Recognition: unknown
Grounding Clinical AI Competency in Human Cognition Through the Clinical World Model and Skill-Mix Framework
Pith reviewed 2026-05-10 17:03 UTC · model grok-4.3
The pith
Clinical AI competency forms an irreducible space of billions of distinct coordinates.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
The Clinical AI Skill-Mix operationalizes competency through eight dimensions. Five define the clinical competency space (condition, phase, care setting, provider role, and task) and three specify how AI engages human reasoning (assigned authority, agent facing, and anchoring layer). The combinatorial product of these dimensions yields a space of billions of distinct competency coordinates. A central structural implication is that validation within one coordinate provides minimal evidence for performance in another, rendering the competency space irreducible. The framework supplies a common grammar through which clinical AI can be specified, evaluated, and bounded across stakeholders.
What carries the argument
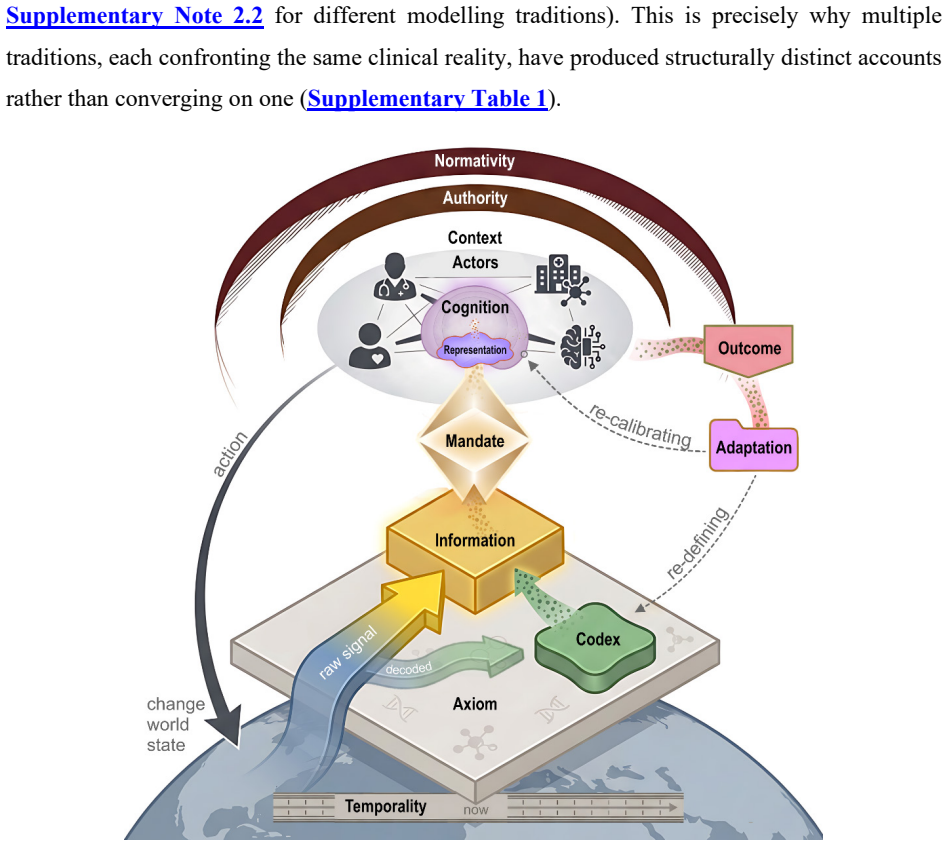
The Clinical World Model as a tripartite interaction among Patient, Provider, and Ecosystem, paired with the eight-dimensional Skill-Mix that generates the combinatorial competency space.
Load-bearing premise
The eight dimensions comprehensively and independently capture all relevant aspects of clinical competency and human cognition without significant overlap or missing factors.
What would settle it
A controlled study finding that validated performance in one set of dimensions, such as a specific condition and care setting, strongly predicts performance in a different condition, phase, or provider role would falsify the claim that the space is irreducible.
Figures
read the original abstract
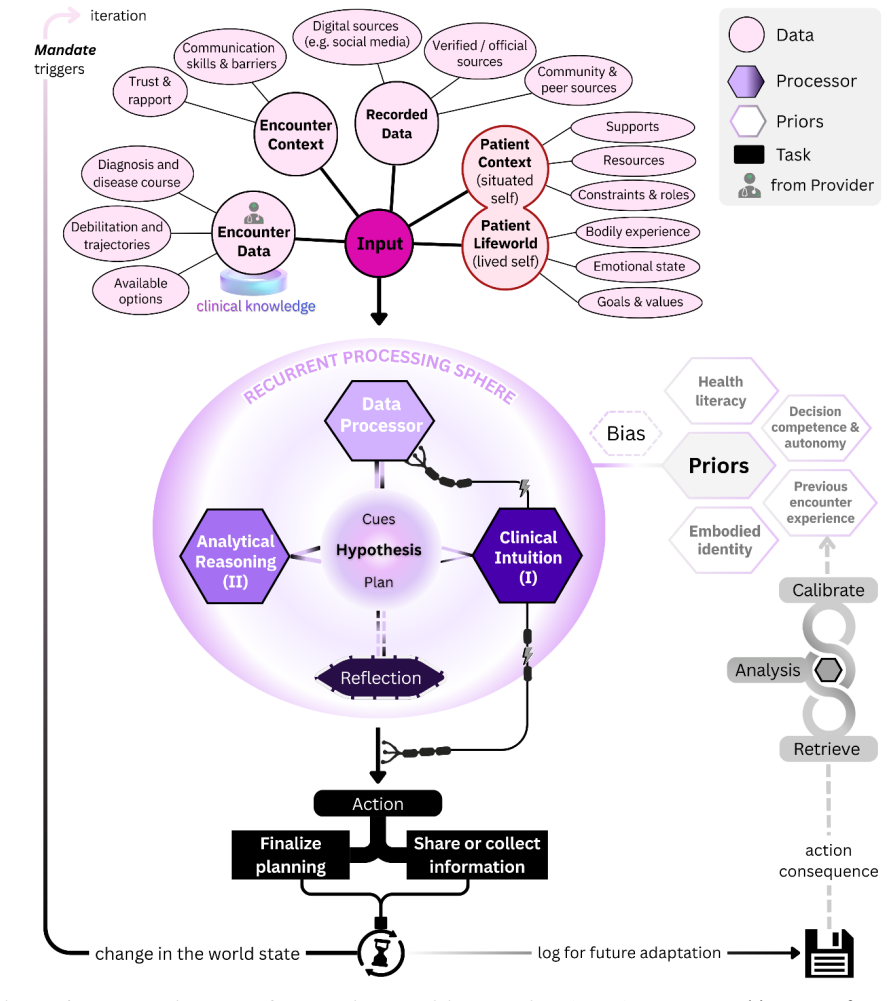
The competency of any intelligent agent is bounded by its formal account of the world in which it operates. Clinical AI lacks such an account. Existing frameworks address evaluation, regulation, or system design in isolation, without a shared model of the clinical world to connect them. We introduce the Clinical World Model, a framework that formalizes care as a tripartite interaction among Patient, Provider, and Ecosystem. To formalize how any agent, whether human or artificial, transforms information into clinical action, we develop parallel decision-making architectures for providers, patients, and AI agents, grounded in validated principles of clinical cognition. The Clinical AI Skill-Mix operationalizes competency through eight dimensions. Five define the clinical competency space (condition, phase, care setting, provider role, and task) and three specify how AI engages human reasoning (assigned authority, agent facing, and anchoring layer). The combinatorial product of these dimensions yields a space of billions of distinct competency coordinates. A central structural implication is that validation within one coordinate provides minimal evidence for performance in another, rendering the competency space irreducible. The framework supplies a common grammar through which clinical AI can be specified, evaluated, and bounded across stakeholders. By making this structure explicit, the Clinical World Model reframes the field's central question from whether AI works to in which competency coordinates reliability has been demonstrated, and for whom.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper introduces the Clinical World Model, which formalizes clinical care as a tripartite interaction among Patient, Provider, and Ecosystem, and develops parallel decision-making architectures for human and AI agents grounded in principles of clinical cognition. It then presents the Clinical AI Skill-Mix framework defined by eight dimensions (condition, phase, care setting, provider role, task, assigned authority, agent facing, and anchoring layer). The combinatorial product of these dimensions is claimed to generate billions of distinct competency coordinates, with the central implication that validation in one coordinate provides minimal evidence for performance in another, rendering the space irreducible and supplying a common grammar for specifying, evaluating, and bounding clinical AI.
Significance. If the eight dimensions can be shown to be mutually independent and collectively exhaustive of factors influencing clinical performance, the framework could provide a valuable conceptual tool for moving beyond binary assessments of AI efficacy toward coordinate-specific reliability claims. This reframing has potential utility for regulatory, design, and stakeholder alignment purposes in clinical AI. As presented, however, the work remains a high-level proposal without empirical grounding or formal justification, limiting its immediate significance to stimulating structured discussion rather than enabling new analyses or predictions.
major comments (2)
- [Abstract and Skill-Mix Framework] Abstract and Skill-Mix Framework description: The claim that the competency space is irreducible because 'validation within one coordinate provides minimal evidence for performance in another' rests on the assertion that the eight dimensions are independent and exhaustive. No orthogonality argument, explicit mapping to 'validated principles of clinical cognition,' or analysis of potential covariances (e.g., between provider role and assigned authority) or omitted factors (e.g., temporal drift or patient-specific priors) is supplied to support this.
- [Clinical World Model] Clinical World Model section: The tripartite model and parallel decision-making architectures are introduced conceptually but without formal definitions, derivations, or concrete mappings showing how they connect to the eight Skill-Mix dimensions or establish the claimed grounding in human cognition.
minor comments (2)
- The manuscript would benefit from one or two worked examples showing how an existing clinical AI system (e.g., a diagnostic model) maps onto specific coordinates and what validation would look like under the framework.
- Additional citations to existing literature on clinical competency frameworks, human factors in medicine, and AI evaluation taxonomies would help position the contribution relative to prior work.
Simulated Author's Rebuttal
We thank the referee for their constructive review, which identifies key areas where the conceptual nature of the Clinical World Model and Skill-Mix framework requires additional clarification. We address each major comment below, providing the strongest honest defense of the manuscript's approach while noting where revisions strengthen the presentation without misrepresenting its scope as a high-level framework.
read point-by-point responses
-
Referee: [Abstract and Skill-Mix Framework] Abstract and Skill-Mix Framework description: The claim that the competency space is irreducible because 'validation within one coordinate provides minimal evidence for performance in another' rests on the assertion that the eight dimensions are independent and exhaustive. No orthogonality argument, explicit mapping to 'validated principles of clinical cognition,' or analysis of potential covariances (e.g., between provider role and assigned authority) or omitted factors (e.g., temporal drift or patient-specific priors) is supplied to support this.
Authors: The manuscript grounds the eight dimensions in established principles of clinical cognition (e.g., dual-process reasoning, situated decision-making, and role-based expertise from cognitive psychology and health services research) rather than claiming mathematical orthogonality. The first five dimensions delineate the clinical context in which competency is exercised, while the final three specify the mode of AI engagement with human reasoning; this separation is intended to highlight that each coordinate combination defines a distinct validation target, even if real-world covariances exist. We agree that covariances (such as between provider role and assigned authority) and omitted factors (such as temporal drift) merit discussion and have added a dedicated paragraph in the Skill-Mix section acknowledging these interdependencies and noting that the framework treats dimensions as analytically separable for the purpose of bounding claims, not as strictly independent variables. Explicit mappings to cognitive principles have been expanded with citations. A full orthogonality proof or covariance analysis lies outside the scope of this conceptual paper and would require dedicated empirical work; the central claim remains that cross-coordinate generalization cannot be assumed a priori. revision: partial
-
Referee: [Clinical World Model] Clinical World Model section: The tripartite model and parallel decision-making architectures are introduced conceptually but without formal definitions, derivations, or concrete mappings showing how they connect to the eight Skill-Mix dimensions or establish the claimed grounding in human cognition.
Authors: The Clinical World Model is presented as a conceptual scaffold to unify existing isolated approaches, drawing on validated cognitive principles such as System 1/System 2 processing and ecological rationality rather than introducing new formalisms. The tripartite structure (Patient–Provider–Ecosystem) formalizes the interaction space in which any agent's decision architecture operates, and the parallel architectures for human and AI agents are defined at the level of information transformation steps (perception, reasoning, action) to enable direct comparison. We have revised the section to include a new table and accompanying text that explicitly maps each World Model component to the Skill-Mix dimensions—for instance, linking the 'anchoring layer' to the provider's cognitive architecture and the 'agent facing' dimension to the tripartite interaction roles. Concrete examples of how these architectures manifest in specific competency coordinates (e.g., diagnostic reasoning in acute care) have been added. Full mathematical derivations are reserved for subsequent technical papers; the current work prioritizes establishing a shared grammar over axiomatic formalization. revision: yes
Circularity Check
No significant circularity; framework is self-contained definitional model
full rationale
The paper introduces the Clinical World Model as a tripartite formalization of care and the Skill-Mix Framework via explicit definition of eight dimensions whose combinatorial product is stated to produce billions of coordinates. The 'central structural implication' of irreducibility is presented directly as a logical consequence of that definition rather than as a prediction derived from independent data, equations, or prior results. No self-citations, fitted parameters renamed as predictions, ansatzes smuggled via citation, or uniqueness theorems are invoked in a load-bearing way. The derivation chain consists of definitional steps grounded in stated principles of clinical cognition, with no reduction of outputs to inputs by construction.
Axiom & Free-Parameter Ledger
axioms (2)
- domain assumption Clinical care can be formalized as a tripartite interaction among Patient, Provider, and Ecosystem.
- ad hoc to paper The eight dimensions fully define the clinical competency space and are independent enough to create billions of distinct coordinates.
invented entities (2)
-
Clinical World Model
no independent evidence
-
Clinical AI Skill-Mix
no independent evidence
Reference graph
Works this paper leans on
-
[1]
SEIPS 2.0: A Human Factors Framework for Healthcare Professionals and Patients (Holden, 2013)20 Aim and Targeted Problem: SEIPS 2.0 extends the original SEIPS model to address the evolving nature of healthcare as a complex sociotechnical system where both professionals and patients actively participate. The framework incorporates three novel concepts (con...
work page 2013
-
[2]
SEIPS 3.0: Human -Centered Design of the Patient Journey for Patient Safety (Carayon, 2020)16 Aim and Targeted Problem: SEIPS 3.0 addresses the challenge that healthcare is increasingly distributed over space and time, with patients interacting with multiple care settings, organizations, and providers throughout their illness trajectory. The model expands...
work page 2020
-
[3]
CORE-MD Clinical Risk Score for Regulatory Evaluation of AI -Based Medical Device Software (Rademakers, 2025)21 Aim and Targeted Problem: The CORE-MD (Coordinating Research and Evidence for Medical Devices) consortium addresses the challenge of determining appropriate clinical evidence requirements for AI -based medical device software (MDSW) before regul...
work page 2025
-
[4]
Expert Consensus on Retrospective Evaluation of LLM Applications in Clinical Scenarios (Chang et al., 2025)22 Aim and Targeted Problem: This expert consensus addresses the lack of standardized evaluation criteria and consistent methodologies for assessing Large Language Model (LLM) applications in healthcare prior to deployment. The framework focuses spec...
work page 2025
-
[5]
ArgMed -Agents: Explainable Clinical Decision Reasoning with LLM Discussion via Argumentation Schemes (Hong et al., 2024)23 Aim and Targeted Problem: This paper addresses two fundamental barriers to deploying LLMs in clinical decision support: (1) LLMs demonstrate inadequate performance in complex reasoning and planning tasks despite strong NLP capabiliti...
work page 2024
-
[6]
MedHELM (Bedi et al., 2025)18 Aim and Targeted Problem: MedHELM addresses the fundamental disconnect between LLM performance on medical licensing examinations (achieving ~99% accuracy) and readiness for real- world clinical deployment. The framework targets three critical limitations in existing evaluation approaches: questions that do not match real-worl...
work page 2025
-
[7]
GlobMed (Yang et al., 2025)24 Aim and Targeted Problem: GlobMed addresses the critical global health inequity created by LLMs trained predominantly on high-resource languages (92% of GPT-3's pretraining is English), which systematically excludes low -resource language communities —those who would benefit most from AI-assisted healthcare. The framework ide...
work page 2025
-
[8]
ClinicalLab (Yan et al., 2024)25 Aim and Targeted Problem: ClinicalLab addresses critical limitations in existing clinical diagnostic evaluation benchmarks for medical LLMs and agents. The framework targets four specific gaps: (1) existing be nchmarks face data leakage or contamination risks from publicly available training data; (2) existing benchmarks n...
work page 2024
-
[9]
DynamiCare (Shang et al., 2025)26 Aim and Targeted Problem: DynamiCare addresses the fundamental mismatch between static, single-turn AI evaluation paradigms and the inherently dynamic, interactive, and iterative nature of real clinical diagnosis. Current frameworks assume complete case information is provided upfront, whereas actual clinical encounters i...
work page 2025
-
[10]
KG4Diagnosis (Zuo, 2024)27 Aim and Targeted Problem: KG4Diagnosis addresses the challenge that integrating Large Language Models in healthcare diagnosis demands systematic frameworks capable of handling complex medical scenarios while maintaining specialized expertise. The targeted problem is that single-agent LLM approaches lack domain -specific precisio...
work page 2024
-
[11]
MEDIC Framework (Kanithi, 2024)28 Aim and Targeted Problem: MEDIC addresses the widening gap between theoretical capability and verified clinical utility of LLMs in healthcare. While models achieve superhuman performance on standardized medical licensing examinations (e.g., USMLE), these static benchmarks have become saturated and increasingly disconnecte...
work page 2024
-
[12]
Cognitive science and clinical reasoning research formalized how providers and patients transform perception into action under uncertainty (Decision-Making Model)52,52,112, while theory- of-mind and shared mental model research examined how agents construct internal representations of one another's states, intentions, and anticipated responses (Mental Mod...
-
[13]
Thinking encompasses the active manipulation of mental representations, including attention, memory retrieval, and pattern 82 recognition, which allows individuals to construct coherent interpretations of complex situations128. Reasoning extends this through systematic inference processes, including deductive reasoning (applying general principles to spec...
-
[14]
These processes do not operate in isolation but form cascading chains where perceptual inputs activate relevant knowledge structures, trigger context -appropriate reasoning strategies, and culminate in decisions that select among competing action options128. In expert domains such as clinical medicine, these cognitive processes become highly specialized a...
-
[15]
Various factors may contribute to shifts between the two systems . Prior experience with a similar condition, as well as time constraints, limited energy, emotional pressure, or high metacognitive confidence, can bias decision- making toward System I . System I is influenced by affective cues and embodied sensations, is prone to bias, and reaches conclusi...
-
[16]
In contrast, System II evaluates the initial judgment and its underlying components before arriving at a final decision. This reasoning process operates as an iterative loop that ultimately culminates in a final action, whether reaching a diagnostic conclusion or gathering additional information to resolve remaining uncertainty 52. Decision-making in clin...
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.