Free-breathing Pulmonary Relaxometry at 0.55T
Pith reviewed 2026-07-03 01:43 UTC · model grok-4.3
The pith
Free-breathing T1 and T2 mapping of the lung is feasible at 0.55T with an automated pipeline.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
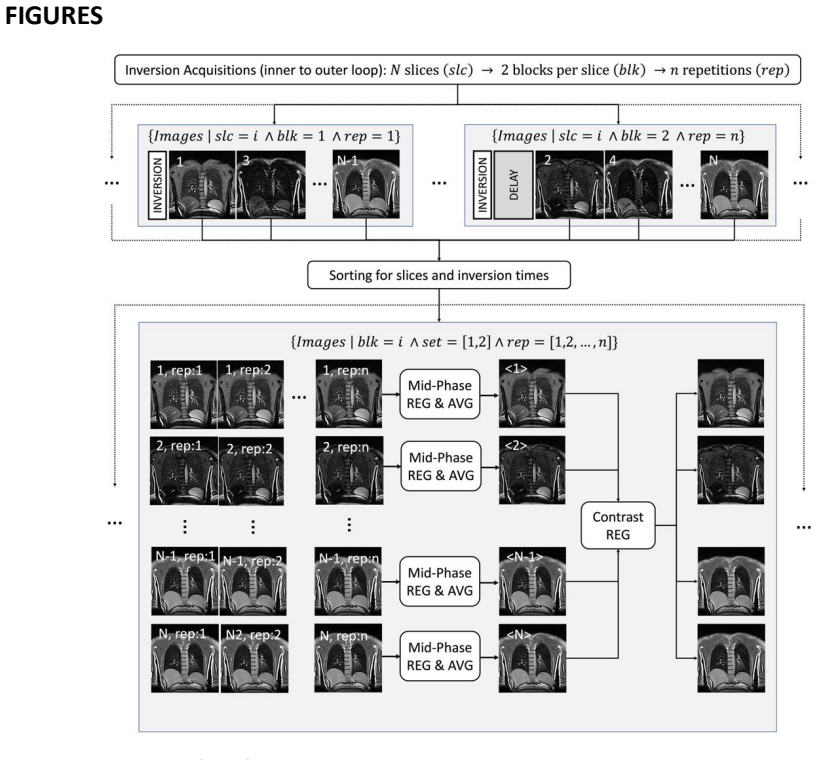
An integrated free-breathing workflow for automated 2D pulmonary relaxometry at 0.55T was developed using an adapted IR-uf-bSSFP sequence. The fully automated pipeline performs multi-contrast registration for motion correction and deep learning based lung segmentation to enable voxel-wise nonlinear fitting of T1 and T2 maps. Phantom results agreed with references, healthy lung parenchyma yielded T1 of 930 plus or minus 40 ms and T2 of 90 plus or minus 8 ms, and the single patient case distinguished a solid mass with higher T1 from surrounding parenchyma.
What carries the argument
The multi-contrast registration for motion correction together with deep learning based lung segmentation, which together permit voxel-wise nonlinear fitting of relaxation times from the transient phase data.
If this is right
- Quantitative T1 and T2 maps of the lung can be generated without breath-holds or external gating.
- Patient compliance improves because the protocol requires no instructed breath-holding.
- The method distinguishes solid lung lesions from healthy parenchyma on the basis of relaxation times.
- Quantitative lung MRI becomes potentially usable in routine clinical settings where breath-holds are impractical.
Where Pith is reading between the lines
- The same automated pipeline could be tested on other low-field scanners to assess hardware dependence.
- Extension to three-dimensional coverage would require only changes to the acquisition geometry while retaining the registration and segmentation steps.
- Application to patients with a wider range of lung pathologies would test whether the reported healthy-tissue values generalize.
Load-bearing premise
The multi-contrast registration for motion correction and deep learning based lung segmentation provide sufficient accuracy to allow reliable voxel-wise nonlinear fitting of relaxation times without significant bias from residual motion or segmentation errors.
What would settle it
Repeated free-breathing and breath-hold scans on the same subjects showing T1 or T2 values that differ by more than the reported standard deviations in regions of high respiratory motion, or maps exhibiting systematic artifacts traceable to segmentation errors.
Figures
read the original abstract
Purpose: To evaluate the feasibility of an integrated, free-breathing workflow for automated 2D pulmonary relaxometry (T1, T2) at 0.55T. Methods: A 2D inversion recovery ultra-fast balanced steady-state free precession (IR-uf-bSSFP) sequence was adapted to achieve high-temporal sampling of the transient phase at 0.55T. The technique was validated in a phantom and tested in eight healthy volunteers as well as one patient. A fully automated pipeline was developed, featuring multi-contrast registration for motion correction and deep learning based lung segmentation to enable voxel-wise nonlinear fitting for T1 and T2 map generation. Results: Phantom results were in close agreement with reference scans. In-vivo, the proposed free-breathing framework effectively mitigated respiratory motion, yielding quantitative maps in close agreement with breath-hold references. Healthy lung parenchyma relaxation times were T1 = (930+-40)ms and T2 = (90+-8)ms. In a patient case, the method successfully distinguished a solid lung mass from healthy parenchyma, with the lesion showing elevated T1 (960ms vs 810ms in the surrounding parenchyma). Conclusions: Simultaneous free-breathing T1 and T2 mapping of the lung is feasible at 0.55T using a fully automated pipeline. By eliminating breath-holds and external gating, this approach improves patient compliance and potentially facilitates the use of quantitative lung MRI in routine clinical practice.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript evaluates the feasibility of simultaneous free-breathing T1 and T2 mapping of the lungs at 0.55T using an adapted 2D IR-uf-bSSFP sequence. A fully automated pipeline incorporating multi-contrast registration for motion correction and deep learning lung segmentation enables voxel-wise nonlinear fitting. Phantom results agree with references; in-vivo data from eight healthy volunteers and one patient yield lung parenchyma values of T1 = (930±40) ms and T2 = (90±8) ms, with effective motion mitigation and close agreement to breath-hold references, plus successful lesion differentiation in the patient case.
Significance. If the registration and segmentation steps prove sufficiently accurate, the work establishes a practical route to quantitative pulmonary relaxometry without breath-holds or external gating at low field strength. This could improve patient compliance and enable broader clinical use of lung MRI relaxometry.
major comments (2)
- [Abstract, Results] Abstract and Results: The central feasibility claim rests on the assertion that multi-contrast registration and DL segmentation 'effectively mitigated' respiratory motion and produced maps 'in close agreement' with breath-hold references, yet no quantitative metrics are reported for registration accuracy (e.g., target registration error or landmark displacement) or segmentation performance (e.g., Dice coefficient or surface distance). At 0.55T, even sub-voxel residual misalignment at air-tissue interfaces can bias apparent T1/T2 values; without these numbers or a sensitivity analysis of the nonlinear fit to residual errors, the absence of significant bias remains unverified.
- [Methods, Results] Methods and Results: The description of the automated pipeline states that voxel-wise nonlinear fitting was performed after registration and segmentation, but no error propagation, statistical analysis details, or assessment of potential confounds such as B1 inhomogeneity or residual motion effects on the fit are provided. This limits evaluation of the reported standard deviations (T1 ±40 ms, T2 ±8 ms) and the patient-case distinction (960 ms vs 810 ms).
minor comments (1)
- [Abstract] The abstract reports healthy lung values as T1 = (930+-40)ms and T2 = (90+-8)ms; consistent use of the ± symbol and explicit reporting of the number of voxels or subjects contributing to these statistics would improve clarity.
Simulated Author's Rebuttal
We thank the referee for their constructive comments, which highlight important aspects of validation for our feasibility study. We address each major comment below.
read point-by-point responses
-
Referee: [Abstract, Results] Abstract and Results: The central feasibility claim rests on the assertion that multi-contrast registration and DL segmentation 'effectively mitigated' respiratory motion and produced maps 'in close agreement' with breath-hold references, yet no quantitative metrics are reported for registration accuracy (e.g., target registration error or landmark displacement) or segmentation performance (e.g., Dice coefficient or surface distance). At 0.55T, even sub-voxel residual misalignment at air-tissue interfaces can bias apparent T1/T2 values; without these numbers or a sensitivity analysis of the nonlinear fit to residual errors, the absence of significant bias remains unverified.
Authors: We agree that quantitative metrics for registration accuracy and segmentation performance would strengthen the manuscript. The original submission relied on visual assessment of motion-corrected images and quantitative agreement of the resulting T1/T2 values with breath-hold references and literature values. We will revise the Results and Methods sections to include Dice coefficients for the DL lung segmentation (computed on a subset of the volunteer data) and mean target registration errors from manually identified landmarks before and after multi-contrast registration. A brief sensitivity analysis will also be added to show the impact of sub-voxel residual motion on the nonlinear fit. revision: yes
-
Referee: [Methods, Results] Methods and Results: The description of the automated pipeline states that voxel-wise nonlinear fitting was performed after registration and segmentation, but no error propagation, statistical analysis details, or assessment of potential confounds such as B1 inhomogeneity or residual motion effects on the fit are provided. This limits evaluation of the reported standard deviations (T1 ±40 ms, T2 ±8 ms) and the patient-case distinction (960 ms vs 810 ms).
Authors: The reported standard deviations reflect the inter-voxel variability within the segmented lung parenchyma across the eight volunteers. We acknowledge that the original Methods section provided limited detail on the nonlinear fitting procedure and potential confounds. In revision we will expand the Methods to describe the Levenberg-Marquardt implementation, the weighting of the transient bSSFP signal points, and the absence of explicit error propagation. We will also add a short discussion noting that B1 inhomogeneity is reduced at 0.55 T relative to 1.5 T and that residual motion effects were assessed indirectly via the close agreement with breath-hold maps; the patient-case distinction is presented as a qualitative demonstration rather than a statistical claim. revision: yes
Circularity Check
No circularity: experimental feasibility study with direct measurements
full rationale
The paper describes an empirical MRI workflow for free-breathing T1/T2 mapping at 0.55T, validated via phantom and in-vivo experiments with direct comparison to breath-hold references. No derivation chain, first-principles predictions, or fitted parameters presented as independent outputs exist; all results are measured quantities from the described sequence, registration, segmentation, and nonlinear fitting steps. The central feasibility claim rests on experimental agreement rather than any self-referential reduction.
Axiom & Free-Parameter Ledger
axioms (1)
- domain assumption The IR-uf-bSSFP signal evolution follows the expected transient phase model for T1 and T2 estimation at 0.55T.
Reference graph
Works this paper leans on
-
[1]
This can be achieved by generating spatially resolved maps of physical parameters, such as the longitudinal T1 and transverse T2 relaxation times
INTRODUCTION Standard clinical magnetic resonance imaging (MRI) traditionally relies on qualitative morphological assessment; however, it also offers the potential for quantitative tissue characterization [1–5]. This can be achieved by generating spatially resolved maps of physical parameters, such as the longitudinal T1 and transverse T2 relaxation times...
-
[2]
The integrated body coil was used for RF transmission and a combination of a 6- channel chest array coil and a 6 -channel spine coil was used for signal reception
METHODS 2.1 MR Pulse Sequence and Imaging Parameters All experiments were performed on a whole-body 0.55T MR-scanner (MAGNETOM Free.Max, Siemens Healthineers, Forchheim, Germany), equipped with low-performance gradients (26 mT/m amplitude, 45 T/m/s slew rate). The integrated body coil was used for RF transmission and a combination of a 6- channel chest ar...
2000
-
[3]
RESULTS The quantitative accuracy of the proposed method was verified in a phantom (Figure 2). The generated maps exhibited high spatial homogeneity, and the measured relaxation times T1 = (742 ± 4) ms; T2 = (213 ± 14) ms demonstrated high concordance with the ground truth values of T1 = (736 ± 1) ms and T2 = (210 ± 10) ms as determined by a standard spin...
-
[4]
DISCUSSION In this study, we introduced and validated a fully automated method for simultaneous T1 and T2 mapping of the lung at 0.55T. The primary components of this approach consist of a free-breathing acquisition strategy , eliminating the need for external triggering or gating hardware , and a corresponding automated post-processing pipeline. Together...
-
[5]
By eliminating the need for breath-holding and external gating hardware, this technique improves patient compliance and accessibility
CONCLUSION In conclusion, we have shown that simultaneous mapping of lung parenchymal T1 and T2 can be implemented at 0.55T using a free -breathing IR -uf-bSSFP acquisition. By eliminating the need for breath-holding and external gating hardware, this technique improves patient compliance and accessibility. Future work will focus on evaluating the diagnos...
-
[6]
ACKNOWLEDGEMENTS This work was supported by the Swiss National Science Foundation, Grant/Award Number: SNF 320030_219186
-
[7]
Practical medical applications of quantitative MR relaxometry
Margaret Cheng HL, Stikov N, Ghugre NR, Wright GA. Practical medical applications of quantitative MR relaxometry. J Magn Reson Imaging. 2012;36(4):805-824. doi:10.1002/jmri.23718
-
[8]
Clinical quantitative MRI and the need for metrology
Cashmore MT, McCann AJ, Wastling SJ, McGrath C, Thornton J, Hall MG. Clinical quantitative MRI and the need for metrology. Br J Radiol. 2021;94(1120):20201215. doi:10.1259/bjr.20201215
-
[9]
Recommendations towards standards for quantitative MRI (qMRI) and outstanding needs
Keenan KE, Biller JR, Delfino JG, et al. Recommendations towards standards for quantitative MRI (qMRI) and outstanding needs. J Magn Reson Imaging JMRI. 2019;49(7):e26-e39. doi:10.1002/jmri.26598
-
[10]
Fotaki A, Velasco C, Prieto C, Botnar RM. Quantitative MRI in cardiometabolic disease: From conventional cardiac and liver tissue mapping techniques to multi-parametric approaches. Front Cardiovasc Med. 2023;9. doi:10.3389/fcvm.2022.991383
-
[11]
T1 and T2 measurements across multiple 0.55T MRI systems using open-source vendor-neutral sequences
Keenan KE, Tasdelen B, Javed A, et al. T1 and T2 measurements across multiple 0.55T MRI systems using open-source vendor-neutral sequences. Magn Reson Med. 2025;93(1):289-300. doi:10.1002/mrm.30281
-
[12]
Imaging biomarker roadmap for cancer studies
O’Connor JPB, Aboagye EO, Adams JE, et al. Imaging biomarker roadmap for cancer studies. Nat Rev Clin Oncol. 2017;14(3):169-186. doi:10.1038/nrclinonc.2016.162
-
[13]
MR imaging of the chest: a practical approach at 1.5T
Puderbach M, Hintze C, Ley S, Eichinger M, Kauczor HU, Biederer J. MR imaging of the chest: a practical approach at 1.5T. Eur J Radiol. 2007;64(3):345-355. doi:10.1016/j.ejrad.2007.08.009
-
[14]
New applications of magnetic resonance imaging for thoracic oncology
Ohno Y. New applications of magnetic resonance imaging for thoracic oncology. Semin Respir Crit Care Med. 2014;35(1):27-40. doi:10.1055/s-0033-1363449
-
[15]
D’Angelo T, Vogl TJ, Wichmann JL. From low-dose to no-dose: thin-section magnetic resonance imaging for evaluation of pulmonary nodules. J Thorac Dis. 2018;10(Suppl 9). doi:10.21037/jtd.2018.04.65
-
[16]
MRI of the lung (3/3)-current applications and future perspectives
Biederer J, Mirsadraee S, Beer M, et al. MRI of the lung (3/3)-current applications and future perspectives. Insights Imaging. 2012;3(4):373-386. doi:10.1007/s13244-011-0142-z
-
[17]
[Imaging of the lung using low-field magnetic resonance imaging]
Hinsen M, Heiss R, Nagel AM, et al. [Imaging of the lung using low-field magnetic resonance imaging]. Radiol. 2022;62(5):418-428. doi:10.1007/s00117-022-00996-7
-
[18]
Biederer J, Beer M, Hirsch W, et al. MRI of the lung (2/3). Why … when … how? Insights Imaging. 2012;3(4):355-371. doi:10.1007/s13244-011-0146-8
-
[19]
Lung parenchyma transverse relaxation rates at 0.55 T
Li B, Lee NG, Cui SX, Nayak KS. Lung parenchyma transverse relaxation rates at 0.55 T. Magn Reson Med. 2023;89(4):1522-1530. doi:10.1002/mrm.29541
-
[20]
Quantitative regional oxygen transfer imaging of the human lung
Arnold JFT, Kotas M, Fidler F, Pracht ED, Flentje M, Jakob PM. Quantitative regional oxygen transfer imaging of the human lung. J Magn Reson Imaging JMRI. 2007;26(3):637-645. doi:10.1002/jmri.21033
-
[21]
MR imaging of pulmonary parenchyma with a half-Fourier single-shot turbo spin-echo (HASTE) sequence
Hatabu H, Gaa J, Tadamura E, et al. MR imaging of pulmonary parenchyma with a half-Fourier single-shot turbo spin-echo (HASTE) sequence. Eur J Radiol. 1999;29(2):152-159. doi:10.1016/s0720-048x(98)00167-3
-
[22]
Triphan SMF, Breuer FA, Gensler D, Kauczor HU, Jakob PM. Oxygen enhanced lung MRI by simultaneous measurement of T1 and T2 * during free breathing using ultrashort TE. J Magn Reson Imaging JMRI. 2015;41(6):1708-1714. doi:10.1002/jmri.24692
-
[23]
Free-Breathing Lung MR Fingerprinting at 0.55T with Retrospective Respiratory Motion Binning
Liu Z, Seiberlich N, Hamilton J. Free-Breathing Lung MR Fingerprinting at 0.55T with Retrospective Respiratory Motion Binning. In: Proc. Intl. Soc. Mag. Reson. Med. 33. ; 2025:1867
2025
-
[24]
Stadler A, Jakob PM, Griswold M, Stiebellehner L, Barth M, Bankier AA. T1 mapping of the entire lung parenchyma: Influence of respiratory phase and correlation to lung function test results in patients with diffuse lung disease. Magn Reson Med. 2008;59(1):96-101. doi:10.1002/mrm.21446
-
[25]
Jobst BJ, Triphan SMF, Sedlaczek O, et al. Functional lung MRI in chronic obstructive pulmonary disease: comparison of T1 mapping, oxygen-enhanced T1 mapping and dynamic contrast enhanced perfusion. PloS One. 2015;10(3):e0121520. doi:10.1371/journal.pone.0121520
-
[26]
T2 mapping of CT remodelling patterns in interstitial lung disease
Buzan MTA, Eichinger M, Kreuter M, et al. T2 mapping of CT remodelling patterns in interstitial lung disease. Eur Radiol. 2015;25(11):3167-3174. doi:10.1007/s00330-015-3751-y
-
[27]
Principles and applications of balanced SSFP techniques
Scheffler K, Lehnhardt S. Principles and applications of balanced SSFP techniques. Eur Radiol. 2003;13(11):2409-2418. doi:10.1007/s00330-003-1957-x
-
[28]
Inversion recovery TrueFISP: quantification of T(1), T(2), and spin density
Schmitt P, Griswold MA, Jakob PM, et al. Inversion recovery TrueFISP: quantification of T(1), T(2), and spin density. Magn Reson Med. 2004;51(4):661-667. doi:10.1002/mrm.20058
-
[29]
Pulmonary relaxometry with inversion recovery ultra- fast steady-state free precession at 1.5T
Bauman G, Santini F, Pusterla O, Bieri O. Pulmonary relaxometry with inversion recovery ultra- fast steady-state free precession at 1.5T. Magn Reson Med. 2017;77(1):74-82. doi:10.1002/mrm.26490
-
[30]
Bieri O. Ultra-fast steady state free precession and its application to in vivo (1)H morphological and functional lung imaging at 1.5 tesla. Magn Reson Med. 2013;70(3):657-663. doi:10.1002/mrm.24858
-
[31]
Rapid Free-Breathing and Automated 2D Shimming of the Lung at 3T
Panos P, Bauman G, Bieri O. Rapid Free-Breathing and Automated 2D Shimming of the Lung at 3T. Magn Reson Med. 2026;95(5):2737-2745. doi:10.1002/mrm.70238
-
[32]
Scale-space and edge detection using anisotropic diffusion
Perona P, Malik J. Scale-space and edge detection using anisotropic diffusion. IEEE Trans Pattern Anal Mach Intell. 1990;12(7):629-639. doi:10.1109/34.56205
-
[33]
Diffeomorphic demons: Efficient non- parametric image registration
Vercauteren T, Pennec X, Perchant A, Ayache N. Diffeomorphic demons: Efficient non- parametric image registration. NeuroImage. 2009;45(1, Supplement 1):S61-S72. doi:10.1016/j.neuroimage.2008.10.040
-
[34]
Avants BB, Epstein CL, Grossman M, Gee JC. Symmetric diffeomorphic image registration with cross-correlation: evaluating automated labeling of elderly and neurodegenerative brain. Med Image Anal. 2008;12(1):26-41. doi:10.1016/j.media.2007.06.004
-
[35]
Highly accurate inverse consistent registration: a robust approach
Reuter M, Rosas HD, Fischl B. Highly accurate inverse consistent registration: a robust approach. NeuroImage. 2010;53(4):1181-1196. doi:10.1016/j.neuroimage.2010.07.020
-
[36]
A reproducible evaluation of ANTs similarity metric performance in brain image registration
Avants BB, Tustison NJ, Song G, Cook PA, Klein A, Gee JC. A reproducible evaluation of ANTs similarity metric performance in brain image registration. NeuroImage. 2011;54(3):2033-2044. doi:10.1016/j.neuroimage.2010.09.025
-
[37]
Pusterla O, Heule R, Santini F, et al. MRI lung lobe segmentation in pediatric cystic fibrosis patients using a recurrent neural network trained with publicly accessible CT datasets. Magn Reson Med. 2022;88(1):391-405. doi:10.1002/mrm.29184
-
[38]
Perfusion-Informed Deep Learning for Automated Pulmonary Vessel Segmentation
Panos P, Oliver B, Bauman G. Perfusion-Informed Deep Learning for Automated Pulmonary Vessel Segmentation. In: Proceedings of the Cape Town - 2026 ISMRM-ISMRT Annual Meeting and Exhibition. Cape Town, South Africa
2026
-
[39]
Feasibility of MR fingerprinting using a high-performance 0.55 T MRI system
Campbell-Washburn AE, Jiang Y, Körzdörfer G, Nittka M, Griswold MA. Feasibility of MR fingerprinting using a high-performance 0.55 T MRI system. Magn Reson Imaging. 2021;81:88-
2021
-
[40]
doi:10.1016/j.mri.2021.06.002
-
[41]
Kato Y, Ichikawa K, Okudaira K, et al. Comprehensive Evaluation of B1+-corrected FISP-based Magnetic Resonance Fingerprinting: Accuracy, Repeatability and Reproducibility of T1 and T2 Relaxation Times for ISMRM/NIST System Phantom and Volunteers. Magn Reson Med Sci. 2019;19(3):168-175. doi:10.2463/mrms.mp.2019-0016
-
[42]
Parker GJM, Barker GJ, Tofts PS. Accurate multislice gradient echo T1 measurement in the presence of non-ideal RF pulse shape and RF field nonuniformity. Magn Reson Med. 2001;45(5):838-845. doi:10.1002/mrm.1112
-
[43]
Mutual-information-based registration of medical images: a survey
Pluim JPW, Maintz JBA, Viergever MA. Mutual-information-based registration of medical images: a survey. IEEE Trans Med Imaging. 2003;22(8):986-1004. doi:10.1109/TMI.2003.815867
-
[44]
Elements of Information Theory 2nd ed - T
Ravindra K. Elements of Information Theory 2nd ed - T. Cover, J. Thomas (Wiley, 2006) WW. https://www.academia.edu/25024538/Elements_of_Information_Theory_2nd_ed_T_Cover_J_T homas_Wiley_2006_WW. Accessed May 27, 2026
-
[45]
Campbell-Washburn AE, Ramasawmy R, Restivo MC, et al. Opportunities in Interventional and Diagnostic Imaging by Using High-Performance Low-Field-Strength MRI. Radiology. 2019;293(2):384-393. doi:10.1148/radiol.2019190452
-
[46]
Yan Q, Yi Y, Shen J, et al. Preliminary study of 3 T-MRI native T1-mapping radiomics in differential diagnosis of non-calcified solid pulmonary nodules/masses. Cancer Cell Int. 2021;21(1):539. doi:10.1186/s12935-021-02195-1
-
[47]
Li G, Huang R, Zhu M, et al. Native T1-mapping and diffusion-weighted imaging (DWI) can be used to identify lung cancer pathological types and their correlation with Ki-67 expression. J Thorac Dis. 2022;14(2):443-454. doi:10.21037/jtd-22-77 [41 ] Scheffler K, Heid O, Hennig J. Magnetization preparation during the steady state: fat-saturated 3D TrueFISP. M...
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.