A CUBS-Compatible Ultrasound Morphology and Uncertainty-Aware Baseline for Carotid Intima-Media Segmentation and Preliminary Risk Prediction
Pith reviewed 2026-06-30 21:40 UTC · model grok-4.3
The pith
A neural network segments carotid intima-media from ultrasound at Dice 0.79 and predicts preliminary risk at AUC 0.69 using morphology alone.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
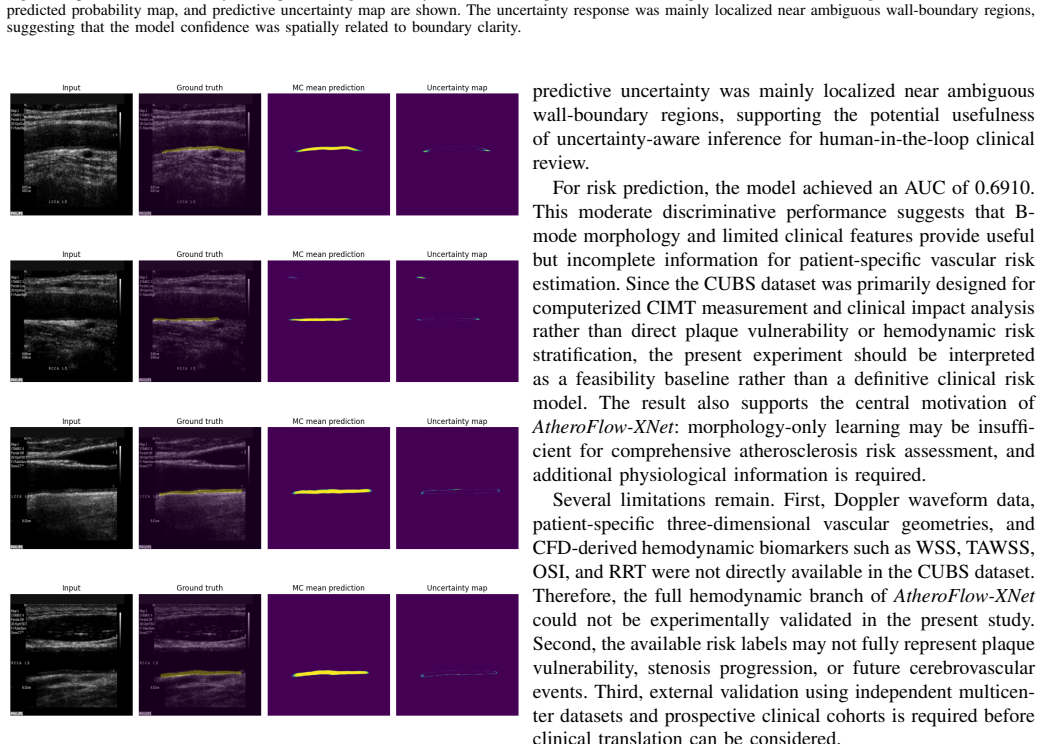
Converting manual boundary annotations into dense intima-media masks on the CUBS ultrasound dataset enables a segmentation model to achieve a Dice coefficient of 0.7930 and segmentation loss of 0.2359, while an auxiliary risk-prediction branch that incorporates clinical variables reaches an AUC of 0.6910; Monte Carlo dropout generates uncertainty maps that flag ambiguous wall-boundary regions, establishing a morphology-driven baseline for automated carotid analysis in the absence of flow data.
What carries the argument
AtheroFlow-XNet, a segmentation network with an auxiliary risk-prediction branch and Monte Carlo dropout for uncertainty-aware inference on dense intima-media masks derived from boundary annotations.
If this is right
- A Dice coefficient of 0.7930 indicates the model can automate identification of the carotid intima-media region from standard B-mode ultrasound.
- An AUC of 0.6910 shows that combining segmented morphology with clinical variables supports preliminary patient-level risk prediction.
- Uncertainty maps from Monte Carlo dropout can highlight regions where wall boundaries are ambiguous for human review.
- The absence of Doppler data means the results define a morphology-only baseline that future models can improve by adding flow profiles or wall-shear biomarkers.
Where Pith is reading between the lines
- Adding Doppler-derived peak systolic velocity or flow profiles to the auxiliary branch could raise the risk-prediction AUC by supplying hemodynamic context missing from the current morphology-only setup.
- Evaluating the model on datasets acquired with different ultrasound machines would test whether the reported Dice score holds under changes in image quality and resolution.
- Linking the uncertainty maps directly to clinical decision thresholds, such as whether to recommend further imaging, would turn the current qualitative observation into a quantifiable triage tool.
Load-bearing premise
The assumption that converting manual lumen-intima and media-adventitia boundary annotations into dense intima-media masks on the CUBS dataset produces reliable supervised training targets that generalize to patient-level risk prediction without Doppler or hemodynamic data.
What would settle it
An independent test on a new multi-center ultrasound cohort where intima-media masks are re-annotated by multiple experts and risk labels come from documented stroke or TIA events over five years; if the Dice coefficient falls below 0.70 or the AUC falls below 0.60, the claim of reliable morphology-based segmentation and risk prediction would be falsified.
Figures

read the original abstract
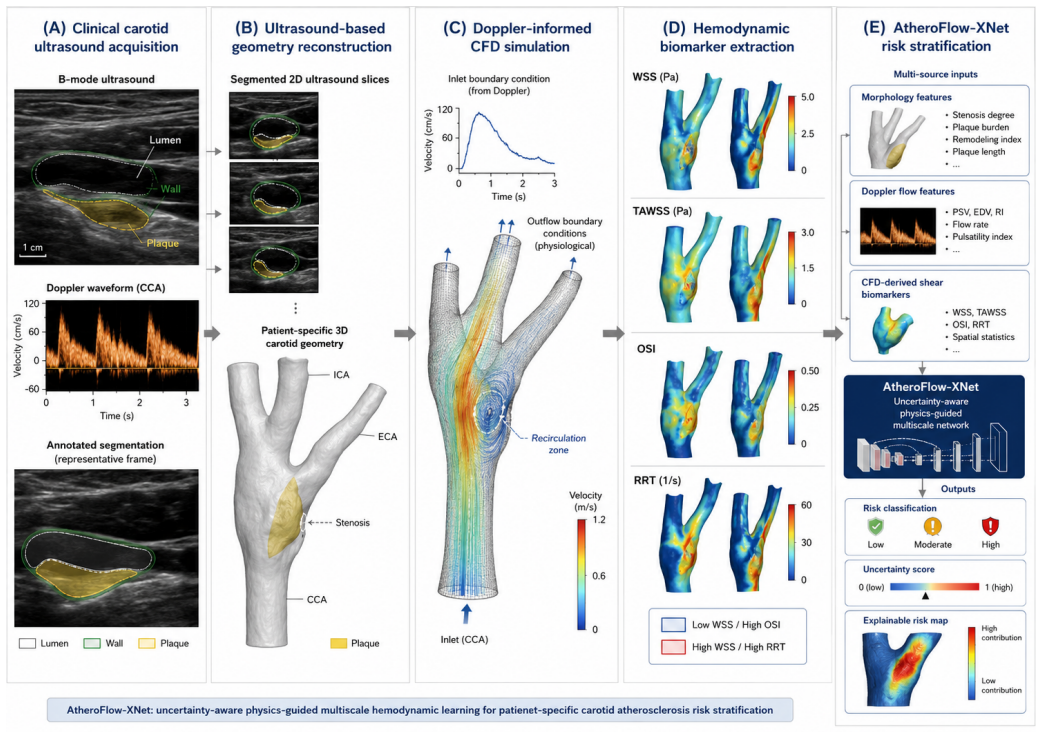
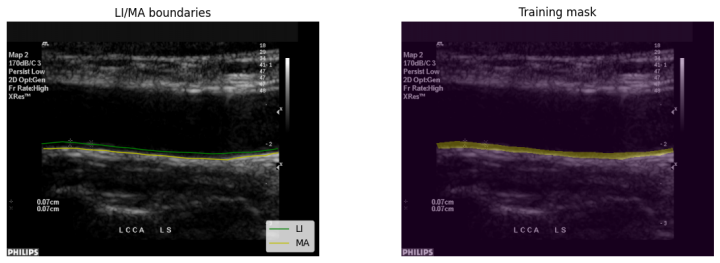
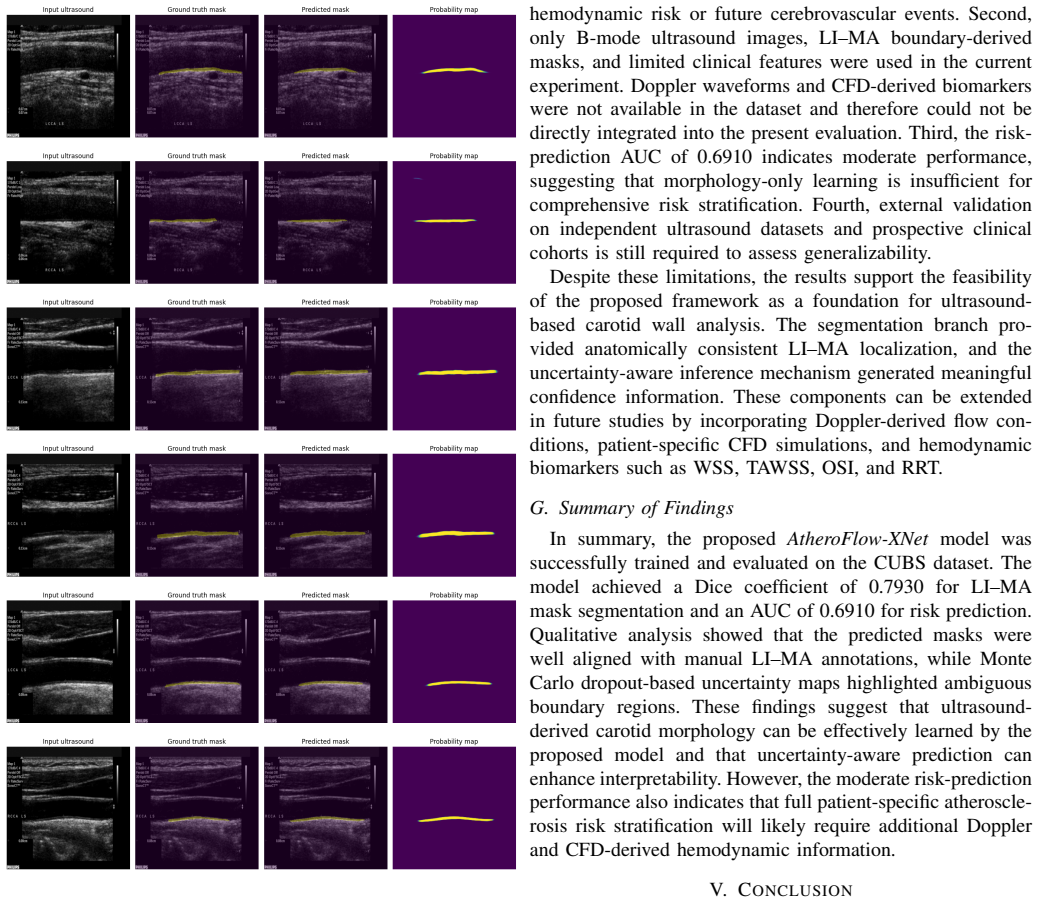
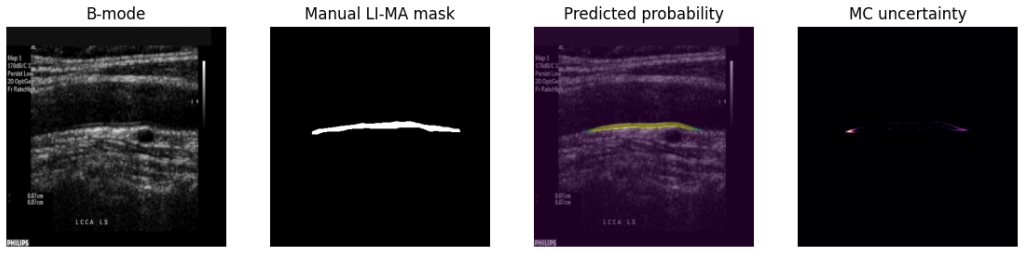
Carotid atherosclerosis is a major contributor to ischemic stroke and transient ischemic attack. Conventional ultrasound assessment is commonly based on intima-media thickness, plaque appearance, stenosis degree, and peak systolic velocity, but these morphology- and velocity-based indicators may not fully capture patient-specific vascular risk. This study presents AtheroFlow-XNet, a CUBS-compatible ultrasound morphology and uncertainty-aware learning baseline for carotid intima-media segmentation and preliminary risk prediction. Using the Carotid Ultrasound Boundary Study dataset, manual lumen-intima and media-adventitia boundary annotations were converted into dense intima-media masks for supervised segmentation. Clinical variables were incorporated into an auxiliary risk-prediction branch, and Monte Carlo dropout was used for uncertainty-aware inference. The model was evaluated using a patient-level train-validation-test split with 1,522 training images, 326 validation images, and 328 testing images. The proposed model achieved a Dice coefficient of 0.7930 for LI-MA mask segmentation, a segmentation loss of 0.2359, and an area under the receiver operating characteristic curve of 0.6910 for preliminary risk prediction. Qualitative results showed that predicted masks were generally aligned with manual annotations, while uncertainty maps highlighted ambiguous wall-boundary regions. These results suggest that ultrasound-derived carotid morphology can support automated wall analysis and uncertainty-aware interpretation. Since CUBS does not provide Doppler waveforms or CFD-derived hemodynamic biomarkers, this work should be interpreted as a reproducible morphology-driven baseline. Future work will incorporate Doppler-derived flow profiles, patient-specific vascular reconstruction, and CFD-based wall shear biomarkers.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript introduces AtheroFlow-XNet as a CUBS-compatible baseline for carotid intima-media segmentation and preliminary risk prediction. Boundary annotations are converted to dense LI-MA masks for supervised training; an auxiliary branch incorporates clinical variables, and Monte Carlo dropout enables uncertainty-aware inference. On a patient-level split (1,522 train / 326 val / 328 test images), the model reports Dice 0.7930, segmentation loss 0.2359, and AUC 0.6910, explicitly framed as a morphology-only baseline given the absence of Doppler or hemodynamic data.
Significance. If the metrics hold, the work supplies a concrete, reproducible morphology-driven baseline on the CUBS dataset together with uncertainty maps, which can serve as a reference point for future carotid ultrasound studies that add flow or CFD features. The modest AUC underscores the limited standalone predictive value of morphology alone.
major comments (3)
- [Evaluation] Evaluation section: no baseline comparisons (e.g., standard U-Net, IMT measurement pipelines, or prior CUBS segmentation results) are provided for the Dice coefficient of 0.7930 or the AUC of 0.6910, which undermines the claim that the reported numbers constitute a useful baseline.
- [Risk Prediction Branch] Risk-prediction branch: the AUC 0.6910 is obtained from an auxiliary branch trained on the identical patient split used for segmentation; without external validation, held-out clinical cohorts, or details on how the branch weighting interacts with the segmentation loss, the preliminary risk-prediction result lacks support for generalizability.
- [Methods and Results] Methods and results: no error bars, confidence intervals, or statistical significance tests accompany the reported metrics, and no ablation is shown on the auxiliary-branch weighting or MC-dropout rate (both listed as free parameters), leaving the contribution of each component unquantified.
minor comments (2)
- [Abstract] Abstract: the patient split sizes are stated in the body but could be repeated in the abstract for immediate clarity.
- [Methods] Notation: the conversion of boundary annotations to dense masks is described but would benefit from an explicit equation or pseudocode showing how the intima-media region is filled.
Simulated Author's Rebuttal
We thank the referee for the constructive comments. Our work is explicitly positioned as a reproducible morphology-only baseline on the CUBS dataset using a patient-level split, and we address each major point below with plans for revision where feasible.
read point-by-point responses
-
Referee: [Evaluation] Evaluation section: no baseline comparisons (e.g., standard U-Net, IMT measurement pipelines, or prior CUBS segmentation results) are provided for the Dice coefficient of 0.7930 or the AUC of 0.6910, which undermines the claim that the reported numbers constitute a useful baseline.
Authors: We agree that comparisons would strengthen the baseline utility. No prior CUBS results exist on this exact patient-level split and dense LI-MA mask task. In revision we will add a standard U-Net comparison under identical conditions to contextualize the Dice score; the AUC remains framed as preliminary morphology-only without optimality claims. revision: partial
-
Referee: [Risk Prediction Branch] Risk-prediction branch: the AUC 0.6910 is obtained from an auxiliary branch trained on the identical patient split used for segmentation; without external validation, held-out clinical cohorts, or details on how the branch weighting interacts with the segmentation loss, the preliminary risk-prediction result lacks support for generalizability.
Authors: We concur that the shared split limits generalizability claims and will expand the methods to detail the auxiliary branch weighting and its interaction with segmentation loss. External validation is unavailable within this CUBS-only study; we will reinforce the preliminary framing in the discussion. revision: partial
-
Referee: [Methods and Results] Methods and results: no error bars, confidence intervals, or statistical significance tests accompany the reported metrics, and no ablation is shown on the auxiliary-branch weighting or MC-dropout rate (both listed as free parameters), leaving the contribution of each component unquantified.
Authors: The absence of these elements is a valid observation. We will add error bars from repeated runs with varied seeds and include ablations on branch weighting and MC-dropout rate in the revised results to quantify component contributions. revision: yes
- Absence of external validation cohorts to support generalizability of the risk-prediction AUC, as the study uses only the CUBS dataset.
Circularity Check
No significant circularity in claimed results
full rationale
The paper reports standard supervised ML metrics (Dice, loss, AUC) on a patient-level held-out test split after converting boundary annotations to masks and adding an auxiliary clinical branch. No mathematical derivation chain, first-principles claims, or predictions that reduce to inputs by construction are present. The work is explicitly framed as a preliminary empirical baseline without Doppler data, with no load-bearing self-citations or ansatzes invoked. This is a normal non-circular empirical report.
Axiom & Free-Parameter Ledger
free parameters (2)
- Monte Carlo dropout rate
- Auxiliary branch weighting
axioms (2)
- domain assumption Manual boundary annotations can be reliably converted to dense segmentation masks without introducing systematic label noise.
- domain assumption Patient-level split prevents leakage and supports generalization to new patients.
Reference graph
Works this paper leans on
-
[1]
Meiburger, Kristen M.; Zahnd, Guillaume; Faita, Francesco; Loizou, Christos; Carvalho, Catarina; Steinman, David; Gibello, Lorenzo; Bruno, Rosa Maria; Marzola, Francesco; Clarenbach, Ricarda; Francesconi, Martina; Nicolaides, Andrew; Campilho, Aurelio; Ghotbi, Reza; Kyr- iacou, Efthyvoulos ; Navab, Nassir; Griffin, Maura; Panayiotou, Andrie; Gherardini, R...
-
[2]
Meiburger, Guillaume Zahnd, Francesco Faita, Christos P
Kristen M. Meiburger, Guillaume Zahnd, Francesco Faita, Christos P. Loizou, Catarina Carvalho, David A. Steinman, Lorenzo Gibello, Rosa Maria Bruno, Francesco Marzola, Ricarda Clarenbach, Mar- tina Francesconi, Andrew N. Nicolaides, Aurelio Campilho, Reza Ghotbi, Efthyvoulos Kyriacou, Nassir Navab, Maura Griffin, Andrie G. Panayiotou, Rachele Gherardini, ...
-
[3]
Piek, L., Gillissen, M., de Ruijter, J., van Sambeek, M., & Lopata, R. (2026). Ultrasound-based computational fluid dynamics analysis of carotid artery hemodynamics in healthy and stenosed conditions. Computer Methods in Biomechanics and Biomedical Engineering, 1–11. https://doi.org/10.1080/10255842.2026.2617934
-
[4]
LaDisa JF Jr, Bowers M, Harmann L, Prost R, Doppalapudi A V , Mohyuddin T, Zaidat O, Migrino RQ. Time-efficient patient-specific quantification of regional carotid artery fluid dynamics and spatial correlation with plaque burden. Med Phys. 2010 Feb;37(2):784-92. doi: 10.1118/1.3292631. PMID: 20229888; PMCID: PMC2826384
-
[5]
Strecker C, Krafft AJ, Kaufhold L, H ¨ullebrandt M, Treppner M, Ludwig U, K ¨ober G, Hennemuth A, Hennig J and Harloff A (2021) Carotid Geometry and Wall Shear Stress Independently Predict Increased Wall Thickness—A Longitudinal 3D MRI Study in High-Risk Patients. Front. Cardiovasc. Med. 8:723860. doi: 10.3389/fcvm.2021.723860
-
[6]
Xu, P., Liu, X., Zhang, H. et al. Assessment of boundary conditions for CFD simulation in human carotid artery. Biomech Model Mechanobiol 17, 1581–1597 (2018). https://doi.org/10.1007/s10237-018-1045-4
-
[7]
Kizhisseri, M., Gharaie, S. & Schluter, J. An analytical method informed by clinical imaging data for estimating outlet boundary conditions in computational fluid dynamics analysis of carotid artery blood flow. Sci Rep 13, 14973 (2023). https://doi.org/10.1038/s41598-023-42004-5
-
[8]
Du J, Wu G, Wu B, Liu C, Mai Z, Liu Y , Wang Y , Zhang P, Wu G, Liu J. The Hemodynamic Effect of Enhanced External Counterpulsation Treat- ment on Atherosclerotic Plaque in the Carotid Artery: A Framework of Patient-Specific Computational Fluid Dynamics Analysis. Cardiol Res Pract. 2020 Apr 30;2020:5903790. doi: 10.1155/2020/5903790. PMID: 32411447; PMCID...
-
[9]
Li Z, Luo A, Liu X, Xie S, Wang Y , Deng L, Zhong S, Liu Y , Cao X, Du Y , Luo W, Deng Y and Yin L (2024) Study on the characteristics of carotid wall shear stress in type 2 diabetes patients based on ultrasound vector flow imaging. Front. Endocrinol. 15:1409082. doi: 10.3389/fendo.2024.1409082
-
[10]
Hong S, Dong Y , Gao W, Song D, Liu M, Li W, Du Y , Xu J, Dong F. Evaluation of Carotid Stenosis in a High-Stroke-Risk Population by Hemodynamic Dual-Parameters Based on Ultrasound Vector Flow Imag- ing. Brain Behav. 2024 Nov;14(11):e70150. doi: 10.1002/brb3.70150. PMID: 39552116; PMCID: PMC11570680
-
[11]
(https://www.sciencedirect.com/science/article/pii/S0741521424013417)
Xiang Zhang, Huanhuan Ding, Xiaoli Ji, Ling Chen, Peipei Huang, Zengqiao Lin, Jianbi Zhu, Shujing Zhou, Zezheng Liu, Miaomiao Zhang, Qi Xu, Predicting vulnerable carotid plaques by detecting wall shear stress based on ultrasonic vector flow imaging, Jour- nal of Vascular Surgery, V olume 80, Issue 5, 2024, Pages 1475- 1486.e1, ISSN 0741-5214, https://doi....
-
[12]
Goudot, G., Sitruk, J., Jimenez, A. et al. Carotid Plaque Vulnerabil- ity Assessed by Combined Shear Wave Elastography and Ultrafast Doppler Compared to Histology. Transl. Stroke Res. 13, 100–111 (2022). https://doi.org/10.1007/s12975-021-00920-6
-
[13]
He L, Cai Y , Feng Y , Feng T, Cademartiri F, Shen E. Age-related wall shear stress changes assessed by vascular vector flow mapping in the carotid arteries of healthy adults: a cross-sectional study. Cardiovasc Diagn Ther. 2024 Aug 31;14(4):668-678. doi: 10.21037/cdt-24-134. Epub 2024 Aug 16. PMID: 39263489; PMCID: PMC11384466
-
[14]
Syamul Bashar, Rifat Hossain, Md
Md. Syamul Bashar, Rifat Hossain, Md. Habibur Rahman, Utsha Roy, Md. Shafiqul Islam, CFD analysis of non-Newtonian blood flow through human carotid artery bifurcation: Carotid sinus susceptible to atherosclerosis, Heliyon, V olume 10, Issue 22, 2024, e40286, ISSN 2405-8440, https://doi.org/10.1016/j.heliyon.2024.e40286. (https://www.sciencedirect.com/scie...
-
[15]
Chen A, Chen Z, Su J, Pen J, Luo T and Zhong H (2025) The effects of carotid plaque classification and bifurcation angle on plaque: a computational fluid dynamics simulation. Front. Physiol. 16:1509875. doi: 10.3389/fphys.2025.1509875
-
[16]
Liu C, Wu G, Xu J, Xiao Q and Wang H (2023) Numerical investigation of the effect of carotid bifurcation stenosis degree on pulsatility charac- teristics. Front. Physiol. 14:1169198. doi: 10.3389/fphys.2023.1169198
-
[17]
Cite this article Li, X., Sun, B., Zhao, H. et al. Retrospective Study of Hemodynamic Changes Before and After Carotid Stenosis Formation by Vessel Surface Repairing. Sci Rep 8, 5493 (2018). https://doi.org/10.1038/s41598-018-23842-0
-
[18]
Yang, J., Zhang, Y ., Xue, J. et al. Hemodynamic effects of steno- sis with varying severity in different segments of the carotid artery using computational fluid dynamics. Sci Rep 15, 4896 (2025). https://doi.org/10.1038/s41598-025-89100-2
-
[19]
Moerman AM, Korteland S, Dilba K, van Gaalen K, Poot DHJ, van Der Lugt A, Verhagen HJM, Wentzel JJ, van Der Steen AFW, Gijsen FJH and Van der Heiden K (2022) The Correlation Between Wall Shear Stress and Plaque Composition in Advanced Human Carotid Atherosclerosis. Front. Bioeng. Biotechnol. 9:828577. doi: 10.3389/fbioe.2021.828577
-
[20]
Dilba K, van Dam-Nolen DHK, Korteland S-A, van der Kolk AG, Kassem M, Bos D, Koudstaal PJ, Nederkoorn PJ, Hendrikse J, Kooi ME, Gijsen FJH, van der Steen AFW, van der Lugt A and Wentzel JJ (2021) The Association Between Time-Varying Wall Shear Stress and the Development of Plaque Ulcerations in Carotid Arteries From the Plaque at Risk Study. Front. Cardio...
-
[21]
Hybrid CFD PINN FSI Simulation in Coronary Artery Trees
Alzhanov N, Ng EYK, Zhao Y . Hybrid CFD PINN FSI Simulation in Coronary Artery Trees. Fluids. 2024; 9(12):280. https://doi.org/10.3390/fluids9120280
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.