, J. et al. (2025). Targeting investigation 463 and treatment in type 2 myocardial infarction: a pilot randomized controlled trial. JACC: 464 Advances4, 101738. 465
2025
-
[4]
Ortiz-Garrido, A., Piñero-Uribe, I., Líebana-Carpio, L., Cano-Nieto, J., Gaitan-Román, 466 D., and Picazo-Angelín, B. (2025). Double chambered left ventricle: an incidental rare 467 congenital heart disease. report of a case within the context of a literature review. The 468 International Journal of Cardiovascular Imaging pp. 1–6.469
2025
-
[5]
Unger, P ., Galloo, X., and Pibarot, P . (2025). Mixed valvular heart disease: diagnosis 470 and management. European Heart Journal46, 2261–2274.471
2025
-
[6]
472 (2023)
Y ao, Z., Xie, W., Zhang, J., Yuan, H., Huang, M., Shi, Y ., Xu, X., and Zhuang, J. 472 (2023). Graph matching and deep neural networks based whole heart and great vessel 473 segmentation in congenital heart disease. Scientific reports13, 7558.474
2023
-
[7]
Lee, J.C., Geske, J.B., Narang, A., Khalique, O.K., Choi, A.D., Sun, Y .P ., Cavalcante,475 J.L., Pinto, D.S., Gafoor, S.A., Jagasia, D.H. et al. (2023). Structural heart imaging 476 survey highlights: training, challenges, and practice patterns in interventional imaging. 477 Cardiovascular Imaging16, 255–258. 478
2023
-
[8]
Antoniades, C., and Chan, K. (2025). Scalable screening for structural heart disease: 479 promises from artificial intelligence-electrocardiogram tools. Oxford University Press UK. 480
2025
-
[9]
Hickson, L.J., Negrotto, S.M., Onuigbo, M., Scott, C.G., Rule, A.D., Norby, S.M., Albright, 481 R.C., Casey, E.T., Dillon, J.J., Pellikka, P .A. et al. (2016). Echocardiography criteria for482 structural heart disease in patients with end-stage renal disease initiating hemodialysis. 483 Journal of the American College of Cardiology67, 1173–1182.484 17
2016
-
[10]
Jiang, H., Wang, T., Sun, Z., Wang, Y ., Yue, Y ., Sun, Y ., Jia, N., Li, M., Luo, S., Song,485 S. et al. (2025). Ultrasep: Sequence-aware pre-training for echocardiography probe 486 movement guidance. Pattern Recognition pp. 112600.487
2025
-
[11]
Krammel, M., Hamp, T., Hafner, C., Magnet, I., Poppe, M., and Marhofer, P . (2023). Fea-488 sibility of resuscitative transesophageal echocardiography at out-of-hospital emergency 489 scenes of cardiac arrest. Scientific Reports13, 20085.490
2023
-
[12]
Palermi, S., Vecchiato, M., Ng, F .S., Attia, Z., Cho, Y ., Anselmino, M., De Ferrari, 491 G.M., Saglietto, A., Sau, A., Chiu, I.M. et al. (2025). Artificial intelligence and the 492 electrocardiogram: A modern renaissance. European Journal of Internal Medicine.493
2025
-
[13]
Alimbayeva, Z.N., Alimbayev, C.A., Bayanbay, N.A., Ozhikenov, K.A., Bodin, O.N., and 494 Mukazhanov, Y .B. (2022). Portable ecg monitoring system. International Journal of 495 Advanced Computer Science and Applications13. 496
2022
-
[14]
Wang, R., Veera, S.C.M., Asan, O., and Liao, T. (2024). A systematic review on the 497 use of consumer-based ecg wearables on cardiac health monitoring. IEEE Journal of 498 Biomedical and Health Informatics28, 6525–6537. 499
2024
-
[15]
Lin, S., Li, Z., Wu, Q., Chen, Y ., Y ang, Y ., and Zhao, H. (2026). A self-supervised 500 electrocardiogram foundation model for empowering cardiovascular disease prediction 501 and genetic factor discovery. Nature Communications.502
2026
-
[16]
Zhu, H., Luo, Q., Wang, Y ., Maimaiti, M., Zhang, H., Xiong, Y ., Ruan, C., Wang, J., Liu,503 Y ., Zhou, M. et al. (2026). Artificial intelligence-enabled 8-channel ecg diagnosing of 504 abnormalities with wide qrs complexes: a cohort study. Health Data Science.505
2026
-
[17]
Poterucha, T.J., Jing, L., Ricart, R.P ., Adjei-Mosi, M., Finer, J., Hartzel, D., Kelsey, C.,506 Long, A., Rocha, D., Ruhl, J.A. et al. (2025). Detecting structural heart disease from 507 electrocardiograms using ai. Nature644, 221–230. 508
2025
-
[18]
Hughes, J.W., Jing, L., Finer, J., Hartzel, D., Kelsey, C., Long, A., Rocha, D., Ruhl, J., 509 Poterucha, T., and Elias, P . (2026). Echonext-mini: A dataset and baseline ai model for 510 detecting structural heart disease from electrocardiograms. NEJM AI pp. AIdbp2500516. 511
2026
-
[19]
Liang, Y ., Sau, A., Zeidaabadi, B., Barker, J., Patlatzoglou, K., Pastika, L., Sieliwonczyk, 512 E., Whinnett, Z., Peters, N.S., Yu, Z. et al. (2025). Artificial intelligence-enhanced 513 electrocardiography to predict regurgitant valvular heart diseases: an international study. 514 European Heart Journal46, 4823–4837. 515
2025
-
[20]
Knight, E., Oikonomou, E.K., Aminorroaya, A., Pedroso, A.F ., and Khera, R. (2026). 516 Wearable-echo-fm: an ecg echo foundation model for 1-lead electrocardiography. Euro- 517 pean Heart Journal-Digital Health7, ztag049. 518
2026
-
[21]
van der Valk, V., Atsma, D., Scherptong, R., and Staring, M. (2025). Explainable ecg 519 analysis by explicit information disentanglement with vaes. IEEE Transactions on 520 Biomedical Engineering. 521
2025
-
[22]
Lang, R.M., Badano, L.P ., Mor-Avi, V., Afilalo, J., Armstrong, A., Ernande, L., Flach- 522 skampf, F .A., Foster, E., Goldstein, S.A., Kuznetsova, T. et al. (2015). Recommendations523 for cardiac chamber quantification by echocardiography in adults: an update from the 524 american society of echocardiography and the european association of cardiovascular...
2015
-
[23]
Zoghbi, W.A., Adams, D., Bonow, R.O., Enriquez-Sarano, M., Foster, E., Grayburn, 527 P .A., Hahn, R.T., Han, Y ., Hung, J., Lang, R.M. et al. (2017). Recommendations for 528 noninvasive evaluation of native valvular regurgitation: a report from the american 529 society of echocardiography developed in collaboration with the society for cardiovascular 530 ...
2017
-
[24]
Baumgartner, H., Hung, J., Bermejo, J., Chambers, J.B., Edvardsen, T., Goldstein, 532 S., Lancellotti, P ., LeFevre, M., Miller Jr, F ., Otto, C.M. et al. (2017). Recommenda- 533 tions on the echocardiographic assessment of aortic valve stenosis: a focused update 534 from the european association of cardiovascular imaging and the american society of 535 e...
2017
-
[25]
(2023).537 Medcpt: Contrastive pre-trained transformers with large-scale pubmed search logs for 538 zero-shot biomedical information retrieval
Jin, Q., Kim, W., Chen, Q., Comeau, D.C., Y eganova, L., Wilbur, W.J., and Lu, Z. (2023).537 Medcpt: Contrastive pre-trained transformers with large-scale pubmed search logs for 538 zero-shot biomedical information retrieval. Bioinformatics39, btad651.539
2023
-
[26]
Mensah, G.A., Fuster, V., Murray, C.J., Roth, G.A., Abate, Y .H., Abbasian, M., Abd- 540 Allah, F ., Abdollahi, A., Abdollahi, M., Abdulah, D.M. et al. (2023). Global burden of 541 cardiovascular diseases and risks, 1990-2022. Journal of the American College of 542 Cardiology82, 2350–2473. 543
2023
-
[27]
Mosterd, A., Hoes, A., De Bruyne, M., Deckers, J., Linker, D., Hofman, A., and Grobbee, 544 D. (1999). Prevalence of heart failure and left ventricular dysfunction in the general 545 population; the rotterdam study. European heart journal20, 447–455.546
1999
-
[28]
Raymond, I., Pedersen, F ., Steensgaard-Hansen, F ., Green, A., Busch-Sorensen, M.,547 Tuxen, C., Appel, J., Jacobsen, J., Atar, D., and Hildebrandt, P . (2003). Prevalence of 548 impaired left ventricular systolic function and heart failure in a middle aged and elderly 549 urban population segment of copenhagen. Heart89, 1422–1429.550
2003
-
[29]
Sahiti, F ., Cejka, V., Schmidbauer, L., Albert, J., Kerwagen, F ., Frantz, S., Gelbrich, G.,551 Heuschmann, P .U., Störk, S., and Morbach, C. (2024). Prognostic utility of pericardial 552 effusion in the general population: findings from the staab cohort study. Journal of the 553 American Heart Association13, e035549. 554
2024
-
[30]
Ou, Q., Chen, Y ., Yu, S., Guo, X., Zhao, H., and Sun, Y . (2016). Prevalence of left atrial555 enlargement and its risk factors in general chinese population. BMC cardiovascular 556 disorders16, 53. 557
2016
-
[31]
Vasan, R.S., Larson, M.G., Benjamin, E.J., Evans, J.C., and Levy, D. (1997). Left 558 ventricular dilatation and the risk of congestive heart failure in people without myocardial 559 infarction. New England Journal of Medicine336, 1350–1355.560
1997
-
[32]
Nkomo, V.T., Gardin, J.M., Skelton, T.N., Gottdiener, J.S., Scott, C.G., and Enriquez- 561 Sarano, M. (2006). Burden of valvular heart diseases: a population-based study. The 562 lancet368, 1005–1011. 563
2006
-
[33]
d’Arcy, J.L., Coffey, S., Loudon, M.A., Kennedy, A., Pearson-Stuttard, J., Birks, J., 564 Frangou, E., Farmer, A.J., Mant, D., Wilson, J. et al. (2016). Large-scale community 565 echocardiographic screening reveals a major burden of undiagnosed valvular heart 566 disease in older people: the oxvalve population cohort study. European heart journal37, 567 3...
2016
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.