Cardiovascular disease classification using radiomics and geometric features from cardiac CT
Pith reviewed 2026-05-19 07:54 UTC · model grok-4.3
The pith
Radiomic and geometric features extracted via cardiac CT segmentation and atlas registration improve cardiovascular disease classification accuracy to 87.5 percent.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
Generating anatomical segmentations and registering images to a normative healthy atlas allows extraction of radiomic features together with geometric features from deformation fields; these features support a downstream classifier that reaches 87.50 percent accuracy on the public ASOCA dataset, outperforming models trained on raw CT images at 67.50 percent.
What carries the argument
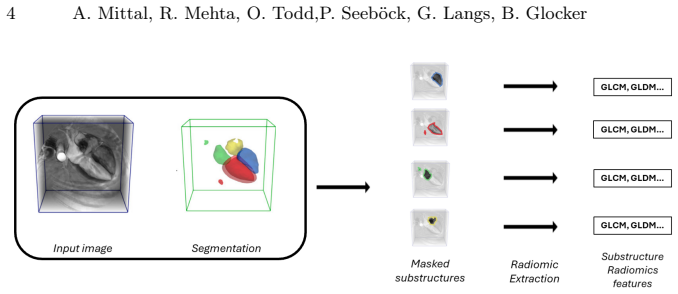
Radiomic features computed on segmentations from foundational models combined with geometric features derived from deformation fields produced by atlas registration to a normative healthy atlas, supplying interpretable inputs to the classifier.
If this is right
- The decomposed pipeline yields classifications that are easier to interpret clinically than those from raw-image models.
- Performance improves over direct training on raw CT data when the derived features are used.
- The method reuses existing foundational segmentation models and registration frameworks rather than training everything end-to-end.
- Results are demonstrated on the publicly available ASOCA dataset with released code.
Where Pith is reading between the lines
- The explicit geometric features could help identify which specific deformations or shape changes most strongly signal particular forms of cardiovascular disease.
- The same radiomic-plus-geometric pipeline could be tested on other CT-based classification tasks such as lung or liver lesion detection.
- Combining these imaging features with routine clinical variables might further raise diagnostic reliability in prospective studies.
- Robustness checks across different scanner vendors or acquisition protocols would clarify how far the accuracy gain generalizes.
Load-bearing premise
The automated segmentations and atlas-registration deformation fields must be accurate enough to encode clinically discriminative information without introducing systematic errors that would mislead the classifier.
What would settle it
A controlled experiment on the same or matched ASOCA-style data showing that a classifier trained on the extracted radiomic and geometric features performs no better than, or worse than, one trained on raw CT images would falsify the central performance claim.
Figures


read the original abstract
Automatic detection and classification of Cardiovascular disease (CVD) from Computed Tomography (CT) images play an important part in facilitating better-informed clinical decisions. However, most of the recent deep learning based methods either directly work on raw CT data or utilize it in pair with anatomical cardiac structure segmentation by training an end-to-end classifier. As such, these approaches become much more difficult to interpret from a clinical perspective. To address this challenge, in this work, we break down the CVD classification pipeline into three components: (i) image segmentation, (ii) image registration, and (iii) downstream CVD classification. Specifically, we utilize the Atlas-ISTN framework and recent segmentation foundational models to generate anatomical structure segmentation and a normative healthy atlas. These are further utilized to extract clinically interpretable radiomic features as well as deformation field based geometric features (through atlas registration) for CVD classification. Our experiments on the publicly available ASOCA dataset show that utilizing these features leads to better CVD classification accuracy (87.50\%) when compared against classification model trained directly on raw CT images (67.50\%). Our code is publicly available: https://github.com/biomedia-mira/grc-net
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
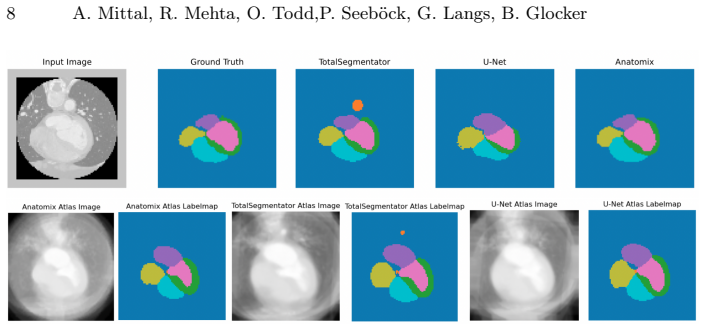
Summary. The manuscript proposes decomposing CVD classification from cardiac CT into three stages: segmentation of anatomical structures via foundational models, atlas-based registration using Atlas-ISTN to produce a normative healthy atlas and deformation fields, and extraction of radiomic plus geometric features for a downstream classifier. Experiments on the public ASOCA dataset report 87.50% classification accuracy using these features versus 67.50% for a model trained directly on raw CT images, with code released publicly.
Significance. If the reported accuracy improvement holds under proper validation, the work supplies a clinically more interpretable pipeline than end-to-end deep learning by grounding predictions in radiomic and deformation-derived geometric features. Public dataset use and open code are positive for reproducibility; the modular design could facilitate clinical adoption if upstream segmentation and registration quality are demonstrated on the target data.
major comments (2)
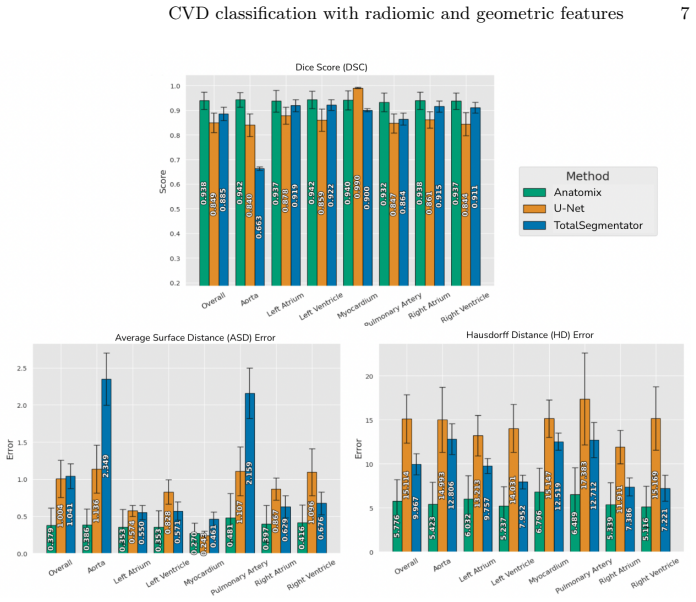
- [Methods / pipeline description] Pipeline description (Methods section): The central accuracy claim (87.50% vs 67.50%) rests on the premise that foundational-model segmentations and Atlas-ISTN deformation fields are sufficiently accurate and free of systematic errors on ASOCA volumes. No dataset-specific quantitative validation is supplied (e.g., Dice coefficients, surface distances, or registration metrics such as Jacobian statistics or landmark errors), leaving open the possibility that the 20-point gap partly reflects artifacts rather than feature informativeness.
- [Results / experimental setup] Experimental results (Results section): The abstract and results report raw accuracy numbers without describing the cross-validation strategy, statistical significance testing of the improvement, class-imbalance handling, or ablation isolating radiomic versus geometric feature groups. These omissions make the superiority claim difficult to evaluate and undermine in the reported performance difference.
minor comments (3)
- [Methods] Specify the exact foundational segmentation models employed and whether any domain-specific fine-tuning or post-processing was applied to the ASOCA CT data.
- [Methods] Clarify the classifier architecture, hyper-parameter selection, and feature dimensionality reduction steps used for the radiomic/geometric feature set.
- [Experiments] Add a brief description of the ASOCA dataset composition (number of cases, class distribution, acquisition parameters) to contextualize the reported accuracies.
Simulated Author's Rebuttal
We thank the referee for the constructive feedback on our manuscript. We address each major comment below and outline the revisions we will make to improve clarity and rigor.
read point-by-point responses
-
Referee: [Methods / pipeline description] Pipeline description (Methods section): The central accuracy claim (87.50% vs 67.50%) rests on the premise that foundational-model segmentations and Atlas-ISTN deformation fields are sufficiently accurate and free of systematic errors on ASOCA volumes. No dataset-specific quantitative validation is supplied (e.g., Dice coefficients, surface distances, or registration metrics such as Jacobian statistics or landmark errors), leaving open the possibility that the 20-point gap partly reflects artifacts rather than feature informativeness.
Authors: We agree that dataset-specific quantitative validation of the segmentation and registration components on ASOCA is important to support the accuracy claims. The manuscript relies on the established performance of the foundational segmentation models and Atlas-ISTN from their original publications but does not report ASOCA-specific metrics such as Dice scores or Jacobian statistics. In the revised manuscript we will add these evaluations in the Methods section, computing and reporting Dice coefficients for the anatomical segmentations and registration quality metrics (e.g., mean Jacobian determinants and overlap after warping) on the ASOCA volumes to demonstrate that upstream steps are reliable and that the observed improvement is attributable to the extracted features. revision: yes
-
Referee: [Results / experimental setup] Experimental results (Results section): The abstract and results report raw accuracy numbers without describing the cross-validation strategy, statistical significance testing of the improvement, class-imbalance handling, or ablation isolating radiomic versus geometric feature groups. These omissions make the superiority claim difficult to evaluate and undermine in the reported performance difference.
Authors: We acknowledge that the current presentation of results lacks several key experimental details needed for full evaluation. The manuscript reports the 87.50% and 67.50% accuracies but does not specify the cross-validation procedure, statistical testing, imbalance handling, or feature ablations. In the revised version we will expand the Results and Methods sections to describe the cross-validation strategy, report statistical significance of the accuracy difference, clarify any class-imbalance mitigation steps, and include ablation experiments that separately evaluate radiomic features and geometric features derived from the deformation fields. revision: yes
Circularity Check
Empirical pipeline comparison with no derivational circularity
full rationale
The manuscript describes a modular pipeline (foundational-model segmentation, Atlas-ISTN registration, radiomic and geometric feature extraction, then downstream classifier) and reports an empirical accuracy comparison on the external public ASOCA dataset (87.50 % vs 67.50 % baseline). No equations, first-principles derivations, or predictions are presented that reduce by construction to fitted parameters, self-definitions, or self-citation chains. The central result is a head-to-head experiment whose numerical outcome is not forced by any internal redefinition or renaming of inputs; the pipeline steps remain independently verifiable against external benchmarks such as Dice scores or registration error metrics, even if those metrics are not reported in the provided text.
Axiom & Free-Parameter Ledger
axioms (2)
- domain assumption Foundational segmentation models produce accurate cardiac structure delineations on the ASOCA dataset.
- domain assumption Deformation fields obtained by registering patient scans to a normative healthy atlas encode geometric differences that are discriminative for CVD.
Lean theorems connected to this paper
-
IndisputableMonolith/Cost/FunctionalEquation.leanwashburn_uniqueness_aczel unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
We extract the following features ... First-order statistics ... Shape descriptors ... GLCM ... deformation field ... SVD
What do these tags mean?
- matches
- The paper's claim is directly supported by a theorem in the formal canon.
- supports
- The theorem supports part of the paper's argument, but the paper may add assumptions or extra steps.
- extends
- The paper goes beyond the formal theorem; the theorem is a base layer rather than the whole result.
- uses
- The paper appears to rely on the theorem as machinery.
- contradicts
- The paper's claim conflicts with a theorem or certificate in the canon.
- unclear
- Pith found a possible connection, but the passage is too broad, indirect, or ambiguous to say the theorem truly supports the claim.
Reference graph
Works this paper leans on
-
[1]
In: Proceedings of the 25th ACM SIGKDD international conference on knowledge discovery & data mining
Akiba, T., Sano, S., Yanase, T., Ohta, T., Koyama, M.: Optuna: A next- generation hyperparameter optimization framework. In: Proceedings of the 25th ACM SIGKDD international conference on knowledge discovery & data mining. pp. 2623–2631 (2019)
work page 2019
-
[2]
Alvén, J., Petersen, R., Hagerman, D., Sandstedt, M., Kitslaar, P., Bergström, G., Fagman, E., Hjelmgren, O.: Plaquevit: a vision transformer model for fully automatic vessel and plaque segmentation in coronary computed tomography an- giography. European Radiology pp. 1–11 (2025)
work page 2025
-
[3]
Frontiers in cardiovascular medicine9, 840262 (2022)
Amal, S., Safarnejad, L., Omiye, J.A., Ghanzouri, I., Cabot, J.H., Ross, E.G.: Use of multi-modal data and machine learning to improve cardiovascular disease care. Frontiers in cardiovascular medicine9, 840262 (2022)
work page 2022
-
[4]
European Heart Journal Open 2(2), oeac018 (2022)
Bray, J.J.H., Hanif, M.A., Alradhawi, M., Ibbetson, J., Dosanjh, S.S., Smith, S.L., Ahmad, M., Pimenta, D.: Machine learning applications in cardiac computed to- mography: a composite systematic review. European Heart Journal Open 2(2), oeac018 (2022)
work page 2022
-
[5]
Computers in biology and medicine142, 105191 (2022) 10 A
Bruns, S., Wolterink, J.M., van den Boogert, T.P., Runge, J.H., Bouma, B.J., Henriques, J.P., Baan, J., Viergever, M.A., Planken, R.N., Išgum, I.: Deep learning- based whole-heart segmentation in 4d contrast-enhanced cardiac ct. Computers in biology and medicine142, 105191 (2022) 10 A. Mittal, R. Mehta, O. Todd,P. Seeböck, G. Langs, B. Glocker
work page 2022
-
[6]
Çiçek, Ö., Abdulkadir, A., Lienkamp, S.S., Brox, T., Ronneberger, O.: 3d u-net: learning dense volumetric segmentation from sparse annotation. In: Medical Image ComputingandComputer-AssistedIntervention–MICCAI2016:19thInternational Conference, Athens, Greece, October 17-21, 2016, Proceedings, Part II 19. pp. 424–
work page 2016
-
[7]
arXiv preprint arXiv:2411.02372 (2024)
Dey, N., Billot, B., Wong, H.E., Wang, C.J., Ren, M., Grant, P.E., Dalca, A.V., Golland, P.: Learning general-purpose biomedical volume representations using randomized synthesis. arXiv preprint arXiv:2411.02372 (2024)
- [8]
-
[9]
Computerized Medical Imaging and Graphics 97, 102049 (2022)
Gharleghi, R., Adikari, D., Ellenberger, K., Ooi, S.Y., Ellis, C., Chen, C.M., Gao, R., He, Y., Hussain, R., Lee, C.Y., et al.: Automated segmentation of normal and diseased coronary arteries–the asoca challenge. Computerized Medical Imaging and Graphics 97, 102049 (2022)
work page 2022
-
[10]
Nature methods 18(2), 203–211 (2021)
Isensee, F., Jaeger, P.F., Kohl, S.A., Petersen, J., Maier-Hein, K.H.: nnu-net: a self-configuring method for deep learning-based biomedical image segmentation. Nature methods 18(2), 203–211 (2021)
work page 2021
-
[11]
The Lancet Digital Health4(4), e256–e265 (2022)
Lin, A., Manral, N., McElhinney, P., Killekar, A., Matsumoto, H., Kwiecinski, J., Pieszko, K., Razipour, A., Grodecki, K., Park, C., et al.: Deep learning-enabled coronary ct angiography for plaque and stenosis quantification and cardiac risk prediction: an international multicentre study. The Lancet Digital Health4(4), e256–e265 (2022)
work page 2022
-
[12]
Decoupled Weight Decay Regularization
Loshchilov, I., Hutter, F.: Decoupled weight decay regularization. arXiv preprint arXiv:1711.05101 (2017)
work page internal anchor Pith review Pith/arXiv arXiv 2017
-
[13]
Frontiers in cardiovascular medicine7, 1 (2020)
Martin-Isla, C., Campello, V.M., Izquierdo, C., Raisi-Estabragh, Z., Baeßler, B., Petersen, S.E., Lekadir, K.: Image-based cardiac diagnosis with machine learning: a review. Frontiers in cardiovascular medicine7, 1 (2020)
work page 2020
-
[14]
IEEE Transactions on Medical Imaging41(2), 360–373 (2021)
Mehta, R., Christinck, T., Nair, T., Bussy, A., Premasiri, S., Costantino, M., Chakravarthy, M.M., Arnold, D.L., Gal, Y., Arbel, T.: Propagating uncertainty across cascaded medical imaging tasks for improved deep learning inference. IEEE Transactions on Medical Imaging41(2), 360–373 (2021)
work page 2021
-
[15]
Scientific Reports15(1), 8472 (2025)
Park, D., Kwon, S.S., Song, Y., Kim, Y.A., Jeong, B., Lee, W., Park, E.A.: Deep learning based automatic quantification of aortic valve calcification on contrast enhanced coronary ct angiography. Scientific Reports15(1), 8472 (2025)
work page 2025
-
[16]
Sinclair, M., Schuh, A., Hahn, K., Petersen, K., Bai, Y., Batten, J., Schaap, M., Glocker, B.: Atlas-istn: joint segmentation, registration and atlas construction with image-and-spatialtransformernetworks.MedicalImageAnalysis 78,102383(2022)
work page 2022
-
[17]
Thanassoulis, G., Peloso, G.M., Pencina, M.J., Hoffmann, U., Fox, C.S., Cupples, L.A., Levy, D., D’Agostino, R.B., Hwang, S.J., O’Donnell, C.J.: A genetic risk score is associated with incident cardiovascular disease and coronary artery calcium: the framinghamheartstudy.Circulation:CardiovascularGenetics 5(1),113–121(2012)
work page 2012
-
[18]
Cancer research77(21), e104–e107 (2017)
Van Griethuysen, J.J., Fedorov, A., Parmar, C., Hosny, A., Aucoin, N., Narayan, V., Beets-Tan, R.G., Fillion-Robin, J.C., Pieper, S., Aerts, H.J.: Computational radiomics system to decode the radiographic phenotype. Cancer research77(21), e104–e107 (2017)
work page 2017
-
[19]
Wasserthal, J., Breit, H.C., Meyer, M.T., Pradella, M., Hinck, D., Sauter, A.W., Heye, T., Boll, D.T., Cyriac, J., Yang, S., et al.: Totalsegmentator: robust segmen- tation of 104 anatomic structures in ct images. Radiology: Artificial Intelligence 5(5), e230024 (2023) CVD classification with radiomic and geometric features 11
work page 2023
-
[20]
Wilkins, E., Wilson, L., Wickramasinghe, K., Bhatnagar, P., Leal, J., Luengo- Fernandez, R., Burns, R., Rayner, M., Townsend, N.: European cardiovascular disease statistics 2017 (2017)
work page 2017
-
[21]
In: Medical Imaging with Deep Learning (2024)
Wundram, A.M., Fischer, P., Wunderlich, S., Faber, H., Koch, L.M., Berens, P., Baumgartner, C.F.: Leveraging probabilistic segmentation models for improved glaucoma diagnosis: A clinical pipeline approach. In: Medical Imaging with Deep Learning (2024)
work page 2024
-
[22]
Medical image analysis 58, 101537 (2019)
Zhuang, X., Li, L., Payer, C., Štern, D., Urschler, M., Heinrich, M.P., Oster, J., Wang, C., Smedby, Ö., Bian, C., et al.: Evaluation of algorithms for multi-modality whole heart segmentation: an open-access grand challenge. Medical image analysis 58, 101537 (2019)
work page 2019
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.