Promise and challenges of heart chamber segmentation from non-contrast CT scans using contrastive unpaired image translation: a feasibility study
Pith reviewed 2026-06-26 06:03 UTC · model grok-4.3
The pith
ChameleonNet enables heart chamber segmentation from non-contrast CT scans by translating contrast images without manual non-contrast labels.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
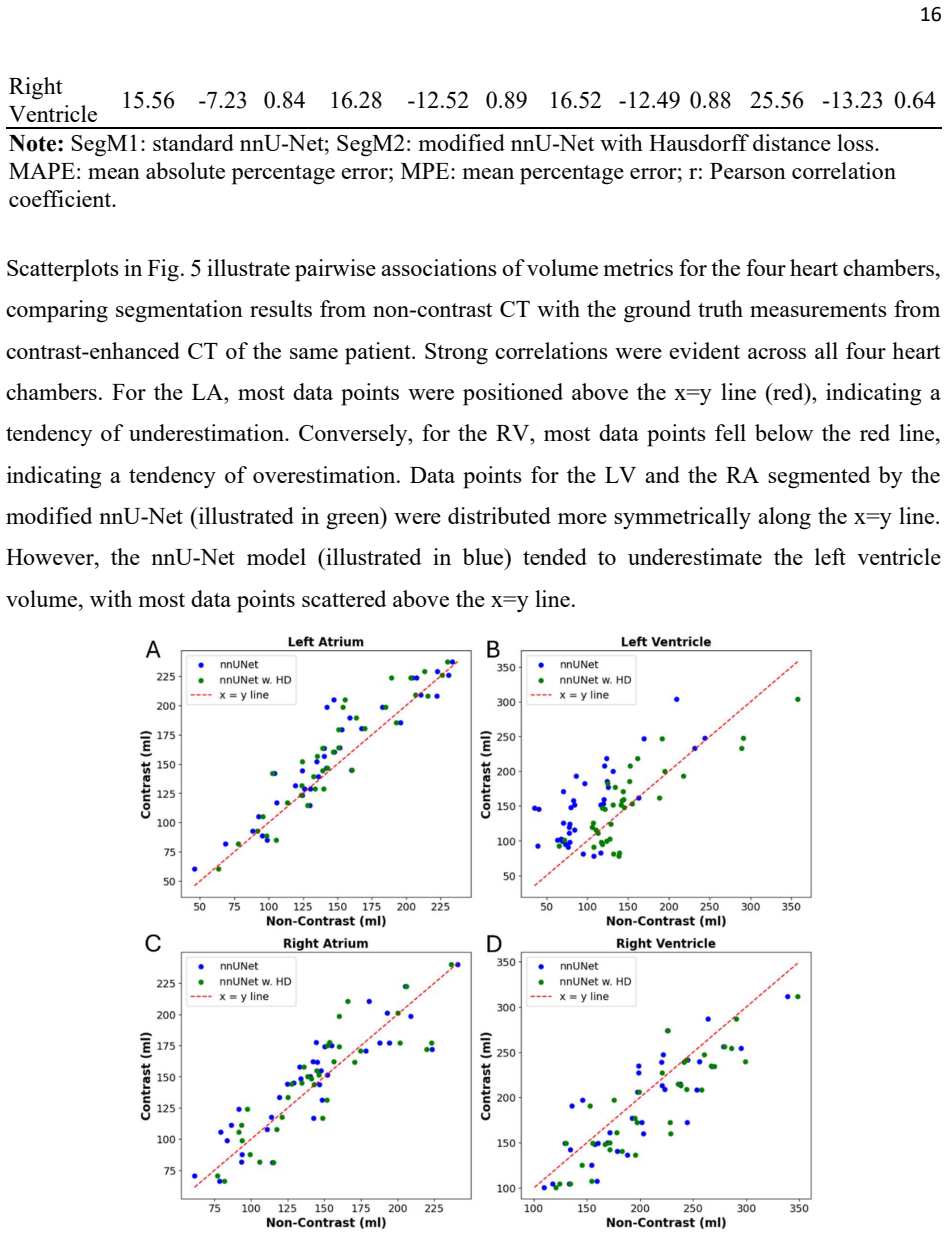
ChameleonNet uses contrastive unpaired translation to generate non-contrast CT images from contrast-enhanced ones, allowing a segmentation network trained on the synthetic images with chamber annotations from the original contrast scans to segment four heart chambers on non-contrast CT. On held-out synthetic non-contrast images the model reaches Dice scores of 0.91 to 0.94 and HD95 distances of 3.6 to 5.7 mm. On real non-contrast scans the predicted chamber volumes correlate with manual measurements at 0.82 to 0.93 while showing mean absolute percentage errors between 9 and 21 percent.
What carries the argument
Contrastive Unpaired Translation (CUT) network with decoupled contrastive learning loss for synthesizing non-contrast CT images, paired with a Hausdorff distance loss-enhanced nnU-Net segmentation model.
Load-bearing premise
The image translation step must preserve the true sizes and boundary locations of the heart chambers so that the segmentation model trained on synthetic data performs accurately on actual non-contrast scans.
What would settle it
Finding a dataset of real non-contrast CT scans with independent ground-truth chamber volumes where the predicted volumes show consistent bias larger than 20 percent or Dice scores below 0.80 would falsify the feasibility claim.
Figures
read the original abstract
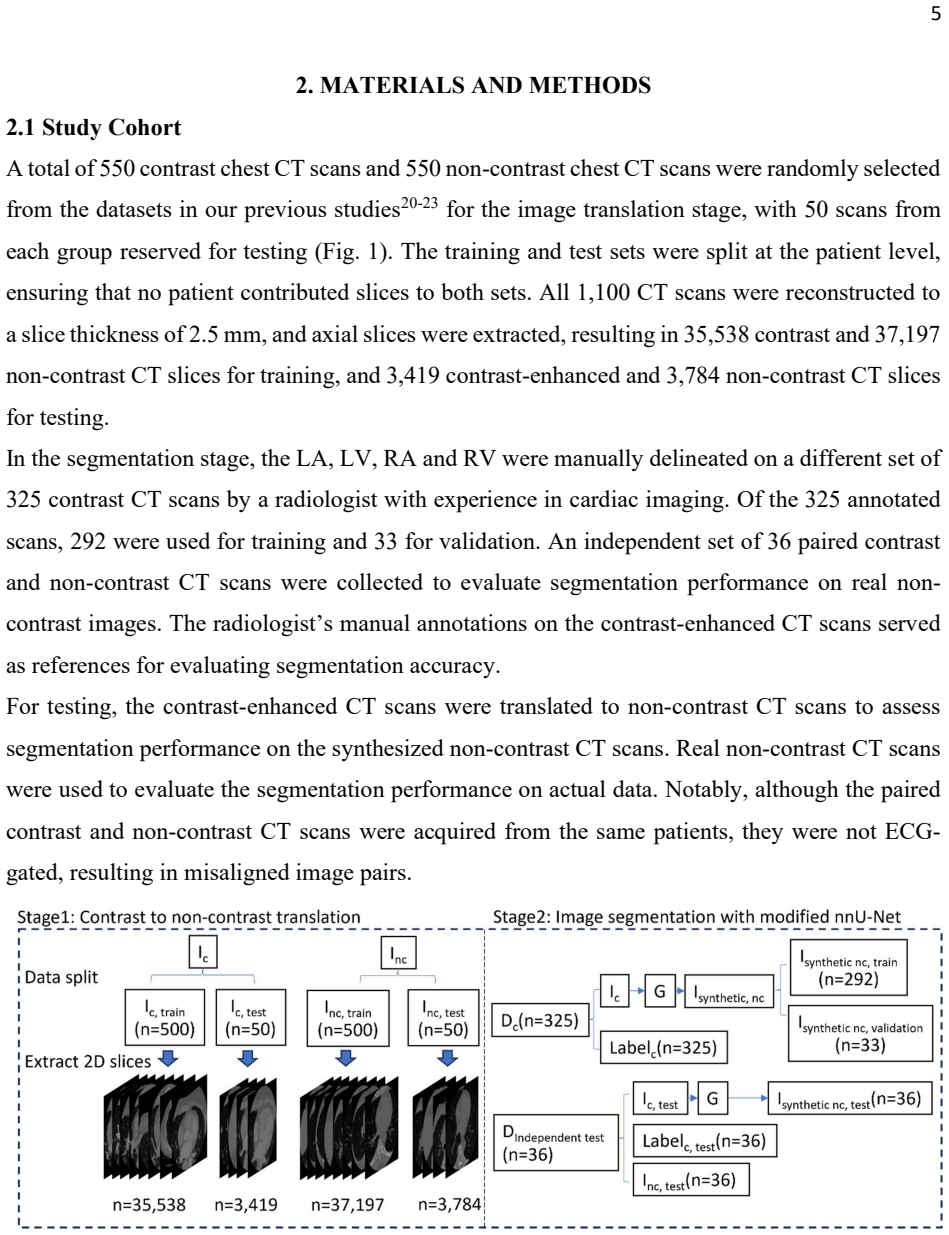
Purpose: To evaluate the feasibility and challenges of heart chamber segmentation from non-contrast CT scans using contrastive unpaired image translation and deep learning-based segmentation. Approach: We developed ChameleonNet, a framework utilizing the Contrastive Unpaired Translation (CUT) network with decoupled contrastive learning (DCL) loss to synthesize non-contrast CT from contrast CT scans. Using annotations of four heart chambers (left atrium (LA), left ventricle (LV), right atrium (RA), and right ventricle (RV)) from contrast scans, we trained a Hausdorff distance loss-enhanced nnU-Net on synthesized non-contrast images. The translation model was trained with 35,538 contrast-enhanced and 37,197 non-contrast CT slices. The segmentation model was trained with 292 synthesized non-contrast scans. Performance was evaluated using Dice similarity coefficient (DSC) and 95th Hausdorff distance (HD95) on 36 synthesized non-contrast scans, and volume agreement on 36 real non-contrast CT scans was assessed using Pearson correlation, mean absolute percentage error (MAPE), and mean percentage error (MPE). Results: The segmentation model achieved DSC of 0.94 (0.01), 0.91 (0.04), 0.92 (0.03), 0.93 (0.02), and HD95 of 3.63 (1.49), 5.74 (4.08), 5.18 (1.77), 5.51 (3.21) mm on synthesized non-contrast images for LA, LV, RA, and RV, respectively. On real non-contrast CT scans, Pearson correlations were 0.93, 0.82, 0.87, and 0.89 (all p<0.001), with MAPE ranging from 9.22% to 20.79%, and MPE ranging from -12.52% to 4.67%. Conclusions: ChameleonNet demonstrated feasibility for heart chamber segmentation from non-contrast CT without manual non-contrast annotations. However, volume errors, particularly for LV and RV, indicate that further refinement and validation are needed before clinical use.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper introduces ChameleonNet, which applies Contrastive Unpaired Translation (CUT) augmented with decoupled contrastive learning (DCL) to synthesize non-contrast CT slices from contrast-enhanced CT. Annotations of LA, LV, RA, and RV from the contrast scans are transferred to the synthesized non-contrast images to train a Hausdorff-distance-enhanced nnU-Net. Evaluation reports DSC 0.91–0.94 and HD95 3.6–5.7 mm on 36 held-out synthesized non-contrast cases, and Pearson correlations 0.82–0.93 (with MAPE 9–21 % and MPE down to –12.5 %) on 36 real non-contrast cases. The central claim is that this pipeline demonstrates feasibility for heart-chamber segmentation on non-contrast CT without requiring manual non-contrast annotations.
Significance. If the reported generalization holds, the work would provide a practical route to leverage abundant contrast-CT annotations for the more common non-contrast modality, reducing the annotation burden and contrast-related risks in cardiac CT analysis. The concrete numeric results on both synthesized and real data, together with the explicit acknowledgment of volume bias, constitute a transparent feasibility study that could guide subsequent refinement.
major comments (3)
- [Abstract / Results] Abstract / Results: DSC and HD95 are reported exclusively on the 36 synthesized non-contrast test cases; on the 36 real non-contrast cases only volume-derived Pearson, MAPE and MPE are supplied. Because no manual segmentations exist on the real non-contrast set, the claim that the model generalizes to real anatomy rests on an indirect proxy whose systematic errors (MAPE 20.79 %, MPE –12.52 % for LV/RV) already signal translation-induced size distortion. This gap directly affects the central feasibility assertion for clinical non-contrast scans.
- [Methods] Methods: The manuscript provides no patient-level data-split description, no statement on whether any of the 36 real non-contrast test cases overlap with the 35 538 / 37 197 training slices, and no details on statistical testing or multiple-comparison correction for the reported p<0.001 correlations. These omissions prevent independent assessment of data leakage and reproducibility.
- [Results] Results: The volume bias observed on real non-contrast scans (particularly LV and RV) is consistent with the known risk that unpaired CUT/DCL translation may alter chamber geometry even when image appearance is realistic. Without a direct segmentation accuracy metric on real data, it remains unclear whether the downstream nnU-Net inherits this geometric distortion.
minor comments (2)
- [Abstract] Abstract: the parenthetical standard deviations are given without clarifying whether they are computed across the 36 cases or across cross-validation folds.
- [Methods] The manuscript should explicitly state the number of patients (rather than slices) in each split to allow evaluation of inter-patient variability.
Simulated Author's Rebuttal
We thank the referee for the constructive feedback and for recognizing the transparency of our feasibility study. We address each major comment below, providing clarifications and committing to revisions that strengthen reproducibility and discussion of limitations without overstating the results.
read point-by-point responses
-
Referee: [Abstract / Results] DSC and HD95 reported only on 36 synthesized cases; real non-contrast cases use only volume proxies (Pearson 0.82-0.93, MAPE up to 20.79%, MPE -12.52% for LV/RV). No manual segmentations on real data means generalization claim rests on indirect proxy with evident systematic errors, affecting central feasibility assertion.
Authors: We agree that the lack of manual annotations on real non-contrast scans precludes direct DSC/HD95 evaluation and that volume metrics are an indirect proxy. This is inherent to the problem we address (no ground-truth labels on the target modality). The high correlations (all p<0.001) and the fact that volume is a primary clinical endpoint provide supporting evidence of generalization, but the observed biases (especially LV/RV) correctly signal translation-induced distortions. In revision we will clarify in the abstract and conclusions that feasibility is shown via synthesized metrics plus proxy validation, with explicit caveats that direct accuracy on real scans remains unproven. revision: partial
-
Referee: [Methods] No patient-level data-split description, no statement on overlap between 36 real non-contrast test cases and the 35,538/37,197 training slices, and no details on statistical testing or multiple-comparison correction for p<0.001 correlations.
Authors: These details were inadvertently omitted. The revised manuscript will add: (1) explicit patient-level splits confirming the 36 real non-contrast cases come from entirely separate patients with zero slice overlap to training data; (2) confirmation that all training slices are from distinct contrast-enhanced and non-contrast acquisitions; (3) statistical methods stating that Pearson correlations used standard two-tailed t-tests with p-values reported as-is (four comparisons, no correction applied). revision: yes
-
Referee: [Results] Volume bias on real scans (esp. LV/RV) consistent with known CUT/DCL risk of altering chamber geometry. Without direct segmentation metric on real data, unclear whether nnU-Net inherits this distortion.
Authors: We concur that unpaired translation can distort geometry even when appearance is realistic, and the MAPE/MPE values are consistent with this. Because the nnU-Net is trained exclusively on synthesized images with transferred labels, any geometric shift in the CUT output is inherited. The strong DSC on held-out synthesized cases indicates the segmentation network itself is robust when input quality is high. We will expand the discussion to explicitly link the observed volume errors to potential translation artifacts and outline future work using sparse manual labels on real scans for direct validation. revision: partial
Circularity Check
No significant circularity; empirical metrics are direct evaluations on held-out data
full rationale
The paper reports an empirical feasibility study using CUT+DCL for unpaired translation followed by nnU-Net segmentation. All reported numbers (DSC 0.91-0.94, HD95 3.63-5.74 mm on synthesized images; Pearson 0.82-0.93, MAPE 9.22-20.79% on real non-contrast scans) are obtained by direct evaluation on held-out image sets with no fitted parameters, no equations that define outputs in terms of inputs, and no load-bearing self-citations that reduce the central claim to prior author work. The derivation chain consists of standard network training and standard segmentation metrics; no step reduces by construction to its own inputs.
Axiom & Free-Parameter Ledger
free parameters (1)
- CUT and nnU-Net network weights
axioms (1)
- domain assumption Unpaired contrastive translation preserves the geometric features required for accurate chamber segmentation on real non-contrast scans
Reference graph
Works this paper leans on
-
[1]
Global trends and regional differences in incidence and mortality of cardiovascular disease, 1990− 2019: findings from 2019 global burden of disease study
Li Y, Cao G-y, Jing W-z, Liu J, Liu M. Global trends and regional differences in incidence and mortality of cardiovascular disease, 1990− 2019: findings from 2019 global burden of disease study. European journal of preventive cardiology. 2023;30(3):276-286
1990
-
[2]
Left atrial size and function: role in prognosis
Hoit BD. Left atrial size and function: role in prognosis. Journal of the American College of Cardiology. 2014;63(6):493-505
2014
-
[3]
Naghavi M, Yankelevitz D, Reeves AP, et al. AI-enabled left atrial volumetry in coronary artery calcium scans (AI-CACTM) predicts atrial fibrillation as early as one year, improves CHARGE-AF, and outperforms NT-proBNP: The multi-ethnic study of atherosclerosis. Journal of cardiovascular computed tomography. 2024
2024
-
[4]
AI-enabled cardiac chambers volumetry in coronary artery calcium scans (AI-CACTM) predicts heart failure and outperforms NT-proBNP: The multi- ethnic study of Atherosclerosis
Naghavi M, Reeves A, Budoff M, et al. AI-enabled cardiac chambers volumetry in coronary artery calcium scans (AI-CACTM) predicts heart failure and outperforms NT-proBNP: The multi- ethnic study of Atherosclerosis. Journal of Cardiovascular Computed Tomography. 2024
2024
-
[5]
Cardiac substructure delineation in radiation therapy–A state‐of‐the‐art review
Finnegan RN, Quinn A, Booth J, et al. Cardiac substructure delineation in radiation therapy–A state‐of‐the‐art review. Journal of Medical Imaging and Radiation Oncology. 2024
2024
-
[6]
Dose to heart substructures is associated with non-cancer death after SBRT in stage I–II NSCLC patients
Stam B, Peulen H, Guckenberger M, et al. Dose to heart substructures is associated with non-cancer death after SBRT in stage I–II NSCLC patients. Radiotherapy and Oncology. 2017;123(3):370-375
2017
-
[7]
Automatic segmentation and quantification of the cardiac structures from non-contrast-enhanced cardiac CT scans
Shahzad R, Bos D, Budde RP, et al. Automatic segmentation and quantification of the cardiac structures from non-contrast-enhanced cardiac CT scans. Physics in Medicine & Biology. 2017;62(9):3798
2017
-
[8]
Open-source, fully-automated hybrid cardiac substructure segmentation: development and optimisation
Finnegan RN, Chin V, Chlap P, et al. Open-source, fully-automated hybrid cardiac substructure segmentation: development and optimisation. Physical and Engineering Sciences in Medicine. 2023;46(1):377-393
2023
-
[9]
nnU-Net: a self-configuring method for deep learning-based biomedical image segmentation
Isensee F, Jaeger PF, Kohl SA, Petersen J, Maier-Hein KH. nnU-Net: a self-configuring method for deep learning-based biomedical image segmentation. Nature methods. 2021;18(2):203-211
2021
-
[10]
nnu-net revisited: A call for rigorous validation in 3d medical image segmentation
Isensee F, Wald T, Ulrich C, et al. nnu-net revisited: A call for rigorous validation in 3d medical image segmentation. Springer; 2024:488-498
2024
-
[11]
Deep learning–based automatic segmentation of cardiac substructures for lung cancers
Chen X, Mumme RP, Corrigan KL, et al. Deep learning–based automatic segmentation of cardiac substructures for lung cancers. Radiotherapy and Oncology. 2024;191:110061
2024
-
[12]
TotalSegmentator: robust segmentation of 104 anatomic structures in CT images
Wasserthal J, Breit H-C, Meyer MT, et al. TotalSegmentator: robust segmentation of 104 anatomic structures in CT images. Radiology: Artificial Intelligence. 2023;5(5)
2023
-
[13]
AI-based, automated chamber volumetry from gated, non-contrast CT
Jacob AJ, Abdelkarim O, Zook S, et al. AI-based, automated chamber volumetry from gated, non-contrast CT. Journal of Cardiovascular Computed Tomography. 2023;17(5):336-340
2023
-
[14]
Deep learning from dual‐energy information for whole‐heart segmentation in dual‐energy and single‐energy non‐contrast‐enhanced cardiac CT
Bruns S, Wolterink JM, Takx RA, et al. Deep learning from dual‐energy information for whole‐heart segmentation in dual‐energy and single‐energy non‐contrast‐enhanced cardiac CT. Medical physics. 2020;47(10):5048-5060
2020
-
[15]
Data augmentation using generative adversarial networks (CycleGAN) to improve generalizability in CT segmentation tasks
Sandfort V, Yan K, Pickhardt PJ, Summers RM. Data augmentation using generative adversarial networks (CycleGAN) to improve generalizability in CT segmentation tasks. Scientific reports. 2019;9(1):16884
2019
-
[16]
Unpaired image-to-image translation using cycle- consistent adversarial networks
Zhu J-Y, Park T, Isola P, Efros AA. Unpaired image-to-image translation using cycle- consistent adversarial networks. 2017:2223-2232. 25
2017
-
[17]
Super-resolution of cardiac MR cine imaging using conditional GANs and unsupervised transfer learning
Xia Y, Ravikumar N, Greenwood JP, Neubauer S, Petersen SE, Frangi AF. Super-resolution of cardiac MR cine imaging using conditional GANs and unsupervised transfer learning. Medical Image Analysis. 2021;71:102037
2021
-
[18]
Unsupervised multi-modal style transfer for cardiac MR segmentation
Chen C, Ouyang C, Tarroni G, et al. Unsupervised multi-modal style transfer for cardiac MR segmentation. Springer; 2020:209-219
2020
-
[19]
Contrastive learning for unpaired image-to-image translation
Park T, Efros AA, Zhang R, Zhu J-Y. Contrastive learning for unpaired image-to-image translation. Springer; 2020:319-345
2020
-
[20]
Pulmonary circulatory system characteristics are associated with future lung cancer risk
Pu J, Bandos A, Yu T, et al. Pulmonary circulatory system characteristics are associated with future lung cancer risk. Med Phys. Apr 2024;51(4):2589-2597. doi:10.1002/mp.16930
-
[21]
Pu J, Gezer NS, Ren S, et al. Automated detection and segmentation of pulmonary embolisms on computed tomography pulmonary angiography (CTPA) using deep learning but without manual outlining. Med Image Anal . Jul 14 2023;89:102882. doi:10.1016/j.media.2023.102882
-
[22]
CT-Derived Body Composition Is a Predictor of Survival after Esophagectomy
Iyer K, Beeche CA, Gezer NS, et al. CT-Derived Body Composition Is a Predictor of Survival after Esophagectomy. J Clin Med. Mar 8 2023;12(6)doi:10.3390/jcm12062106
-
[23]
A pilot study: quantify lung volume and emphysema extent directly from 2-D scout images
Pu J, Sechrist J, Meng x, Sciurba FC, Leader JK. A pilot study: quantify lung volume and emphysema extent directly from 2-D scout images. Medical Physics. 2021;48(8):4316-4325
2021
-
[24]
Representation learning with contrastive predictive coding
Oord Avd, Li Y, Vinyals O. Representation learning with contrastive predictive coding. arXiv preprint arXiv:180703748. 2018
2018
-
[25]
Decoupled contrastive learning
Yeh C-H, Hong C-Y, Hsu Y-C, Liu T-L, Chen Y, LeCun Y. Decoupled contrastive learning. Springer; 2022:668-684
2022
-
[26]
Generative adversarial networks
Goodfellow I, Pouget-Abadie J, Mirza M, et al. Generative adversarial networks. Communications of the ACM. 2020;63(11):139-144
2020
-
[27]
Reducing the hausdorff distance in medical image segmentation with convolutional neural networks
Karimi D, Salcudean SE. Reducing the hausdorff distance in medical image segmentation with convolutional neural networks. IEEE Transactions on medical imaging. 2019;39(2):499-513
2019
-
[28]
Image-to-image translation with conditional adversarial networks
Isola P, Zhu J-Y, Zhou T, Efros AA. Image-to-image translation with conditional adversarial networks. 2017:1125-1134
2017
-
[29]
Least squares generative adversarial networks
Mao X, Li Q, Xie H, Lau RY, Wang Z, Paul Smolley S. Least squares generative adversarial networks. 2017:2794-2802
2017
-
[30]
Loss odyssey in medical image segmentation
Ma J, Chen J, Ng M, et al. Loss odyssey in medical image segmentation. Medical Image Analysis. 2021;71:102035
2021
-
[31]
Image quality assessment: from error visibility to structural similarity
Wang Z, Bovik AC, Sheikh HR, Simoncelli EP. Image quality assessment: from error visibility to structural similarity. IEEE transactions on image processing. 2004;13(4):600-612
2004
-
[32]
Gans trained by a two time- scale update rule converge to a local nash equilibrium
Heusel M, Ramsauer H, Unterthiner T, Nessler B, Hochreiter S. Gans trained by a two time- scale update rule converge to a local nash equilibrium. Advances in neural information processing systems. 2017;30
2017
-
[33]
ECG-gated cardiac CT
Desjardins B, Kazerooni EA. ECG-gated cardiac CT. American Journal of Roentgenology. 2004;182(4):993-1010
2004
-
[34]
Total heart volume variation throughout the cardiac cycle in humans
Carlsson M, Cain P, Holmqvist C, Stahlberg F, Lundback S, Arheden H. Total heart volume variation throughout the cardiac cycle in humans. American Journal of Physiology-Heart and Circulatory Physiology. 2004;287(1):H243-H250
2004
-
[35]
Structure-driven unsupervised domain adaptation for cross- modality cardiac segmentation
Cui Z, Li C, Du Z, et al. Structure-driven unsupervised domain adaptation for cross- modality cardiac segmentation. IEEE Transactions on Medical Imaging. 2021;40(12):3604-3616. 26
2021
-
[36]
Feature extraction for generative medical imaging evaluation: New evidence against an evolving trend
Woodland M, Castelo A, Al Taie M, et al. Feature extraction for generative medical imaging evaluation: New evidence against an evolving trend. Springer; 2024:87-97
2024
-
[37]
Elastix: a toolbox for intensity-based medical image registration
Klein S, Staring M, Murphy K, Viergever MA, Pluim JP. Elastix: a toolbox for intensity-based medical image registration. IEEE transactions on medical imaging. 2009;29(1):196-205
2009
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.