CoMNet: A MedNeXt-CorrDiff Framework for Multi-Site Brain Tumor Segmentation
Pith reviewed 2026-07-01 07:05 UTC · model grok-4.3
The pith
An ensemble of MedNeXt fold predictions refined by a corrective diffusion block produces higher Dice scores on multi-site glioma MRI datasets.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
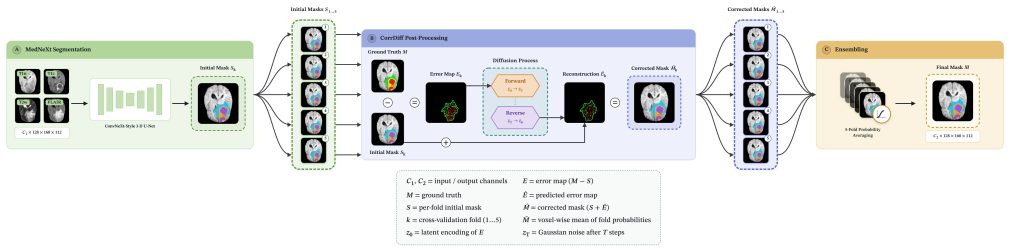
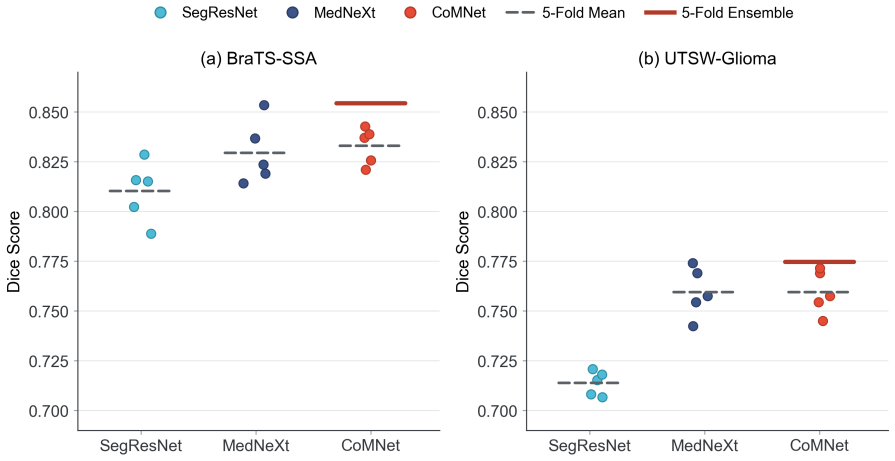
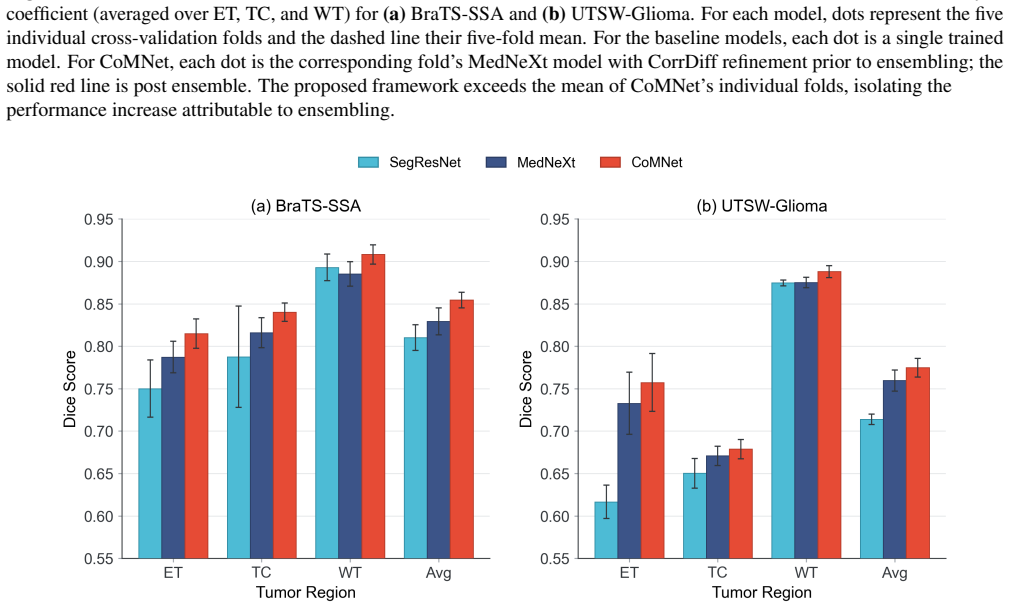
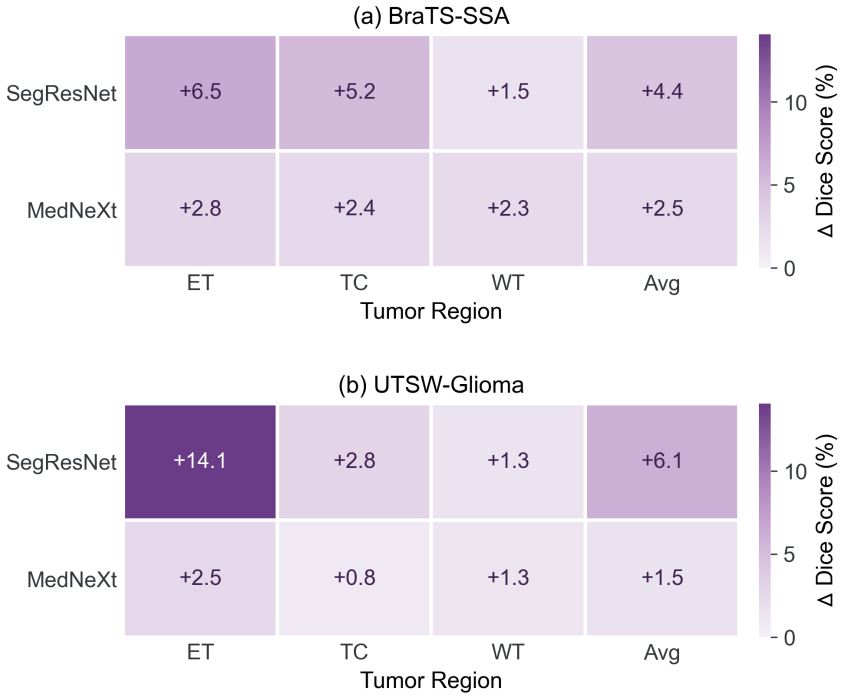
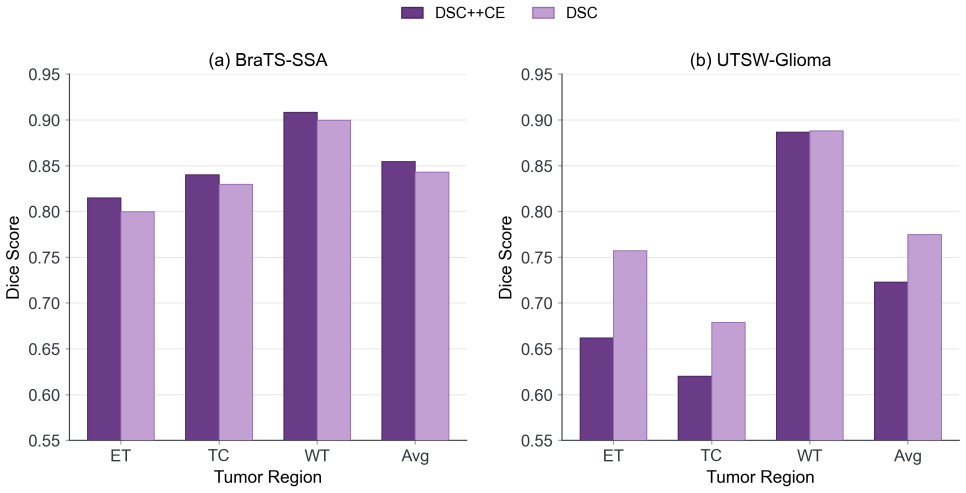
CoMNet uses MedNeXt as the primary 3D segmentation network and adds a corrective diffusion block that learns to correct residual errors in individual fold prediction maps. These corrected maps are then aggregated via probabilistic thresholding into a final mask. The resulting ensemble achieves the highest Dice score compared with two baseline models on the UTSW-Glioma and BraTS-SSA datasets while remaining less sensitive to site-dependent imaging variability.
What carries the argument
The corrective diffusion block that refines residual errors across MedNeXt fold predictions before ensembling them into a consensus mask.
If this is right
- Fold-level probability ensembling becomes a practical way to stabilize predictions across scanner differences.
- Corrective diffusion post-processing can be added to existing state-of-the-art 3D networks without changing their training.
- The method improves segmentation of small but clinically important regions such as enhancing tumor and tumor core.
- Multi-site robustness is obtained without explicit domain adaptation or site labels during inference.
Where Pith is reading between the lines
- The same corrective-diffusion-plus-ensemble pattern may transfer to other segmentation tasks that suffer from acquisition-site shifts.
- Clinical deployment could become simpler if one model plus diffusion refinement replaces multiple site-tuned models.
- Testing on longitudinal scans from the same patients would show whether the reduced variance also improves change detection over time.
Load-bearing premise
The diffusion block can learn corrections that reduce site variance without adding new artifacts or needing site-specific adjustments.
What would settle it
On a held-out multi-site glioma dataset the CoMNet Dice score falls below the plain MedNeXt baseline or the corrected masks show measurable new false-positive regions compared with the uncorrected folds.
Figures
read the original abstract
Accurate brain tumor segmentation from multiparametric magnetic resonance imaging (MRI) is critical for treatment planning, response assessment, and neuro-oncology research. However, automated segmentation remains a difficult task in computer vision because of variation in tumor appearance and MRI protocols across patient scans. Moreover, clinically important regions such as enhancing tumor and tumor core are often small relative to the full brain volume, further increasing the difficulty of achieving high voxel-level precision. These challenges are amplified in multi-site datasets, where differences in scanner hardware and acquisition parameters can introduce non-biological variation. To address this, networks must learn tumor-specific features while remaining robust to site-dependent noise. In this paper, we show that an ensemble of multi-fold predictions from a modern 3D convolutional segmentation network with corrective diffusion (CorrDiff) post-processing improves brain tumor segmentation across datasets. We propose CoMNet, an ensembled MedNeXt-CorrDiff framework for accurate multi-site brain tumor segmentation. In this framework, we use MedNeXt as the primary segmentation model for feature learning, while a corrective diffusion block learns to refine the residual errors in the individual prediction maps before probabilistic thresholding. This process reduces the variance across fold predictions by correcting fold-specific residual errors and aggregating them into a consensus mask that is less sensitive to site-dependent imaging variability. Our proposed framework achieved the highest Dice score compared to two baseline models on the UTSW-Glioma and BraTS-SSA datasets. Experimental results support the use of corrective diffusion and fold-level probability ensembling as meaningful additions to existing state-of-the-art models for accurate glioma segmentation on multi-site datasets.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript proposes CoMNet, an ensembled MedNeXt-CorrDiff framework that uses multi-fold predictions from a 3D convolutional segmentation network followed by a corrective diffusion post-processing block to refine residual errors and reduce site-dependent variance in multi-site brain tumor segmentation on MRI. It claims this yields the highest Dice scores versus two baseline models on the UTSW-Glioma and BraTS-SSA datasets.
Significance. If the performance gains are real, statistically validated, and attributable to the CorrDiff block rather than ensembling alone, the work could provide a useful, site-agnostic refinement strategy for handling scanner variability in clinical glioma segmentation. The absence of any quantitative results, ablations, or variance metrics in the manuscript prevents assessment of whether this significance is realized.
major comments (1)
- [Abstract] Abstract: The central claim that the framework 'achieved the highest Dice score compared to two baseline models' supplies no Dice values, standard deviations, p-values, ablation results (with vs. without CorrDiff), or site-stratified metrics. This leaves the weakest assumption—that the corrective diffusion block reduces site-dependent variance without new artifacts—untested by any reported evidence.
Simulated Author's Rebuttal
We thank the referee for the feedback highlighting the need for quantitative support in the abstract. We agree the current abstract is insufficiently detailed and will revise it (and related sections) to include specific metrics, ablations, and variance analysis.
read point-by-point responses
-
Referee: [Abstract] Abstract: The central claim that the framework 'achieved the highest Dice score compared to two baseline models' supplies no Dice values, standard deviations, p-values, ablation results (with vs. without CorrDiff), or site-stratified metrics. This leaves the weakest assumption—that the corrective diffusion block reduces site-dependent variance without new artifacts—untested by any reported evidence.
Authors: We agree the abstract must be revised to report concrete Dice scores (with standard deviations), p-values where computed, ablation comparisons (with vs. without CorrDiff), and site-stratified results. The revised abstract will explicitly state the numerical improvements on UTSW-Glioma and BraTS-SSA. We will also add explicit reporting of prediction variance across folds/sites and a brief analysis confirming CorrDiff does not introduce new artifacts (e.g., via visual inspection and quantitative edge-error metrics). These changes will be made in the next version; the experimental section will be expanded if needed to ensure all supporting data are present. revision: yes
Circularity Check
No circularity; empirical performance claim with no derivation chain
full rationale
The paper describes an empirical segmentation framework (MedNeXt ensemble + CorrDiff post-processing) and asserts a highest Dice score on two datasets versus baselines. No equations, parameter-fitting steps, self-definitional relations, or load-bearing self-citations appear in the supplied text. The central claim is an experimental comparison result rather than any quantity derived from or equivalent to its own inputs by construction. This is the common case of a methods paper whose validity rests on external benchmarks, not internal reduction.
Axiom & Free-Parameter Ledger
Reference graph
Works this paper leans on
-
[1]
& Balasamy, K
Suganyadevi, S., Seethalakshmi, V . & Balasamy, K. A review on deep learning in medical image analysis.Int. J. Multimed. Inf. Retr.11, 19–38 (2022)
2022
-
[2]
K., Hadjiiski, L
Chan, H.-P., Samala, R. K., Hadjiiski, L. M. & Zhou, C. Deep learning in medical image analysis.Deep. learning medical image analysis: challenges applications3–21 (2020)
2020
-
[3]
Liu, Z.et al.Deep learning based brain tumor segmentation: a survey.Complex & intelligent systems9, 1001–1026 (2023)
2023
-
[4]
G.et al.Multi-class glioma segmentation on real-world data with missing mri sequences: comparison of three deep learning algorithms.Sci
Pemberton, H. G.et al.Multi-class glioma segmentation on real-world data with missing mri sequences: comparison of three deep learning algorithms.Sci. reports13, 18911 (2023)
2023
-
[5]
& Frayne, R
Bento, M., Fantini, I., Park, J., Rittner, L. & Frayne, R. Deep learning in large and multi-site structural brain mr imaging datasets.Front. neuroinformatics15, 805669 (2022). 13/15
2022
-
[6]
In 2024 IEEE International Symposium on Biomedical Imaging (ISBI), 1–4 (IEEE, 2024)
Jiang, Z.et al.Enhancing generalizability in brain tumor segmentation: Model ensemble with adaptive post-processing. In 2024 IEEE International Symposium on Biomedical Imaging (ISBI), 1–4 (IEEE, 2024)
2024
-
[7]
Adewole, M.et al.The brats-africa dataset: expanding the brain tumor segmentation data to capture african populations. Radiol. Artif. Intell.7, e240528 (2025)
2025
-
[8]
journal computer assisted radiology surgery19, 2101–2109 (2024)
De Sutter, S.et al.Modality redundancy for mri-based glioblastoma segmentation.Int. journal computer assisted radiology surgery19, 2101–2109 (2024)
2024
-
[9]
InProceedings of the IEEE/CVF conference on computer vision and pattern recognition, 11976–11986 (2022)
Liu, Z.et al.A convnet for the 2020s. InProceedings of the IEEE/CVF conference on computer vision and pattern recognition, 11976–11986 (2022)
2022
-
[10]
InInternational conference on medical image computing and computer-assisted intervention, 405–415 (Springer, 2023)
Roy, S.et al.Mednext: transformer-driven scaling of convnets for medical image segmentation. InInternational conference on medical image computing and computer-assisted intervention, 405–415 (Springer, 2023)
2023
- [11]
-
[12]
& Zheng, Y
Li, W., Huang, W. & Zheng, Y . Corrdiff: Corrective diffusion model for accurate mri brain tumor segmentation.IEEE J. Biomed. Heal. Informatics28, 1587–1598 (2024)
2024
-
[13]
& Liu, M
Guan, H. & Liu, M. Domain adaptation for medical image analysis: a survey.IEEE Transactions on Biomed. Eng.69, 1173–1185 (2021)
2021
-
[14]
H., Kalra, S
Kushol, R., Wilman, A. H., Kalra, S. & Yang, Y .-H. Dsmri: domain shift analyzer for multi-center mri datasets.Diagnostics 13, 2947 (2023)
2023
-
[15]
& Yap, P.-T
Liu, S. & Yap, P.-T. Learning multi-site harmonization of magnetic resonance images without traveling human phantoms. Commun. engineering3, 6 (2024)
2024
-
[16]
OnLine23, 90 (2024)
Abbasi, S.et al.Deep learning for the harmonization of structural mri scans: a survey.BioMedical Eng. OnLine23, 90 (2024)
2024
- [17]
-
[18]
& Liu, M
Wu, M., Yu, M., Lin, W., Yap, P.-T. & Liu, M. Unpaired multi-site brain mri harmonization with image style-guided latent diffusion. InInternational Conference on Medical Image Computing and Computer-Assisted Intervention, 683–693 (Springer, 2025)
2025
-
[19]
NeuroImage316, 121297 (2025)
Lan, H.et al.Diffusion based multi-domain neuroimaging harmonization method with preservation of anatomical details. NeuroImage316, 121297 (2025)
2025
-
[20]
& Brox, T
Ronneberger, O., Fischer, P. & Brox, T. U-net: Convolutional networks for biomedical image segmentation. InInternational Conference on Medical image computing and computer-assisted intervention, 234–241 (Springer, 2015)
2015
-
[21]
S., Brox, T
Çiçek, Ö., Abdulkadir, A., Lienkamp, S. S., Brox, T. & Ronneberger, O. 3d u-net: learning dense volumetric segmentation from sparse annotation. InInternational conference on medical image computing and computer-assisted intervention, 424–432 (Springer, 2016)
2016
-
[22]
& Ahmadi, S.-A
Milletari, F., Navab, N. & Ahmadi, S.-A. V-net: Fully convolutional neural networks for volumetric medical image segmentation. In2016 fourth international conference on 3D vision (3DV), 565–571 (Ieee, 2016)
2016
-
[23]
3d mri brain tumor segmentation using autoencoder regularization
Myronenko, A. 3d mri brain tumor segmentation using autoencoder regularization. InInternational MICCAI brainlesion workshop, 311–320 (Springer, 2018)
2018
-
[24]
F., Kohl, S
Isensee, F., Jaeger, P. F., Kohl, S. A., Petersen, J. & Maier-Hein, K. H. nnu-net: a self-configuring method for deep learning-based biomedical image segmentation.Nat. methods18, 203–211 (2021)
2021
-
[25]
Chen, J.et al.Transunet: Transformers make strong encoders for medical image segmentation.arXiv preprint arXiv:2102.04306(2021)
work page internal anchor Pith review Pith/arXiv arXiv 2021
-
[26]
In International MICCAI brainlesion workshop, 272–284 (Springer, 2021)
Hatamizadeh, A.et al.Swin unetr: Swin transformers for semantic segmentation of brain tumors in mri images. In International MICCAI brainlesion workshop, 272–284 (Springer, 2021)
2021
-
[27]
InInternational conference on medical image computing and computer-assisted intervention, 109–119 (Springer, 2021)
Wang, W.et al.Transbts: Multimodal brain tumor segmentation using transformer. InInternational conference on medical image computing and computer-assisted intervention, 109–119 (Springer, 2021)
2021
-
[28]
InProceedings of the IEEE/CVF conference on computer vision and pattern recognition, 16133–16142 (2023)
Woo, S.et al.Convnext v2: Co-designing and scaling convnets with masked autoencoders. InProceedings of the IEEE/CVF conference on computer vision and pattern recognition, 16133–16142 (2023). 14/15
2023
-
[29]
& Abbeel, P
Ho, J., Jain, A. & Abbeel, P. Denoising diffusion probabilistic models.Adv. neural information processing systems33, 6840–6851 (2020)
2020
-
[30]
image analysis88, 102846 (2023)
Kazerouni, A.et al.Diffusion models in medical imaging: A comprehensive survey.Med. image analysis88, 102846 (2023)
2023
-
[31]
& Cattin, P
Wolleb, J., Sandkühler, R., Bieder, F., Valmaggia, P. & Cattin, P. C. Diffusion models for implicit image segmentation ensembles. InInternational conference on medical imaging with deep learning, 1336–1348 (PMLR, 2022). 32.Wu, J.et al.Medsegdiff: Medical image segmentation with diffusion probabilistic model. InMedical imaging with deep learning, 1623–1639...
2022
-
[32]
H.et al.The multimodal brain tumor image segmentation benchmark (brats).IEEE transactions on medical imaging34, 1993–2024 (2014)
Menze, B. H.et al.The multimodal brain tumor image segmentation benchmark (brats).IEEE transactions on medical imaging34, 1993–2024 (2014)
1993
-
[33]
D.et al.Advancing brain tumor analysis: Curating a high-quality mri dataset for deep learning-based molecular marker profiling
Reddy, D. D.et al.Advancing brain tumor analysis: Curating a high-quality mri dataset for deep learning-based molecular marker profiling. InProceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, 2373–2379 (2024)
2024
-
[34]
D.et al.The university of texas southwestern glioma dataset-mri, molecular markers and segmentations.Sci
Reddy, D. D.et al.The university of texas southwestern glioma dataset-mri, molecular markers and segmentations.Sci. Data(2026). 15/15
2026
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.