Oxygenation and spatial heterogeneity shape radiotherapy protocol ranking through phenotypic adaptation
Pith reviewed 2026-06-30 11:08 UTC · model grok-4.3
The pith
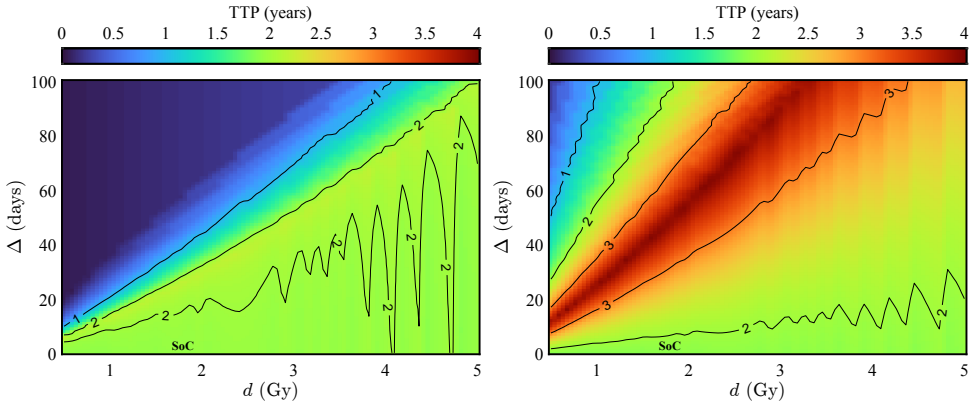
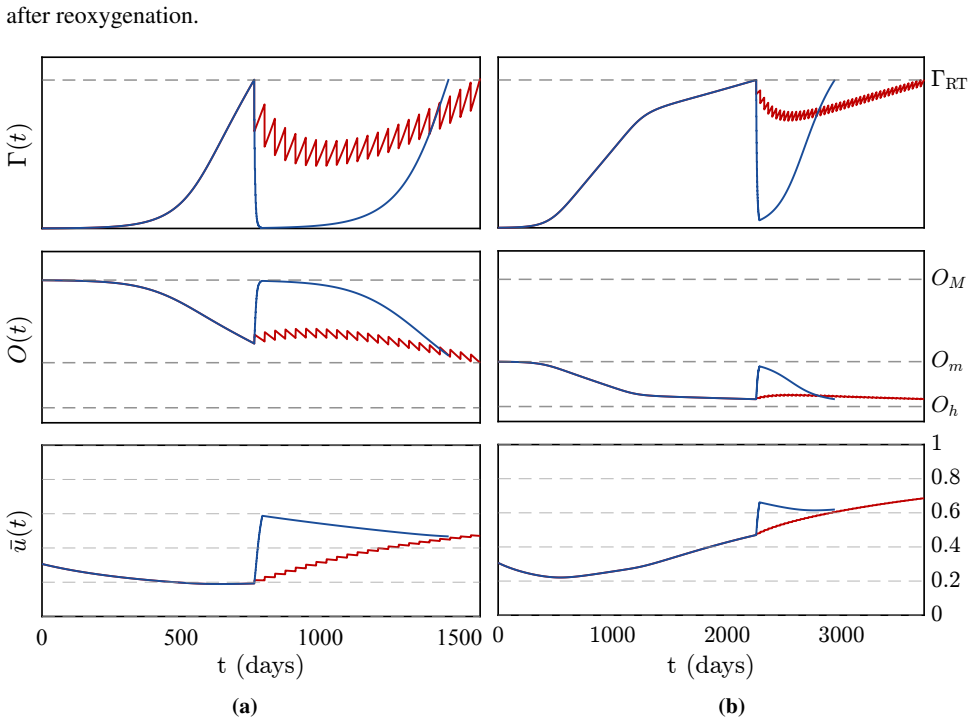
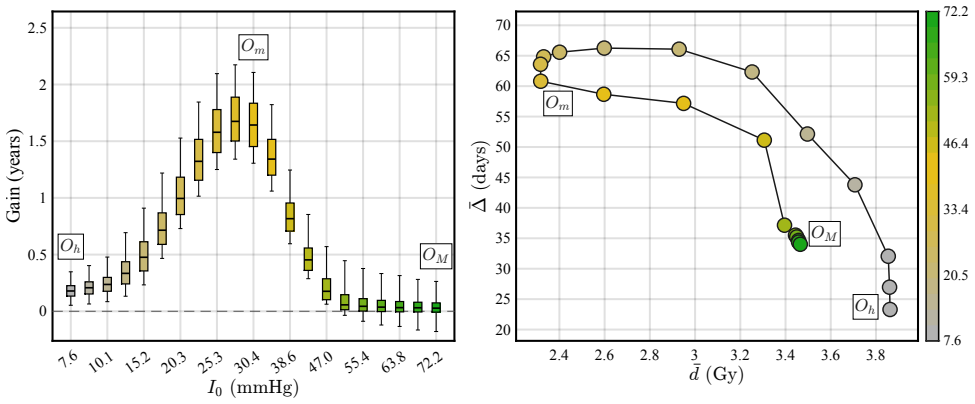
Under moderate hypoxia, protracted radiotherapy schedules with longer intervals between fractions can double time-to-progression by altering the balance between reoxygenation and selection for resistant phenotypes.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
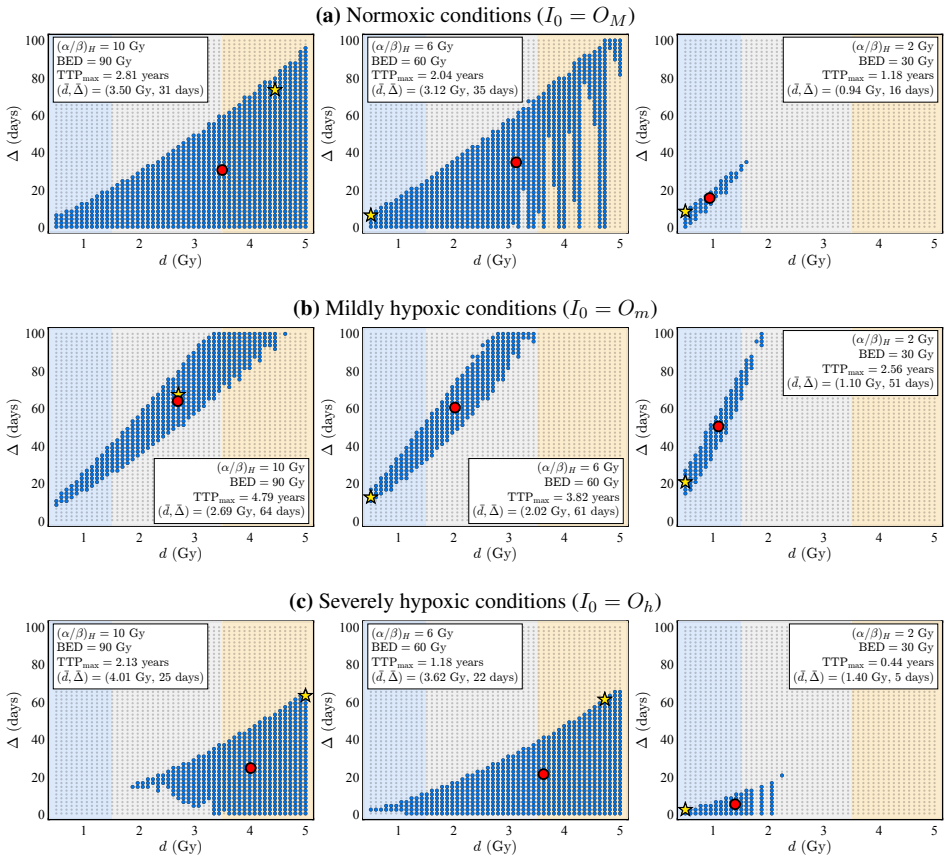
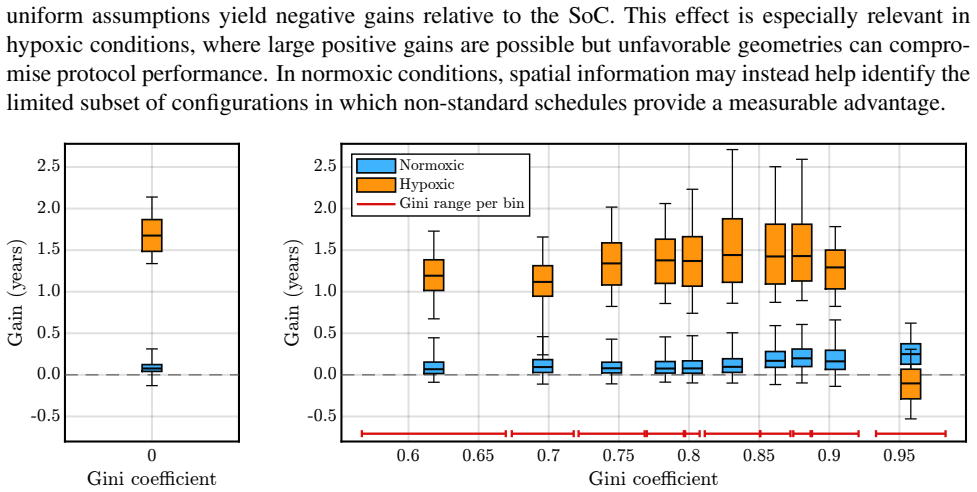
A mathematical model that integrates spatial oxygen dynamics with continuous phenotypic adaptation shows that under moderate hypoxia protracted fractionation schedules substantially increase time-to-progression by shifting the balance between reoxygenation and selection for resistant phenotypes; when oxygen delivery is spatially heterogeneous, the geometric organization of sources produces large variability in outcomes and can change the relative ranking of protocols even at identical total oxygen supply.
What carries the argument
Integrated model of spatial oxygen dynamics and continuous phenotypic adaptation to hypoxia and radiation, used to rank fractionation schedules under a shared normal-tissue toxicity constraint.
If this is right
- Under moderate hypoxia protracted schedules with longer intervals can increase time-to-progression up to twofold relative to standard protocols.
- Different spatial arrangements of oxygen sources produce large variability in time-to-progression even when total oxygen supply is fixed.
- Geometric organization of oxygen delivery can reverse the ranking of otherwise identical fractionation schedules.
- Radiotherapy effectiveness emerges from the interaction of schedule, microenvironmental structure, and evolutionary dynamics rather than from schedule properties alone.
Where Pith is reading between the lines
- Mapping oxygen source geometry inside individual tumors could be used to select the fractionation schedule expected to perform best for that geometry.
- The same model framework could be extended to ask whether adding agents that block phenotypic adaptation would widen or narrow the advantage of protracted schedules.
- Clinical imaging that resolves local oxygen heterogeneity might identify patients for whom standard schedules are likely to underperform.
Load-bearing premise
Phenotypic adaptation occurs continuously and predictably shifts the reoxygenation-versus-resistance balance as a direct function of inter-fraction interval length.
What would settle it
An experiment that measures time-to-progression in controlled moderate-hypoxia tumor spheroids or xenografts under standard versus protracted schedules, with and without pharmacological blockade of phenotypic adaptation, would test whether the predicted doubling occurs.
Figures
read the original abstract
Tumor response to radiotherapy is strongly influenced by oxygen availability and phenotypic heterogeneity, yet their combined impact on the relative performance of fractionation schedules remains unclear. Here, we develop a mathematical model that integrates spatial oxygen dynamics with continuous phenotypic adaptation to hypoxia and radiation, and use it to systematically compare radiotherapy protocols under a common normal-tissue toxicity constraint. Under spatially uniform oxygenation, we find that alternative fractionation schedules provide little improvement over standard-of-care protocols in normoxic conditions. Under moderate hypoxia, however, a distinct class of protracted schedules with longer inter-fraction intervals substantially increases time-to-progression, in some cases by up to twofold. This regime-dependent benefit is consistent with a shift in the balance between reoxygenation and selection for resistant phenotypes. When oxygen delivery is spatially heterogeneous, treatment outcomes depend strongly on the geometric organization of oxygen sources. Even with identical total oxygen supply, different spatial configurations lead to large variability in time-to-progression and can alter the relative ranking of radiotherapy protocols. These results show that radiotherapy effectiveness is not an intrinsic property of a treatment schedule alone, but emerges from its interaction with tumor microenvironmental structure and evolutionary dynamics. Incorporating both spatial heterogeneity and phenotypic adaptation may therefore be important for the consistent evaluation and design of fractionation strategies in heterogeneous tumors.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript develops a mathematical model that integrates spatial oxygen dynamics with continuous phenotypic adaptation to hypoxia and radiation. It systematically compares radiotherapy fractionation protocols under a fixed normal-tissue toxicity constraint. Key claims include that under spatially uniform moderate hypoxia, protracted schedules with longer inter-fraction intervals increase time-to-progression by up to twofold relative to standard protocols, attributed to a shift favoring reoxygenation over resistant-phenotype selection; under normoxia the benefit is minimal. With spatially heterogeneous oxygen delivery, outcomes and protocol rankings vary strongly with the geometric arrangement of oxygen sources even at fixed total oxygen supply.
Significance. If the model predictions hold, the work demonstrates that fractionation schedule performance is not an intrinsic property of the schedule but emerges from its interaction with microenvironmental structure and evolutionary dynamics. This provides a transparent framework (two free parameters governing adaptation rates and oxygen consumption/delivery) for exploring regime-dependent protocol ranking. The internal consistency between equations and reported numerical outcomes, together with the absence of hidden parameter tuning, strengthens the result as a falsifiable prediction for future experimental tests in hypoxic tumor models.
minor comments (3)
- [Abstract] Abstract: the statement that protracted schedules 'substantially increase time-to-progression, in some cases by up to twofold' would be strengthened by a parenthetical reference to the specific parameter regime or figure panel in which this factor is obtained.
- [Methods] The implementation of the normal-tissue toxicity constraint is described only at a high level; an explicit equation or short paragraph in the methods section showing how total dose or biologically effective dose is normalized across schedules would aid reproducibility.
- [Results] Figure captions for spatial heterogeneity results should state the precise metric used to quantify 'geometric organization' (e.g., number or spacing of oxygen sources) so that readers can map the reported ranking changes to concrete configurations.
Simulated Author's Rebuttal
We thank the referee for the positive assessment of the manuscript, the accurate summary of its contributions, and the recommendation for minor revision. No specific major comments were listed in the report.
Circularity Check
No significant circularity; model predictions are simulation outputs under stated assumptions
full rationale
The paper constructs a mathematical model integrating spatial oxygen dynamics and continuous phenotypic adaptation, then numerically compares fractionation schedules under a toxicity constraint. No load-bearing step reduces by construction to a fitted parameter renamed as prediction, a self-citation chain, or a definitional loop. Time-to-progression rankings emerge from forward simulation of the coupled PDE/ODE system rather than from parameter tuning that encodes the target result. The derivation chain remains self-contained against external benchmarks; the reader's 5.0 suspicion is not supported by any quoted reduction in the provided text.
Axiom & Free-Parameter Ledger
free parameters (2)
- phenotypic adaptation rates to hypoxia and radiation
- oxygen consumption and delivery parameters
axioms (2)
- domain assumption Phenotypic adaptation to hypoxia and radiation occurs continuously and can be modeled as a deterministic process that alters radiation sensitivity over time
- domain assumption Normal-tissue toxicity is equivalent across all fractionation schedules when total dose is constrained
Reference graph
Works this paper leans on
-
[1]
The hallmarks of cancer
Hanahan D and Weinberg RA. The hallmarks of cancer. Cell 2000; 100:57–70
2000
-
[2]
Siegel RL, Miller KD, Wagle NS, and Jemal A. Cancer statistics, 2023. CA: A Cancer Journal for Clinicians 2023; 73:17–48.DOI:10.3322/caac.21763
-
[3]
Tumor hypoxia and radiotherapy: a major driver of resistance even for novel radiotherapy modalities
Beckers C, Pruschy M, and Vetrugno I. Tumor hypoxia and radiotherapy: a major driver of resistance even for novel radiotherapy modalities. Seminars in Cancer Biology 2024; 98:19– 30.DOI:10.1016/j.semcancer.2023.11.006
-
[4]
Oxygen levels do not determine radi- ation survival of breast cancer stem cells
Lagadec C, Dekmezian C, Bauch ´e L, and Pajonk F. Oxygen levels do not determine radi- ation survival of breast cancer stem cells. PLOS ONE 2012; 7:e34545.DOI:10 . 1371 / journal.pone.0034545
2012
-
[5]
Biologically-based mathematical modeling of tumor vasculature and angiogenesis via time-resolved imaging data
Hormuth DA, Phillips CM, Wu C, Lima EABF, Lorenzo G, Jha PK, Jarrett AM, Oden JT, and Yankeelov TE. Biologically-based mathematical modeling of tumor vasculature and angiogenesis via time-resolved imaging data. Cancers 2021; 13:3008.DOI:10 . 3390 / cancers13123008
2021
-
[6]
Mathematical modeling in radiotherapy for cancer: a comprehensive narrative review
Zheng D, Preuss K, Milano MT, He X, Gou L, Shi Y, Marples B, Wan R, Yu H, Du H, and Zhang C. Mathematical modeling in radiotherapy for cancer: a comprehensive narrative review. Radiation Oncology 2025; 20:49.DOI:10.1186/s13014-025-02626-7 18
-
[8]
Wenzl T and Wilkens JJ. Theoretical analysis of the dose dependence of the oxygen enhance- ment ratio and its relevance for clinical applications. Radiation Oncology 2011; 6:171.DOI: 10.1186/1748-717X-6-171
-
[9]
Alfonso JCL and Berk L. Modeling the effect of intratumoral heterogeneity of radiosensitivity on tumor response over the course of fractionated radiation therapy. Radiation Oncology 2019; 14:88.DOI:10.1186/s13014-019-1288-y
-
[10]
Celora GL, Byrne HM, and Kevrekidis PG. Spatio-temporal modelling of phenotypic het- erogeneity in tumour tissues and its impact on radiotherapy treatment. Journal of Theoretical Biology 2023; 556:111248.DOI:10.1016/j.jtbi.2022.111248
-
[11]
Chiari G, Fiandaca G, and Delitala ME. Hypoxia-related radiotherapy resistance in tumors: treatment efficacy investigation in an eco-evolutionary perspective. Frontiers in Applied Math- ematics and Statistics 2023; 9:1193191.DOI:10.3389/fams.2023.1193191
-
[12]
Prokopiou S, Moros EG, Poleszczuk J, Caudell JJ, Torres-Roca JF, and Enderling H. A pro- liferation saturation index to predict radiation response and personalize radiotherapy fraction- ation. Radiation Oncology 2015; 10:159.DOI:10.1186/s13014-015-0465-x
-
[13]
Non-standard radiotherapy fractionations delay the time to malignant transfor- mation of low-grade gliomas
Henares-Molina A, Benzekry S, Lara PC, Garc ´ıa-Rojo M, P´erez-Garc´ıa VM, and Mart´ınez- Gonz´alez A. Non-standard radiotherapy fractionations delay the time to malignant transfor- mation of low-grade gliomas. PLOS ONE 2017; 12:1–19.DOI:10 . 1371 / journal . pone.0178552
2017
-
[14]
Br ¨uningk SC, Peacock J, Whelan CJ, Brady-Nicholls R, Yu HHM, Sahebjam S, and Enderling H. Intermittent radiotherapy as alternative treatment for recurrent high grade glioma: a mod- eling study based on longitudinal tumor measurements. Scientific Reports 2021; 11:20219. DOI:10.1038/s41598-021-99507-2
-
[15]
Phenotype structuring in collective cell migration: a tu- torial of mathematical models and methods
Lorenzi T, Painter KJ, and Villa C. Phenotype structuring in collective cell migration: a tu- torial of mathematical models and methods. Journal of Mathematical Biology 2025; 90:61. DOI:10.1007/s00285-025-02223-y
-
[16]
MOREOVER: multiomics MR-guided radiotherapy optimization in locally advanced rectal cancer
Boldrini L, Chiloiro G, Di Franco S, Romano A, Smiljanic L, Tran EH, Bono F, Davies CD, Lopetuso L, De Bonis M, Minucci A, Giac `o L, Cusumano D, Placidi L, Giannarelli D, Sala E, and Gambacorta MA. MOREOVER: multiomics MR-guided radiotherapy optimization in locally advanced rectal cancer. Radiation Oncology 2024; 19:94.DOI:10.1186/s13014- 024-02492-9
-
[17]
Molecular imaging-based dose painting: a novel paradigm for radiation therapy prescription
Bentzen SM and Gr ´egoire V. Molecular imaging-based dose painting: a novel paradigm for radiation therapy prescription. Seminars in Radiation Oncology 2011; 21:101–10.DOI:10. 1016/j.semradonc.2010.10.001
2011
-
[18]
The linear quadratic model: usage, interpretation and challenges
McMahon SJ. The linear quadratic model: usage, interpretation and challenges. Physics in Medicine and Biology 2018; 64:01TR01.DOI:10.1088/1361-6560/aaf26a
-
[19]
Rockne R, Rockhill JK, Mrugala M, Spence AM, Kalet I, Hendrickson K, Lai A, Cloughesy T, Alvord E. C. J, and Swanson KR. Predicting the efficacy of radiotherapy in individual glioblastoma patients in vivo: a mathematical modeling approach. Physics in Medicine and Biology 2010; 55:3271–85.DOI:10.1088/0031-9155/55/12/001
-
[20]
The sensitivity of microorganisms to irradiation under con- trolled gas conditions
Howard-Flanders P and Alper T. The sensitivity of microorganisms to irradiation under con- trolled gas conditions. Radiation Research 1957; 7:518–40.DOI:10.2307/3570400 19
-
[21]
Brenner DJ. The linear-quadratic model is an appropriate methodology for determining iso- effective doses at large doses per fraction. Seminars in Radiation Oncology 2008; 18:234–9. DOI:10.1016/j.semradonc.2008.04.004
-
[22]
Del Monte U. Does the cell number 10(9) still really fit one gram of tumor tissue? Cell Cycle 2009; 8:505–6.DOI:10.4161/cc.8.3.7608
-
[23]
A mechanistic investigation of the oxygen enhancement ra- tio and its relevance to radiotherapy
Grimes DR and Partridge M. A mechanistic investigation of the oxygen enhancement ra- tio and its relevance to radiotherapy. Biomedical Physics & Engineering Express 2015; 1:045209.DOI:10.1088/2057-1976/1/4/045209
-
[24]
Defining normoxia, physoxia and hypoxia in tumours: implications for treat- ment response
McKeown SR. Defining normoxia, physoxia and hypoxia in tumours: implications for treat- ment response. British Journal of Radiology 2014; 87:20130676.DOI:10 . 1259 / bjr . 20130676
2014
-
[25]
Mart ´ınez-Gonz´alez A, Calvo GF, P´erez Romasanta LA, and P´erez-Garc´ıa VM. Hypoxic cell waves around necrotic cores in glioblastoma: a biomathematical model and its therapeutic im- plications. Bulletin of Mathematical Biology 2012; 74:2875–96.DOI:10.1007/s11538- 012-9786-1
-
[26]
The linear-quadratic model is inappropriate to model high dose per fraction effects in radiosurgery
Kirkpatrick JP, Meyer JJ, and Marks LB. The linear-quadratic model is inappropriate to model high dose per fraction effects in radiosurgery. Seminars in Radiation Oncology 2008; 18:240– 3.DOI:10.1016/j.semradonc.2008.04.005
-
[27]
Cui M, Gao XS, Li X, et al. Variability of alpha/beta ratios for prostate cancer with the frac- tionation schedule: caution against using the linear-quadratic model for hypofractionated ra- diotherapy. Radiation Oncology 2022; 17:54.DOI:10.1186/s13014-022-02010-9
-
[28]
Brower JV, Amini A, Chen S, Hullett CR, Kimple RJ, Wojcieszynski AP, Bassetti M, Witek ME, Yu M, Harari PM, and Baschnagel AM. Improved survival with dose-escalated radio- therapy in stage III non-small-cell lung cancer: analysis of the National Cancer Database. Annals of Oncology 2016; 27:1887–94.DOI:10.1093/annonc/mdw276
-
[29]
Excessive toxicity when treating central tumors in a phase II study of stereotactic body radiation therapy for medically inop- erable early-stage lung cancer
Timmerman R, McGarry R, Yiannoutsos C, Papiez L, Tudor K, DeLuca J, Ewing M, Ab- dulrahman R, DesRosiers C, Williams M, and Fletcher J. Excessive toxicity when treating central tumors in a phase II study of stereotactic body radiation therapy for medically inop- erable early-stage lung cancer. Journal of Clinical Oncology 2006; 24:4833–9.DOI:10 . 1200/JCO...
2006
-
[30]
Are more complicated tumour control probability models better? Mathematical Medicine and Biology 2013; 30:1–19.DOI:10
Gong J, Dos Santos MM, Finlay C, and Hillen T. Are more complicated tumour control probability models better? Mathematical Medicine and Biology 2013; 30:1–19.DOI:10. 1093/imammb/dqr023
2013
-
[31]
Gaito S, Burnet N, Aznar M, Crellin A, Indelicato DJ, Ingram S, Pan S, Price G, Hwang E, France A, Smith E, and Whitfield G. Normal tissue complication probability modelling for toxicity prediction and patient selection in proton beam therapy to the central nervous system: a literature review. Clinical Oncology (Royal College of Radiologists) 2022; 34:e22...
-
[32]
Nuijens AC, Oei AL, Franken NAP, Rasch CRN, and Stalpers LJA. Towards personalized radiotherapy in pelvic cancer: patient-related risk factors for late radiation toxicity. Current Oncology 2025; 32:47.DOI:10.3390/curroncol32010047
-
[33]
Delineation of organs at risk in radiotherapy and perspectives
Eber J, Bockel S, Antoni D, Khamphan C, No ¨el G, and Le F`evre C. Delineation of organs at risk in radiotherapy and perspectives. Cancer/Radioth´erapie 2025; 29:104758
2025
-
[34]
Is alpha/beta for prostate tumors really low? Interna- tional Journal of Radiation Oncology, Biology, Physics 2001; 50:1021–31.DOI:10.1016/ S0360-3016(01)01607-8 20
Fowler JF, Chappell R, and Ritter MA. Is alpha/beta for prostate tumors really low? Interna- tional Journal of Radiation Oncology, Biology, Physics 2001; 50:1021–31.DOI:10.1016/ S0360-3016(01)01607-8 20
2001
-
[35]
Steel GG, McMillan TJ, and Peacock JH. The 5Rs of radiobiology. International Journal of Radiation Biology 1989; 56:1045–8.DOI:10.1080/09553008914552491
-
[36]
[18 F ] FMISO- PET imaging reveals the role of hypoxia severity in checkpoint blockade response
McNeal KC, Reeves KM, Song PN, Lapi SE, Sorace AG, and Larimer BM. [18 F ] FMISO- PET imaging reveals the role of hypoxia severity in checkpoint blockade response. Nuclear Medicine and Biology 2024; 134–135:108918.DOI:10.1016/j.nucmedbio.2024. 108918
-
[37]
Cicchetti A, Laurino F, Possenti L, Rancati T, and Zunino P. In silico model of the early ef- fects of radiation therapy on the microcirculation and the surrounding tissues. Physica Medica 2020; 73:125–34.DOI:10.1016/j.ejmp.2020.04.006
-
[38]
Qiu GZ, Jin MZ, Dai JX, Sun W, Feng JH, and Jin WL. Reprogramming of the tumor in the hypoxic niche: the emerging concept and associated therapeutic strategies. Trends in Pharma- cological Sciences 2017; 38:669–86.DOI:10.1016/j.tips.2017.05.002 21 Supporting Information This section contains supplementary material intended to support the results presented...
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.