Analytical and Cross-Sectional Clinical Validity of a Smartphone-Based U-Turn Test in Multiple Sclerosis
Pith reviewed 2026-05-17 01:11 UTC · model grok-4.3
The pith
A smartphone-based U-turn test accurately measures turn speed in people with multiple sclerosis across lab and home settings.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
The U-Turn Test computes median turn speed from smartphone inertial sensors during a 180-degree pivot and achieves turn detection F1 scores above 95 percent versus motion capture across wear locations. Turn speed values agree closely with the laboratory reference (ICC 0.87-0.92) with negligible bias, remain similar between supervised (1.44 rad/s) and unsupervised (1.47 rad/s) conditions, reach test-retest reliability above 0.90 when two or more home tests are averaged, and show strong negative correlations with the Timed 25-Foot Walk (rho = -0.79), EDSS (rho = -0.75), ambulation score (rho = -0.73), MSWS-12 (rho = -0.65), and ABC scale (rho = -0.61).
What carries the argument
The U-Turn Test (UTT), a smartphone-based maneuver that records sensor data during a single 180-degree turn and derives median angular speed as the balance metric.
If this is right
- Turn detection remains accurate (F1 > 95 percent) regardless of smartphone placement on the body.
- Speed measurements obtained at home match supervised laboratory values with minimal bias.
- Averaging two or more unsupervised tests yields test-retest reliability above 0.90.
- Turn speed supplies dynamic-balance information that is not fully captured by standard clinical scales.
- The method is positioned for use in future multiple sclerosis clinical trials that require remote data collection.
Where Pith is reading between the lines
- Home-based testing could support more frequent monitoring of mobility changes between clinic visits.
- The single-belt placement may lower barriers for patients who find multiple sensors or lab travel difficult.
- Longitudinal follow-up could test whether turn-speed changes predict falls or respond to physical therapy.
- Pairing UTT data with other smartphone gait metrics might yield a richer remote mobility profile.
Load-bearing premise
The premise that cross-sectional correlations with EDSS and T25FW demonstrate specific validity for dynamic balance rather than simply tracking overall disability severity.
What would settle it
A study in which unsupervised home UTT turn speeds show low agreement with lab measures or lose their correlation with balance outcomes after statistical adjustment for overall EDSS level would falsify the clinical-validity claim.
Figures
read the original abstract
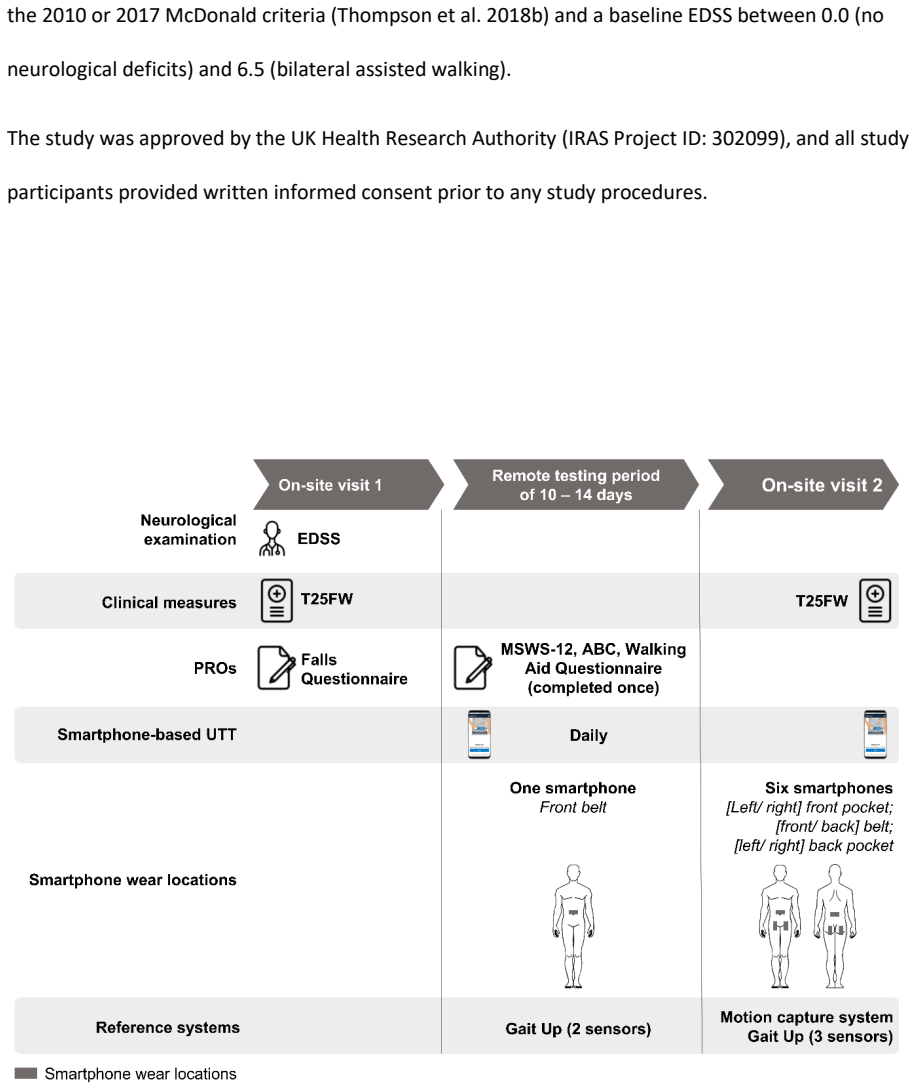
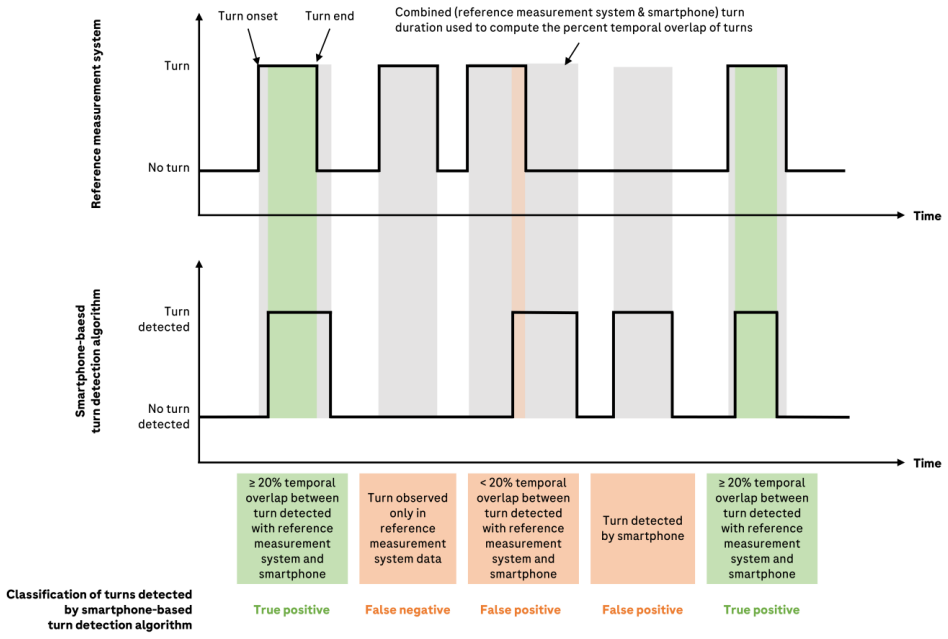
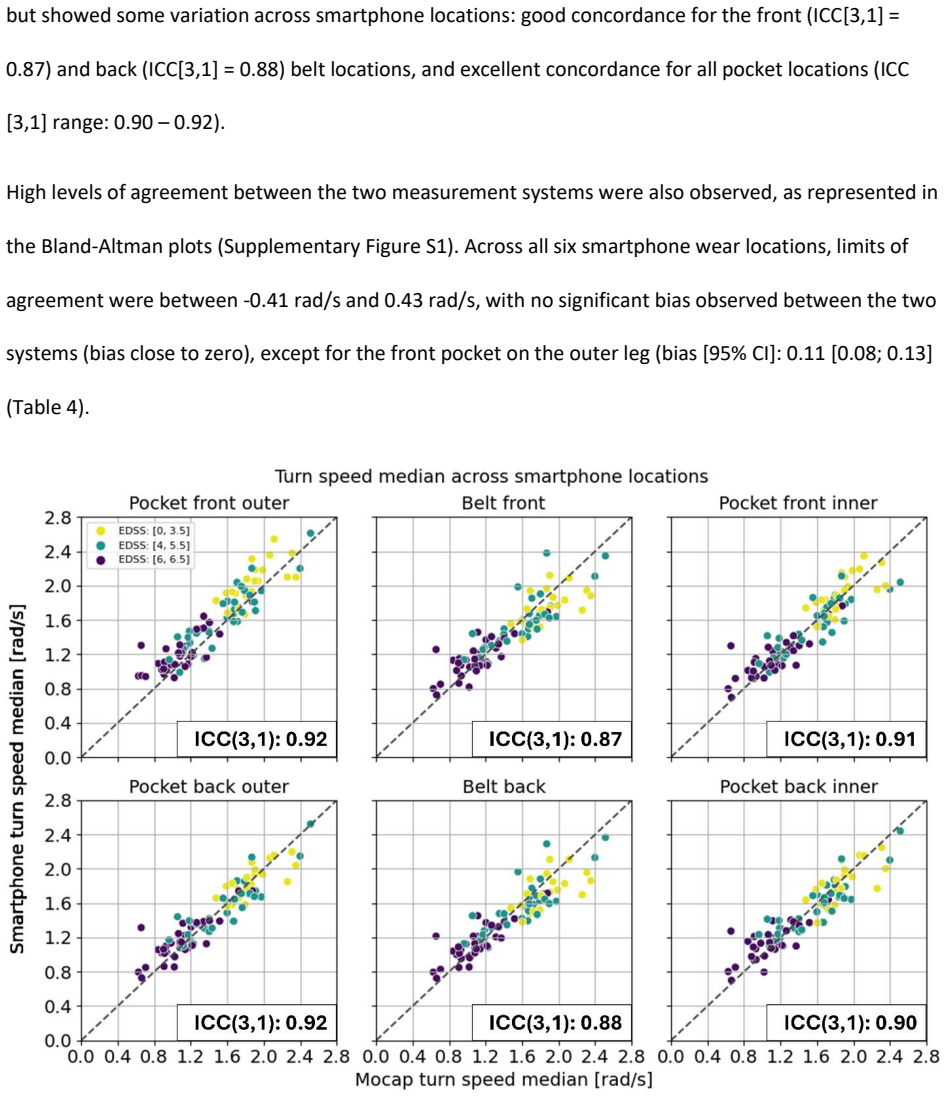
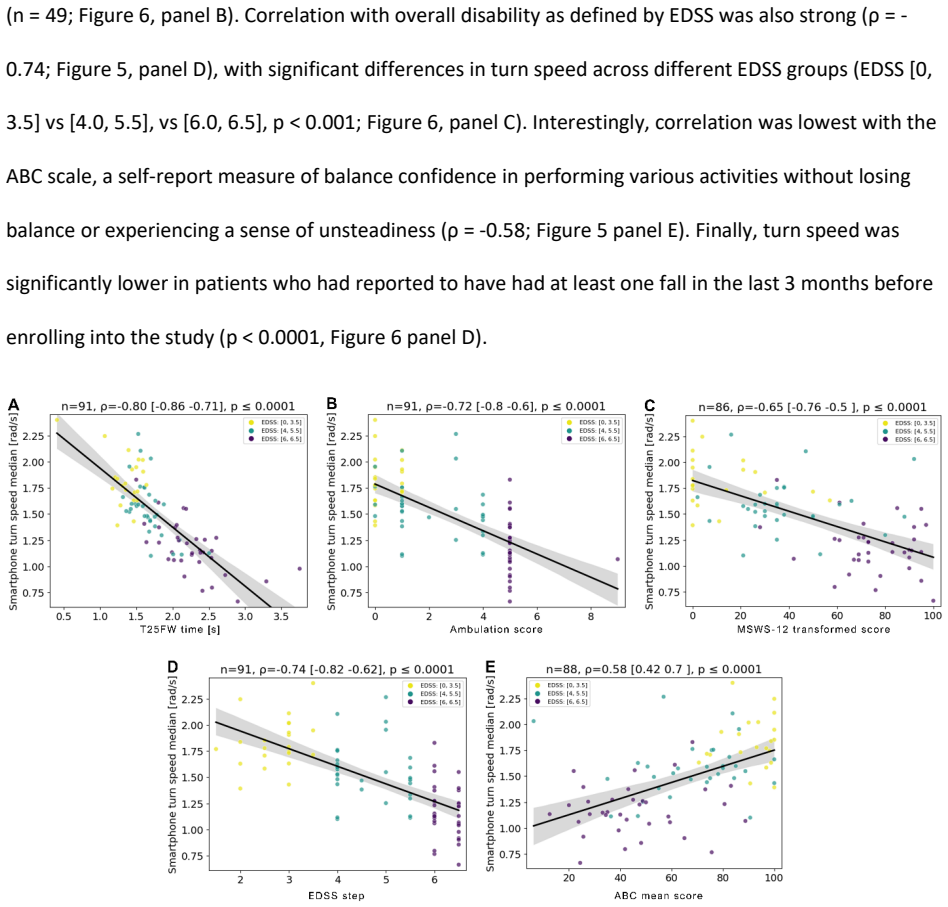
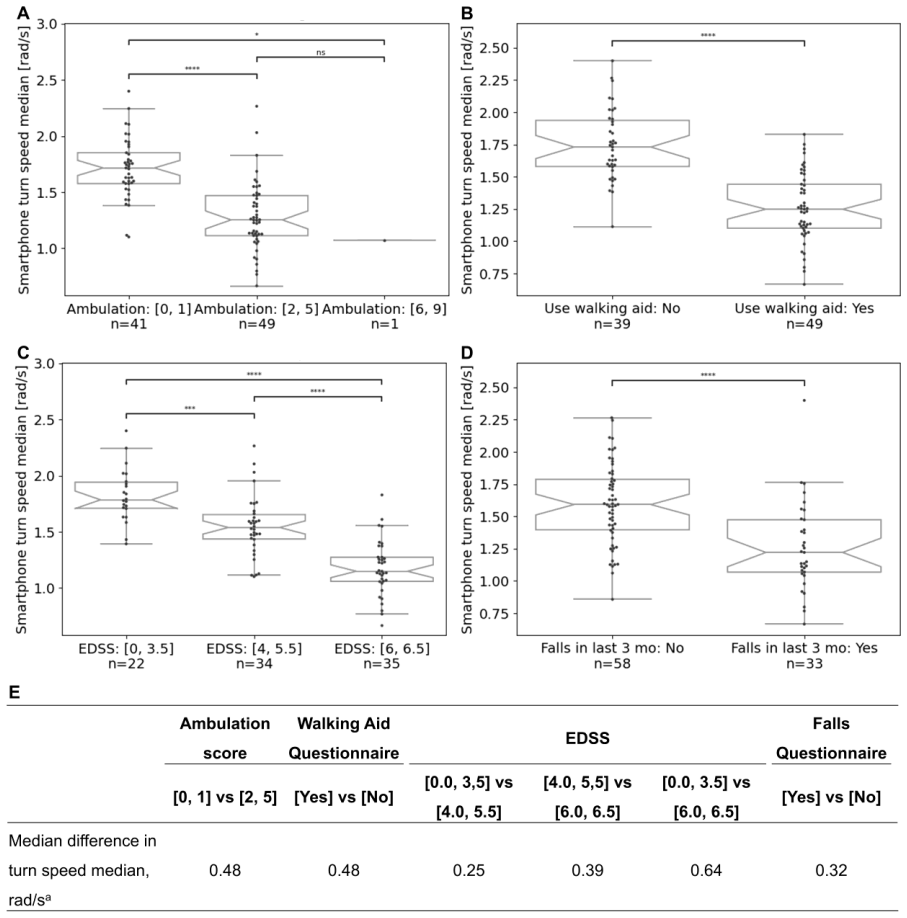
Background: Gait and balance impairment can profoundly impact people with multiple sclerosis (PwMS). Objectives: To evaluate the analytical and clinical validity of the U-Turn Test (UTT), a smartphone-based assessment of dynamic balance in PwMS. Methods: The GaitLab study (ISRCTN15993728) enrolled adult PwMS (EDSS 0.0-6.5). PwMS performed the UTT in a gait laboratory (supervised) using 6 smartphones at different wear locations and daily during a two-week remote period (unsupervised) using one smartphone (belt front). Median turn speed was computed per UTT. In the supervised setting, turn detection accuracy of smartphones was compared to motion capture (mocap) via F1 scores. Agreement between smartphone- and mocap-derived turn speed was assessed by Bland-Altman and ICC(3,1). In the unsupervised setting, test-retest reliability (ICC[2,1]) and correlations with Timed 25-Foot Walk (T25FW), EDSS, Ambulation Score, 12-item Multiple Sclerosis Walking Scale (MSWS-12), and Activities-specific Balance Confidence scale (ABC) were evaluated. Results: Ninety-six PwMS were included. Turn speed was comparable across supervised (1.44 rad/s) and unsupervised settings (1.47 rad/s). In the supervised setting, turn detection was highly accurate (F1 >95% across wear locations). Turn speed agreement with mocap was high (ICC[3,1]: 0.87-0.92), with minimal bias (-0.04 to 0.11 rad/s). Unsupervised test-retest reliability (ICC[2,1]) was >0.90 when aggregating >=2 tests. Turn speed correlated with T25FW (rho=-0.79), EDSS (rho=-0.75), Ambulation score (rho=-0.73), MSWS-12 (rho=-0.65), and ABC (rho=-0.61). Conclusion: The UTT accurately and reproducibly measures turn speed across wear locations and settings, providing complementary dynamic balance insights to clinical measures and showing potential for use in multiple sclerosis trials.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper evaluates the analytical and clinical validity of a smartphone-based U-Turn Test (UTT) for dynamic balance in people with multiple sclerosis (PwMS, EDSS 0-6.5). In the supervised GaitLab setting with 96 participants and 6 phone wear locations, it reports high turn detection accuracy versus motion capture (F1 >95%), strong agreement on turn speed (ICC[3,1] 0.87-0.92, minimal bias), and comparable median turn speeds (~1.44-1.47 rad/s) to the unsupervised home setting (single belt-front placement over 2 weeks). Unsupervised test-retest reliability exceeds ICC[2,1] >0.90 when aggregating >=2 tests, with moderate-to-strong Spearman correlations to T25FW (rho=-0.79), EDSS (rho=-0.75), ambulation score (rho=-0.73), MSWS-12 (rho=-0.65), and ABC (rho=-0.61).
Significance. If the results hold after addressing incremental validity, the work demonstrates a feasible, reproducible smartphone method for quantifying turning performance that could complement existing MS outcome measures in trials and remote monitoring. Strengths include multi-location analytical validation against mocap ground truth, unsupervised reliability data, and direct correlation with established clinical scales using standard statistics (Bland-Altman, ICC, Spearman).
major comments (2)
- [Results] Results section (correlations paragraph): The strong correlations with T25FW (rho=-0.79) and EDSS (rho=-0.75) are reported, but the central claim that UTT 'provides complementary dynamic balance insights' is not supported by evidence that turn speed explains unique variance beyond straight-line gait speed. Partial correlations or hierarchical regression (incremental R² after controlling for T25FW) are needed to substantiate independence from overall mobility.
- [Methods] Methods section (study population and procedures): The cohort of 96 PwMS is described at a high level, but exact exclusion criteria, full demographics (age, sex, disease duration, EDSS distribution), and handling of potential selection bias or dropouts are insufficiently detailed to evaluate generalizability and interpret the unsupervised home data.
minor comments (2)
- [Abstract] Abstract and Results: Clarify the exact definition and computation of 'median turn speed' per UTT trial, including any filtering or outlier handling for both supervised and unsupervised data.
- [Results] Results: Report the number of participants contributing to each correlation and reliability analysis to allow assessment of missing data impact.
Simulated Author's Rebuttal
We thank the referee for the constructive and detailed feedback on our manuscript evaluating the smartphone-based U-Turn Test in multiple sclerosis. The comments have identified important areas for strengthening the reporting and interpretation. We address each major comment below and will incorporate revisions accordingly.
read point-by-point responses
-
Referee: [Results] Results section (correlations paragraph): The strong correlations with T25FW (rho=-0.79) and EDSS (rho=-0.75) are reported, but the central claim that UTT 'provides complementary dynamic balance insights' is not supported by evidence that turn speed explains unique variance beyond straight-line gait speed. Partial correlations or hierarchical regression (incremental R² after controlling for T25FW) are needed to substantiate independence from overall mobility.
Authors: We agree that the manuscript's claim of complementary insights would be more robust with evidence of incremental validity. The current correlations demonstrate associations but do not isolate the unique contribution of turn speed beyond overall gait speed. In the revised manuscript, we will add partial Spearman correlation analyses between median turn speed and the clinical measures (EDSS, ambulation score, MSWS-12, ABC), controlling for T25FW performance. We will also consider a hierarchical regression approach if appropriate. These results will be reported, and the discussion and conclusion will be updated to reflect whether turn speed explains additional variance. revision: yes
-
Referee: [Methods] Methods section (study population and procedures): The cohort of 96 PwMS is described at a high level, but exact exclusion criteria, full demographics (age, sex, disease duration, EDSS distribution), and handling of potential selection bias or dropouts are insufficiently detailed to evaluate generalizability and interpret the unsupervised home data.
Authors: We acknowledge that the participant description in the Methods section is summarized at a high level and lacks sufficient granularity. Although the manuscript reports that 96 PwMS were included, we will revise this section to include the precise inclusion and exclusion criteria, comprehensive demographic characteristics (e.g., mean age and standard deviation, sex distribution, mean disease duration, EDSS range and distribution), details on recruitment, any participants who were excluded or dropped out, and explicit discussion of potential selection bias and its implications for the unsupervised data. This expanded reporting will improve transparency and allow readers to better assess generalizability. revision: yes
Circularity Check
No circularity: purely empirical validation with external benchmarks
full rationale
The manuscript reports an empirical study validating smartphone-derived turn speed against motion-capture ground truth (F1 scores, Bland-Altman, ICC[3,1]) and against established clinical scales (Spearman correlations with T25FW, EDSS, etc.). No equations, first-principles derivations, fitted parameters re-labeled as predictions, or self-citation chains appear in the provided text or abstract. All reported quantities are direct statistical comparisons to independent external references; the central claims therefore do not reduce to their own inputs by construction.
Axiom & Free-Parameter Ledger
axioms (2)
- domain assumption EDSS, T25FW, MSWS-12 and ABC are valid and relevant reference measures for MS ambulation and balance.
- standard math ICC and Bland-Altman methods appropriately quantify agreement and reliability for continuous turn-speed data.
Reference graph
Works this paper leans on
-
[1]
Adusumilli G, Lancia S, Levasseur VA, Amblee V, Orchard M, Wagner JM, et al. Turning is an important marker of balance confidence and walking limitation in persons with multiple sclerosis. PLOS ONE. 2018;13(6):e0198178. doi: 10.1371/journal.pone.0198178. 36 Anastasi D, Lencioni T, Carpinella I, Castagna A, Crippa A, Gervasoni E, et al. Dynamic balance dur...
-
[2]
37 Crenna P, Carpinella I, Rabuffetti M, Calabrese E, Mazzoleni P, Nemni R, et al
doi: 10.7224/1537-2073.2020-014. 37 Crenna P, Carpinella I, Rabuffetti M, Calabrese E, Mazzoleni P, Nemni R, et al. The association between impaired turning and normal straight walking in Parkinson's disease. Gait Posture. 2007;26(2):172-8. doi: 10.1016/j.gaitpost.2007.04.010. Cumming RG, Klineberg RJ. Fall Frequency and Characteristics and the Risk of Hi...
-
[3]
38 Jawad A, Baattaiah BA, Alharbi MD, Chevidikunnan MF, Khan F. Factors contributing to falls in people with multiple sclerosis: The exploration of the moderation and mediation effects. Mult Scler Relat Disord. 2023;76:104838. doi: 10.1016/j.msard.2023.104838. Kappos L. Neurostatus scoring definitions: Version 04/10.2. Available via: https://www.neurostat...
-
[4]
Metrics for evaluaƟng 3D medical image segmentaƟon: analysis, selecƟon, and tool
Taha AA, Hanbury A. Metrics for evaluating 3D medical image segmentation: analysis, selection, and tool. BMC Med Imaging. 2015;15:29. doi: 10.1186/s12880-015-0068-x. Thompson AJ, Baranzini SE, Geurts J, Hemmer B, Ciccarelli O. Multiple sclerosis. Lancet. 2018a;391(10130):1622-36. doi: 10.1016/S0140-6736(18)30481-1 41 Thompson AJ, Banwell BL, Barkhof F, Ca...
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.