DSA-NRP: No-Reflow Prediction from Angiographic Perfusion Dynamics in Stroke EVT
Pith reviewed 2026-05-19 07:49 UTC · model grok-4.3
The pith
Perfusion features from DSA sequences predict no-reflow after successful EVT more accurately than clinical variables.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
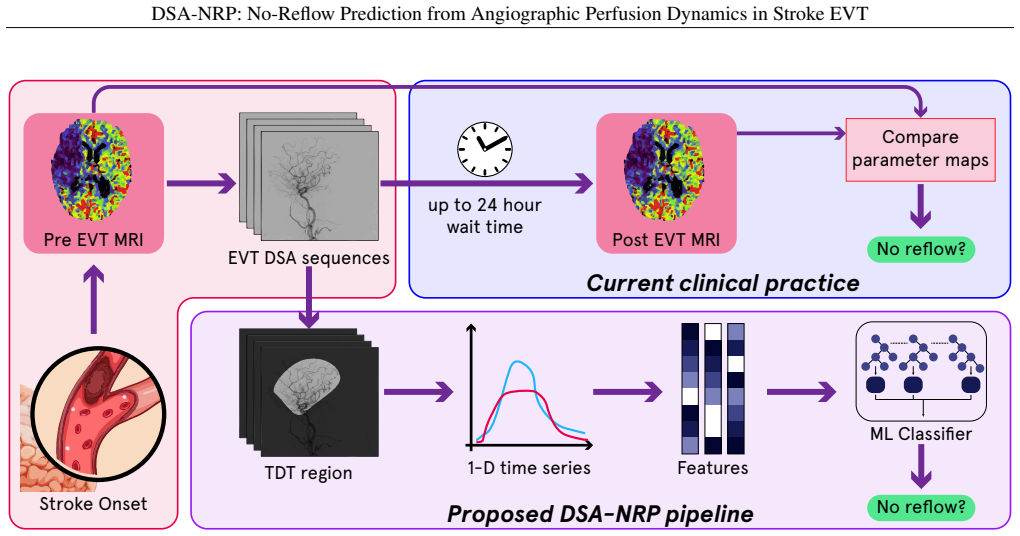
The authors claim that statistical and temporal perfusion features extracted from pre- and post-EVT DSA sequences in the target downstream territory allow ML classifiers to predict no-reflow, defined as persistent hypoperfusion on post-procedure MRI, with an AUC of 0.7703 compared to 0.5728 for clinical features alone, in patients who achieved good recanalization scores.
What carries the argument
Machine learning classifiers trained on statistical and temporal perfusion features from angiographic sequences of the target territory.
If this is right
- Clinicians could identify high-risk patients immediately after EVT for proactive management.
- Intra-procedural DSA data provides real-time insights into microvascular integrity.
- This reduces dependence on delayed perfusion MRI for no-reflow detection.
- The framework lays groundwork for integrating such predictions into acute stroke care workflows.
Where Pith is reading between the lines
- If validated, this approach might be extended to predict other post-EVT complications like hemorrhage using similar DSA analysis.
- It could influence the design of future EVT protocols to include automated perfusion feature extraction.
- A testable extension would be applying the model to multi-center data to check generalizability.
Load-bearing premise
The features from DSA sequences capture microvascular integrity separately from whether the main artery was successfully opened.
What would settle it
A follow-up study in which the DSA model shows no better performance than the clinical baseline on new patient data would disprove the advantage.
Figures



read the original abstract
Following successful large-vessel recanalization via endovascular thrombectomy (EVT) for acute ischemic stroke (AIS), some patients experience a complication known as no-reflow, defined by persistent microvascular hypoperfusion that undermines tissue recovery and worsens clinical outcomes. Although prompt identification is crucial, standard clinical practice relies on perfusion magnetic resonance imaging (MRI) within 24 hours post-procedure, delaying intervention. In this work, we introduce the first-ever machine learning (ML) framework to predict no-reflow immediately after EVT by leveraging previously unexplored intra-procedural digital subtraction angiography (DSA) sequences and clinical variables. Our retrospective analysis included AIS patients treated at UCLA Medical Center (2011-2024) who achieved favorable mTICI scores (2b-3) and underwent pre- and post-procedure MRI. No-reflow was defined as persistent hypoperfusion (Tmax > 6 s) on post-procedural imaging. From DSA sequences (AP and lateral views), we extracted statistical and temporal perfusion features from the target downstream territory to train ML classifiers for predicting no-reflow. Our novel method significantly outperformed a clinical-features baseline(AUC: 0.7703 $\pm$ 0.12 vs. 0.5728 $\pm$ 0.12; accuracy: 0.8125 $\pm$ 0.10 vs. 0.6331 $\pm$ 0.09), demonstrating that real-time DSA perfusion dynamics encode critical insights into microvascular integrity. This approach establishes a foundation for immediate, accurate no-reflow prediction, enabling clinicians to proactively manage high-risk patients without reliance on delayed imaging.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper introduces DSA-NRP, an ML framework that extracts statistical and temporal perfusion features from pre- and post-EVT DSA sequences (AP and lateral views) of the target downstream territory, combined with clinical variables, to predict no-reflow (Tmax > 6 s on post-procedural MRI) in mTICI 2b-3 patients. In a retrospective UCLA cohort (2011-2024), the model reports AUC 0.7703 ± 0.12 and accuracy 0.8125 ± 0.10, outperforming a clinical-features baseline (AUC 0.5728 ± 0.12, accuracy 0.6331 ± 0.09), claiming that DSA dynamics encode microvascular integrity for immediate prediction.
Significance. If the reported performance gain proves robust under pre-specified protocols and proper validation, the work could enable real-time intra-procedural no-reflow risk stratification, reducing reliance on delayed post-EVT MRI and supporting earlier intervention. The novelty of leveraging intra-procedural DSA perfusion dynamics is a clear strength, though the single-center retrospective design and limited methodological transparency temper immediate clinical impact.
major comments (2)
- [Abstract/Methods] Abstract/Methods: No pre-specified protocol is described for defining the target downstream territory, selecting AP vs. lateral views, or setting time-window boundaries for feature extraction. This leaves open the possibility that territory masks or windows were refined after inspecting MRI labels or outcomes, which would make the AUC improvement (0.7703 vs. 0.5728) potentially artifactual rather than evidence that DSA dynamics independently capture microvascular integrity after successful recanalization.
- [Results] Results: Only aggregate AUC and accuracy with standard deviations are presented; the manuscript provides no details on cross-validation folds, stratification, feature selection procedure, or class-imbalance handling. Without these, the statistical reliability of the headline comparison to the clinical baseline cannot be assessed and the central claim remains difficult to evaluate.
minor comments (1)
- [Abstract] Abstract: The total number of patients, no-reflow prevalence, and exact clinical features used in the baseline are not stated, which are needed to interpret the reported metrics and baseline performance.
Simulated Author's Rebuttal
We thank the referee for the thoughtful and constructive review. The comments highlight important aspects of methodological transparency that we address point by point below. We have revised the manuscript to provide the requested details on protocol definition and validation procedures while preserving the integrity of the original analysis.
read point-by-point responses
-
Referee: [Abstract/Methods] Abstract/Methods: No pre-specified protocol is described for defining the target downstream territory, selecting AP vs. lateral views, or setting time-window boundaries for feature extraction. This leaves open the possibility that territory masks or windows were refined after inspecting MRI labels or outcomes, which would make the AUC improvement (0.7703 vs. 0.5728) potentially artifactual rather than evidence that DSA dynamics independently capture microvascular integrity after successful recanalization.
Authors: We agree that explicit documentation of the analysis protocol is essential to rule out post-hoc refinement. The target downstream territory was defined a priori as the vascular bed distal to the site of large-vessel occlusion, identified on the initial diagnostic DSA run using standard anatomical landmarks (e.g., MCA territory for M1 occlusions). AP and lateral projections were chosen because they constitute the routine biplane acquisitions performed during EVT at our center; no post-MRI selection occurred. Time windows were fixed to the full contrast transit phase (injection to venous clearance, typically 4–12 s) based on prior angiographic literature rather than outcome inspection. Nevertheless, to eliminate any ambiguity we have added a new subsection titled “Target Territory Definition and View Selection Protocol” in the Methods that codifies these rules with explicit exclusion criteria and timing parameters. We also include a supplementary figure illustrating example territory masks. revision: yes
-
Referee: [Results] Results: Only aggregate AUC and accuracy with standard deviations are presented; the manuscript provides no details on cross-validation folds, stratification, feature selection procedure, or class-imbalance handling. Without these, the statistical reliability of the headline comparison to the clinical baseline cannot be assessed and the central claim remains difficult to evaluate.
Authors: We acknowledge that the original Results section omitted the granular validation details required for independent assessment. The reported figures derive from 5-fold stratified cross-validation with folds balanced by no-reflow label (prevalence ~28 %). Stratification was performed at the patient level to avoid leakage across pre- and post-EVT sequences from the same individual. Feature selection used recursive feature elimination with cross-validation inside each outer fold; the final feature set was locked before evaluating the clinical baseline. Class imbalance was addressed by class-weighted logistic regression and random-forest variants; no synthetic oversampling was applied. We have expanded the Results section with a dedicated paragraph describing the full pipeline, added a supplementary table listing per-fold AUCs, and included a CONSORT-style flow diagram of the modeling steps. These additions allow direct evaluation of the 0.77 vs. 0.57 AUC difference. revision: yes
Circularity Check
No circularity: standard empirical ML prediction on held-out data
full rationale
The paper presents an empirical machine learning classifier that extracts statistical and temporal perfusion features from pre- and post-EVT DSA sequences in the target downstream territory and trains models to predict no-reflow (defined via post-procedural MRI Tmax > 6 s). Performance is reported with standard deviations consistent with cross-validation or held-out testing (AUC 0.7703 ± 0.12 vs baseline 0.5728 ± 0.12). No equations, derivations, or first-principles results are described that reduce the output to an input quantity by construction. No self-citations, uniqueness theorems, or ansatzes are invoked to justify the feature set or model; the central claim rests on direct comparison of classifier accuracy against a clinical-features baseline using standard ML practices.
Axiom & Free-Parameter Ledger
free parameters (1)
- ML classifier hyperparameters
axioms (1)
- domain assumption No-reflow is correctly defined by persistent Tmax > 6 s on post-procedural perfusion MRI.
Reference graph
Works this paper leans on
-
[1]
Global Epidemiology of Stroke and Access to Acute Ischemic Stroke Interventions Neurology
Saini Vasu, Guada Luis, Yavagal Dileep R.. Global Epidemiology of Stroke and Access to Acute Ischemic Stroke Interventions Neurology. 2021;97
work page 2021
-
[2]
Kim Joosup, Olaiya Muideen T, De Silva Deidre A, et al. Global stroke statistics 2023: Availability of reperfusion services around the world International Journal of Stroke. 2024;19:253–270
work page 2023
-
[3]
Karonen Jari O., Vanninen Ritva L., Liu Yawu, et al. Combined Diffusion and Perfusion MRI With Correlation to Single- Photon Emission CT in Acute Ischemic Stroke: Ischemic Penumbra Predicts Infarct Growth Stroke. 1999;30:1583–1590
work page 1999
-
[4]
Endovascular Thrombectomy for Acute Ischemic Stroke: A Meta-analysis JAMA
Badhiwala Jetan H., Nassiri Farshad, Alhazzani Waleed, et al. Endovascular Thrombectomy for Acute Ischemic Stroke: A Meta-analysis JAMA. 2015;314:1832
work page 2015
-
[5]
Ganesh Aravind, Goyal Mayank. Thrombectomy for Acute Ischemic Stroke: Recent Insights and Future Directions Current Neurology and Neuroscience Reports. 2018;18:59
work page 2018
-
[6]
Hyperacute Management of Ischemic Strokes Journal of the American College of Cardiology
Patel Pratit, Yavagal Dileep, Khandelwal Priyank. Hyperacute Management of Ischemic Strokes Journal of the American College of Cardiology. 2020;75:1844–1856
work page 2020
-
[7]
Mujanovic Adnan, Ng Felix, Meinel Thomas R, et al. No-reflow phenomenon in stroke patients: A systematic literature review and meta-analysis of clinical data International Journal of Stroke. 2024;19:58–67
work page 2024
-
[8]
Horie Nobutaka, Inoue Manabu, Morimoto Takeshi, et al. Recanalization Does Not Always Equate to Reperfusion: No-Reflow Phenomenon After Successful Thrombectomy Stroke. 2025;56:183–189
work page 2025
-
[9]
Schiphorst Adrien Ter, Charron Sylvain, Hassen Wagih Ben, et al. Tissueno-reflow despite full recanalization following thrombectomy for anterior circulation stroke with proximal occlusion: A clinical study Journal of Cerebral Blood Flow & Metabolism. 2021;41:253–266
work page 2021
-
[10]
Ng Felix C., Churilov Leonid, Yassi Nawaf, et al. Prevalence and Significance of Impaired Microvascular Tissue Reperfusion Despite Macrovascular Angiographic Reperfusion (No-Reflow) Neurology. 2022;98. 10 DSA-NRP: No-Reflow Prediction from Angiographic Perfusion Dynamics in Stroke EVT
work page 2022
-
[11]
Liebeskind David S, Bracard Serge, Guillemin Francis, et al. eTICI reperfusion: defining success in endovascular stroke therapy Journal of NeuroInterventional Surgery. 2019;11:433–438
work page 2019
-
[12]
Mujanovic Adnan, Kammer Christoph, Kurmann Christoph C., et al. Association of Intravenous Thrombolysis with Delayed Reperfusion After Incomplete Mechanical Thrombectomy Clinical Neuroradiology. 2023;33:87–98
work page 2023
-
[13]
Powers William J., Derdeyn Colin P., Biller José, et al. 2015 American Heart Association/American Stroke Association Focused Update of the 2013 Guidelines for the Early Management of Patients With Acute Ischemic Stroke Regarding Endovascular Treatment: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association...
work page 2015
-
[14]
Cho Yong-Hwan, Choi Jae Hyung. Mechanical thrombectomy for acute ischemic stroke with occlusion of the M2 segment of the middle cerebral artery: A literature review Journal of Cerebrovascular and Endovascular Neurosurgery. 2021;23:193–200
work page 2021
-
[15]
Liyis Bryan Gervais De, Surya Stevanus Christian, Tedyanto Eric Hartono, Pramana Nyoman Angga Krishna, Widyadharma I. Putu Eka. Mechanical thrombectomy in M1 and M2 segments of middle cerebral arteries: A meta-analysis of prospective cohort studies Clinical Neurology and Neurosurgery. 2023;231:107823
work page 2023
-
[16]
Endovascular Treatment of Stroke Due to Medium-Vessel Occlusion New England Journal of Medicine
Goyal Mayank, Ospel Johanna M., Ganesh Aravind, et al. Endovascular Treatment of Stroke Due to Medium-Vessel Occlusion New England Journal of Medicine. 2025;392:1385–1395
work page 2025
-
[17]
Kan Yuan, Li Sijie, Zhang Bowei, Ding Yuchuan, Zhao Wenbo, Ji Xunming. No-reflow phenomenon following stroke recanalization therapy: Clinical assessment advances: A narrative review Brain Circulation. 2023;9:214–221
work page 2023
-
[18]
Abdalkader Mohamad, Siegler James E., Lee Jin Soo, et al. Neuroimaging of Acute Ischemic Stroke: Multimodal Imaging Approach for Acute Endovascular Therapy Journal of Stroke. 2023;25:55–71
work page 2023
-
[19]
Arnould Marie-Cécile, Grandin Cécile B., Peeters André, Cosnard Guy, Duprez Thierry P.. Comparison of CT and three MR sequences for detecting and categorizing early (48 hours) hemorrhagic transformation in hyperacute ischemic stroke AJNR. American journal of neuroradiology. 2004;25:939–944
work page 2004
-
[20]
Comparative Sensitivity of Computed Tomography vs
Hwang David Y ., Silva Gisele S., Furie Karen L., Greer David M.. Comparative Sensitivity of Computed Tomography vs. Magnetic Resonance Imaging for Detecting Acute Posterior Fossa Infarct The Journal of Emergency Medicine. 2012;42:559–565
work page 2012
-
[21]
Sheriff Faheem, Castro Pedro, Kozberg Mariel, et al. Dynamic Cerebral Autoregulation Post Endovascular Thrombectomy in Acute Ischemic Stroke Brain Sciences. 2020;10:641
work page 2020
-
[22]
Migdady Ibrahim, Johnson-Black Phoebe H., Leslie-Mazwi Thabele, Malhotra Rishi. Current and Emerging Endovascular and Neurocritical Care Management Strategies in Large-Core Ischemic Stroke Journal of Clinical Medicine. 2023;12:6641
work page 2023
-
[23]
Blood Pressure Management After Endovascular Thrombectomy Frontiers in Neurology
Peng Teng J., Ortega-Gutiérrez Santiago, De Havenon Adam, Petersen Nils H.. Blood Pressure Management After Endovascular Thrombectomy Frontiers in Neurology. 2021;12:723461
work page 2021
-
[24]
Dong Xiao, Liu Yuanyuan, Chu Xuehong, et al. Blood pressure management after endovascular thrombectomy: Insights of recent randomized controlled trials CNS Neuroscience & Therapeutics. 2024;30:e14907
work page 2024
-
[25]
Svilaas Tone, Vlaar Pieter J., Van Der Horst Iwan C., et al. Thrombus Aspiration during Primary Percutaneous Coronary Intervention New England Journal of Medicine. 2008;358:557–567
work page 2008
-
[26]
Kaesmacher Johannes, Bellwald Sebastian, Dobrocky Tomas, et al. Safety and Efficacy of Intra-arterial Urokinase After Failed, Unsuccessful, or Incomplete Mechanical Thrombectomy in Anterior Circulation Large-Vessel Occlusion Stroke JAMA Neurology. 2020;77:318
work page 2020
-
[27]
Renú Arturo, Millán Mónica, San Román Luis, et al. Effect of Intra-arterial Alteplase vs Placebo Following Successful Thrombectomy on Functional Outcomes in Patients With Large Vessel Occlusion Acute Ischemic Stroke: The CHOICE Randomized Clinical Trial JAMA. 2022;327:826
work page 2022
-
[28]
P., Van Der Sluijs Matthijs, et al
Su Ruisheng, Cornelissen Sandra A. P., Van Der Sluijs Matthijs, et al. autoTICI: Automatic Brain Tissue Reperfusion Scoring on 2D DSA Images of Acute Ischemic Stroke Patients IEEE Transactions on Medical Imaging. 2021;40:2380– 2391
work page 2021
-
[29]
Huang Shuangfeng, Xu Jiali, Kang Haijuan, et al. A Comprehensive Prediction Model for Futile Recanalization in AIS Patients Post-Endovascular Therapy: Integrating Clinical, Imaging, and No-Reflow Biomarkers.Aging and disease. 2024;15:2852–2862. Place: United States
work page 2024
-
[30]
No-reflow phenomenon in acute ischemic stroke: an angiographic evaluation Neurological Sciences
Nicolini Ettore, Iacobucci Marta, De Michele Manuela, et al. No-reflow phenomenon in acute ischemic stroke: an angiographic evaluation Neurological Sciences. 2023;44:3939–3948
work page 2023
-
[31]
Prasetya Haryadi, Ramos Lucas A, Epema Thabiso, et al. qTICI: Quantitative assessment of brain tissue reperfusion on digital subtraction angiograms of acute ischemic stroke patients International Journal of Stroke. 2021;16:207–216. 11 DSA-NRP: No-Reflow Prediction from Angiographic Perfusion Dynamics in Stroke EVT
work page 2021
-
[32]
Sun Yu, Jou Eric, Nguyen Thanh N., et al. Predictors of futile recanalization after endovascular treatment in acute ischemic stroke: a multi-center study Frontiers in Neuroscience. 2023;17:1279366
work page 2023
-
[33]
Sabieleish Muhannad, Thormann Maximilian, Metzler Jonathan, et al. Image processing-based mTICI grading after endovascular treatment for acute ischemic stroke Current Directions in Biomedical Engineering. 2021;7:235–238
work page 2021
-
[34]
Mittmann Benjamin J., Braun Michael, Runck Frank, et al. Deep learning-based classification of DSA image sequences of patients with acute ischemic stroke International Journal of Computer Assisted Radiology and Surgery. 2022;17:1633– 1641
work page 2022
-
[35]
Zhang Haoyue, Polson Jennifer, Nael Kambiz, et al. A Machine Learning Approach to Predict Acute Ischemic Stroke Thrombectomy Reperfusion using Discriminative MR Image Features in 2021 IEEE EMBS International Conference on Biomedical and Health Informatics (BHI)(Athens, Greece):1–4IEEE 2021
work page 2021
-
[36]
Zhang Haoyue, Polson Jennifer S., Wang Zichen, et al. A Deep Learning Approach to Predict Recanalization First-Pass Effect following Mechanical Thrombectomy in Patients with Acute Ischemic Stroke American Journal of Neuroradiology. 2024;45:1044–1052
work page 2024
-
[37]
Da Ros Valerio, Cavallo Armando, Di Donna Carlo, et al. Ensemble machine learning to predict futile recanalization after mechanical thrombectomy based on non-contrast CT imaging Journal of Stroke and Cerebrovascular Diseases. 2024;33:107890
work page 2024
-
[38]
Kelly Brendan, Martinez Mesha, Do Huy, et al. DEEP MOVEMENT: Deep learning of movie files for management of endovascular thrombectomy European Radiology. 2023;33:5728–5739
work page 2023
-
[39]
CVFSNet: A Cross View Fusion Scoring Network for end-to-end mTICI scoring Medical Image Analysis
Xu Weijin, Tan Tao, Yang Huihua, et al. CVFSNet: A Cross View Fusion Scoring Network for end-to-end mTICI scoring Medical Image Analysis. 2025;102:103508
work page 2025
-
[40]
Rubiera Marta, Garcia-Tornel Alvaro, Olivé-Gadea Marta, et al. Computed Tomography Perfusion After Thrombectomy: An Immediate Surrogate Marker of Outcome After Recanalization in Acute Stroke Stroke. 2020;51:1736–1742
work page 2020
-
[41]
Jann Kay, Hauf Martinus, Kellner Weldon Frauke, et al. Implication of cerebral circulation time in intracranial stenosis measured by digital subtraction angiography on cerebral blood flow estimation measured by arterial spin labelingDiagnostic and Interventional Radiology. 2016;22:481–488
work page 2016
-
[42]
Lee Han-Jui, Hong Jia-Sheng, Lin Chung-Jung, et al. Automatic flow analysis of digital subtraction angiography using independent component analysis in patients with carotid stenosis PLOS ONE. 2017;12:e0185330
work page 2017
-
[43]
Lu Yun-Hao, Cai Yan, Zhang Yi, Wang Rui, Li Zhi-Yong. Digital Subtraction Angiography Contrast Material Transport as a Direct Assessment for Blood Perfusion of Middle Cerebral Artery Stenosis Frontiers in Physiology. 2021;12:716173. 12
work page 2021
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.