Planned, delivered and variable RBE dose difference analysis for a patient cohort with base-of-tongue cancer treated with IMPT
Pith reviewed 2026-06-27 10:22 UTC · model grok-4.3
The pith
Planned and delivered proton doses differ substantially for base-of-tongue cancer due to anatomy changes, and variable RBE influences plan evaluation.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
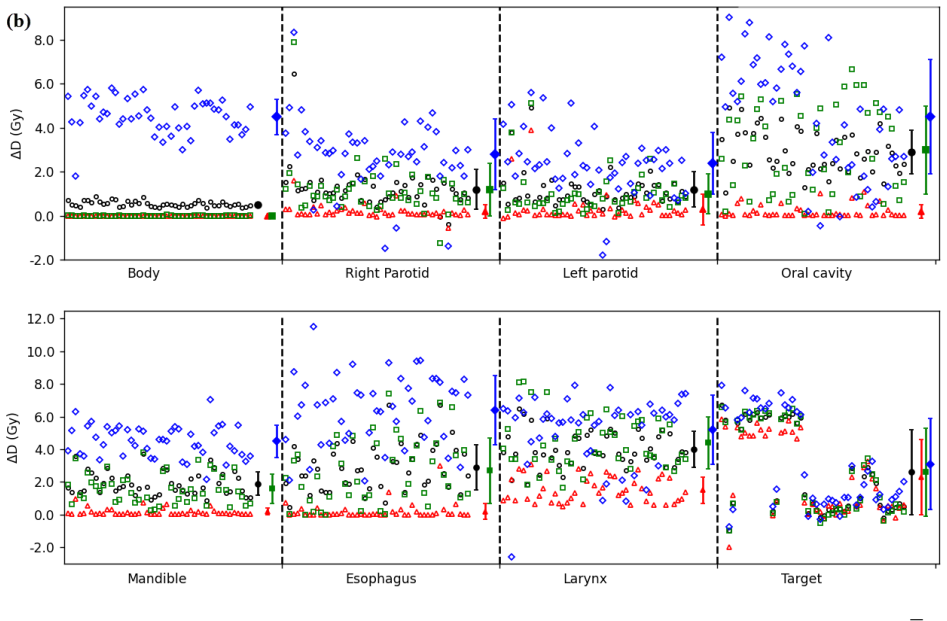
The authors analyze a patient cohort with base-of-tongue cancer treated by IMPT to measure differences between planned and delivered doses while incorporating variable RBE. They observe that anatomy changes can produce large discrepancies and that variable RBE exceeds 1.1 particularly at beam ends, thereby altering plan evaluation, in the absence of clinical tools for routine assessment of these quantities.
What carries the argument
Comparison of planned versus delivered dose distributions using variable RBE models across a base-of-tongue cancer cohort.
If this is right
- Clinics lack installed tools for evaluating delivered versus planned dose differences in proton therapy.
- Head and neck patients suffer the most anatomy changes over long treatment courses and difficulty eating.
- Variable RBE values larger than 1.1 at beam ends change how treatment plans are evaluated.
- The constant RBE of 1.1 may not capture the full biological effect in these cases.
Where Pith is reading between the lines
- Similar dose-difference tracking could be applied to other treatment sites to identify where adaptive replanning is most needed.
- Incorporating variable RBE into routine evaluation might shift estimates of normal-tissue complication probabilities in head and neck cases.
- The absence of clinical tools noted in the study points to a practical barrier that future software development could address.
Load-bearing premise
The selected base-of-tongue cancer cohort experiences the most anatomy changes compared with other treatment sites and the analysis methods accurately capture delivered dose without unstated modeling errors.
What would settle it
Direct comparison of repeated imaging and dose recalculation for the same patients showing delivered doses match planned doses within a small margin regardless of anatomy shifts, or outcome data showing identical clinical results under constant and variable RBE.
Figures
read the original abstract
Background: To our knowledge, no tools have been installed in clinic for delivered and planned dose differences evaluation. This difference could be large for head and neck patients who suffer the most anatomy changes compared with other treatment sites due to long treatment courses and difficulty in eating. At the same time, variable RBE dose is an increasing concern for proton therapy. The constant RBE 1.1 is widely applied in clinics, however, the real RBE is larger than 1.1 especially at the end of beam range. How they are different and what the influence on plan evaluation are an interesting topic to investigate.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript analyzes differences between planned and delivered doses as well as the effects of variable RBE (versus constant RBE=1.1) for a cohort of base-of-tongue cancer patients treated with IMPT. It motivates the work by noting that anatomy changes during long treatment courses can produce large dose discrepancies in head-and-neck cases and that variable RBE, which exceeds 1.1 at the distal beam edge, may alter plan evaluation.
Significance. If the delivered-dose and variable-RBE comparisons prove robust, the study could highlight the need for adaptive planning or site-specific RBE models in proton therapy for head-and-neck patients. The absence of comparative data across treatment sites, however, prevents the cohort from being positioned as representative of the largest possible effects.
major comments (1)
- [Background] Background: The claim that head-and-neck patients 'suffer the most anatomy changes compared with other treatment sites' is unsupported; no quantitative metrics (weight loss, CTV volume change, setup error) or citations comparing base-of-tongue cases to prostate, lung, or other sites are provided. This directly weakens the motivation for selecting this cohort as the site of largest effect.
Simulated Author's Rebuttal
We thank the referee for their review and constructive comment on our manuscript. We respond to the major comment below.
read point-by-point responses
-
Referee: The claim that head-and-neck patients 'suffer the most anatomy changes compared with other treatment sites' is unsupported; no quantitative metrics (weight loss, CTV volume change, setup error) or citations comparing base-of-tongue cases to prostate, lung, or other sites are provided. This directly weakens the motivation for selecting this cohort as the site of largest effect.
Authors: We agree that the statement is unsupported by quantitative metrics or comparative citations. The intent was to note known challenges in head-and-neck cases (long courses, eating difficulties), but the comparative phrasing ('most' relative to other sites) lacks evidence and should not have been included. We will revise the Background section to remove this claim, focusing instead on the clinical relevance of anatomy changes for base-of-tongue IMPT patients without asserting superiority of effect size over other sites. This change will be incorporated in the revised manuscript. revision: yes
Circularity Check
No circularity: empirical cohort analysis with no derivations or self-referential fits
full rationale
The paper is a retrospective clinical dosimetry study comparing planned vs. delivered doses (with constant vs. variable RBE) in a base-of-tongue IMPT cohort. No equations, parameter fits, predictions, or derivation chains are described in the provided text or abstract. The background statement that head/neck patients 'suffer the most anatomy changes' is an unsupported claim (no comparative metrics or citations), but this is an evidentiary gap rather than circularity. No self-citations, ansatzes, or renamings reduce any result to its own inputs by construction. The analysis is self-contained against external patient data and does not invoke uniqueness theorems or fitted inputs called predictions.
Axiom & Free-Parameter Ledger
Reference graph
Works this paper leans on
-
[1]
Monte Carlo simulations in radiotherapy dosimetry
Andreo P. Monte Carlo simulations in radiotherapy dosimetry. Radiat Oncol. 2018;13(1):121. doi:10.1186/s13014-018-1065-3
-
[2]
Quantification of Proton Dose Calculation Accuracy in the Lung
Grassberger C, Daartz J, Dowdell S, Ruggieri T, Sharp G, Paganetti H. Quantification of Proton Dose Calculation Accuracy in the Lung. Int J Radiat Oncol Biol Phys. 2014;89(2):424. doi:10.1016/j.ijrobp.2014.02.023
-
[3]
Pencil beam algorithms are unsuitable for proton dose calculations in lung
Taylor PA, Kry S, Followill D. Pencil beam algorithms are unsuitable for proton dose calculations in lung. Int J Radiat Oncol Biol Phys. 2017;99(3):750-756. doi:10.1016/j.ijrobp.2017.06.003
-
[4]
Paganetti H. Mechanisms and Review of Clinical Evidence of Variations in Relative Biological Effectiveness in Proton Therapy. Int J Radiat Oncol. 2022;112(1):222-236. doi:10.1016/j.ijrobp.2021.08.015
-
[5]
Giovannini G, Böhlen T, Cabal G, et al. Variable RBE in proton therapy: comparison of different model predictions and their influence on clinical-like scenarios. Radiat Oncol. 2016;11(1):68. doi:10.1186/s13014-016-0642-6
-
[6]
Ödén J, Toma-Dasu I, Witt Nyström P, Traneus E, Dasu A. Spatial correlation of linear energy transfer and relative biological effectiveness with suspected treatment-related toxicities following proton therapy for intracranial tumors. Med Phys. 2020;47(2):342-351. doi:10.1002/mp.13911
-
[7]
Paganetti H, Blakely E, Carabe-Fernandez A, et al. Report of the AAPM TG-256 on the relative biological effectiveness of proton beams in radiation therapy. Med Phys. 2019;46(3):e53-e78. doi:10.1002/mp.13390
-
[8]
The linear-quadratic formula and progress in fractionated radiotherapy
Fowler JF. The linear-quadratic formula and progress in fractionated radiotherapy. Br J Radiol. 1989;62(740):679-694. doi:10.1259/0007-1285-62-740-679 16
-
[9]
Range uncertainty in proton therapy due to variable biological effectiveness
Carabe A, Moteabbed M, Depauw N, Schuemann J, Paganetti H. Range uncertainty in proton therapy due to variable biological effectiveness. Phys Med Biol. 2012;57(5):1159-1172. doi:10.1088/0031-9155/57/5/1159
-
[10]
Wedenberg M, Lind BK, Hårdemark B. A model for the relative biological effectiveness of protons: the tissue specific parameter α/β of photons is a predictor for the sensitivity to LET changes. Acta Oncol Stockh Swed. 2013;52(3):580-588. doi:10.3109/0284186X.2012.705892
-
[11]
McNamara AL, Schuemann J, Paganetti H. A phenomenological relative biological effectiveness (RBE) model for proton therapy based on all published in vitro cell survival data. Phys Med Biol. 2015;60(21):8399-8416. doi:10.1088/0031-9155/60/21/8399
-
[12]
Hawkins RB. A microdosimetric-kinetic model of cell death from exposure to ionizing radiation of any LET, with experimental and clinical applications. Int J Radiat Biol. 1996;69(6):739-755. doi:10.1080/095530096145481
-
[13]
Elsässer T, Weyrather WK, Friedrich T, et al. Quantification of the relative biological effectiveness for ion beam radiotherapy: direct experimental comparison of proton and carbon ion beams and a novel approach for treatment planning. Int J Radiat Oncol Biol Phys. 2010;78(4):1177-1183. doi:10.1016/j.ijrobp.2010.05.014
-
[14]
Carlson DJ, Stewart RD, Semenenko VA, Sandison GA. Combined Use of Monte Carlo DNA Damage Simulations and Deterministic Repair Models to Examine Putative Mechanisms of Cell Killing. Radiat Res. 2008;169(4):447-459. doi:10.1667/RR1046.1
-
[15]
A technique for the quantitative evaluation of dose distributions
Low DA, Harms WB, Mutic S, Purdy JA. A technique for the quantitative evaluation of dose distributions. Med Phys. 1998;25(5):656-661. doi:10.1118/1.598248
-
[16]
Miften M, Olch A, Mihailidis D, et al. Tolerance limits and methodologies for IMRT measurement- based verification QA: Recommendations of AAPM Task Group No. 218. Med Phys. 2018;45(4):e53-e83. doi:10.1002/mp.12810
-
[17]
Drzymala RE, Mohan R, Brewster L, et al. Dose-volume histograms. Int J Radiat Oncol. 1991;21(1):71-78. doi:10.1016/0360-3016(91)90168-4
-
[18]
National Protocol for Model-Based Selection for Proton Therapy in Head and Neck Cancer
Langendijk JA, Hoebers FJP, de Jong MA, et al. National Protocol for Model-Based Selection for Proton Therapy in Head and Neck Cancer. Int J Part Ther. 2021;8(1):354-365. doi:10.14338/IJPT- 20-00089.1
-
[19]
Qi XS, Yang Q, Lee SP, Li XA, Wang D. An Estimation of Radiobiological Parameters for Head- and-Neck Cancer Cells and the Clinical Implications. Cancers. 2012;4(2):566-580. doi:10.3390/cancers4020566
-
[20]
Calculation of cranial nerve complication probability for acoustic neuroma radiosurgery
Meeks SL, Buatti JM, Foote KD, Friedman WA, Bova FJ. Calculation of cranial nerve complication probability for acoustic neuroma radiosurgery. Int J Radiat Oncol Biol Phys. 2000;47(3):597-602. doi:10.1016/s0360-3016(00)00493-4
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.