Do Clinical Models Change Treatment Decisions?
Pith reviewed 2026-06-29 12:03 UTC · model grok-4.3
The pith
Strong medical QA performance does not reliably predict whether models change treatment decisions when patient context changes.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
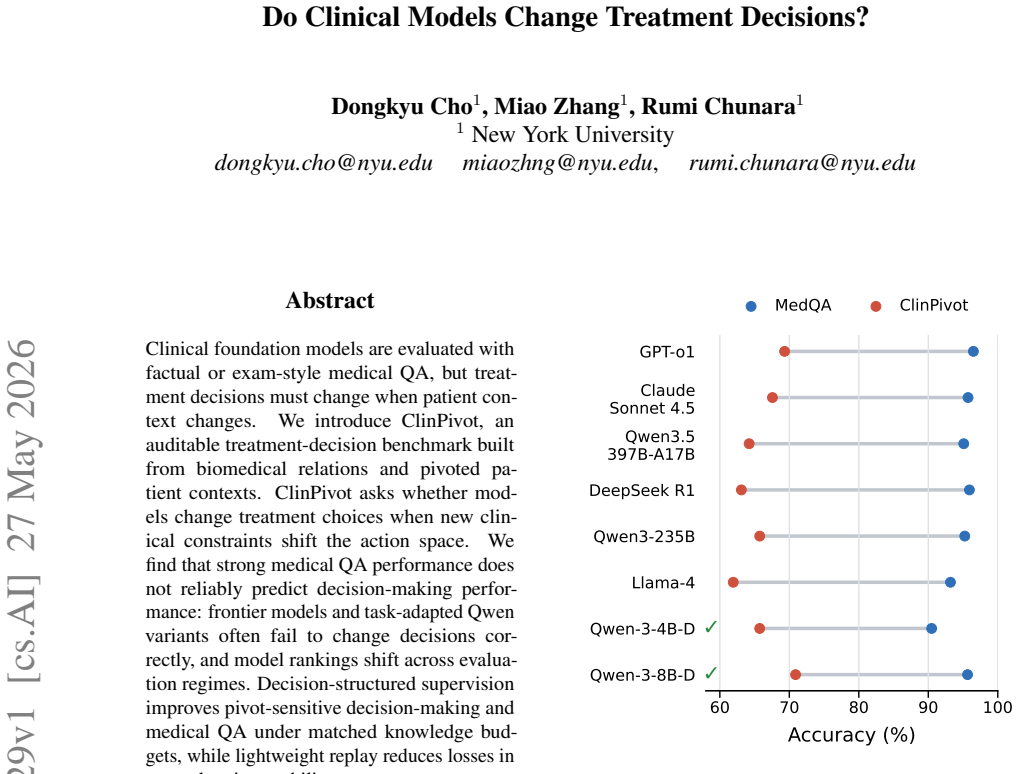
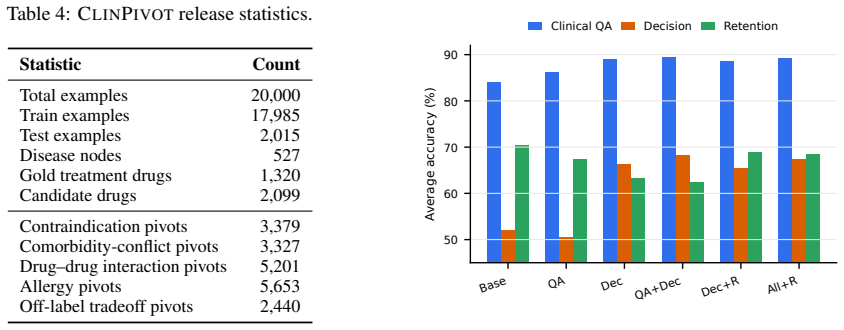
Strong performance on medical QA benchmarks does not reliably predict decision-making performance on treatment choices that must change with new clinical constraints. Frontier models and task-adapted Qwen variants often fail to change decisions correctly in response to pivoted patient contexts, and model rankings shift across evaluation regimes. Decision-structured supervision improves pivot-sensitive decision-making and medical QA under matched knowledge budgets, while lightweight replay reduces losses in general assistant ability.
What carries the argument
ClinPivot, an auditable benchmark that constructs pivoted patient contexts from biomedical relations to test whether models change treatment choices when the action space shifts.
If this is right
- Models that excel at medical QA may still fail to adjust treatments when patient constraints change.
- Model rankings on decision-making tasks differ from those on standard QA evaluations.
- Decision-structured supervision during training improves both adaptive decision-making and QA performance.
- Lightweight replay during specialized training can preserve general assistant abilities.
Where Pith is reading between the lines
- Evaluation of clinical AI should incorporate explicit tests of context-driven adaptation rather than relying solely on QA accuracy.
- Training approaches that emphasize decision pivots may transfer to other adaptive reasoning tasks outside medicine.
- Benchmarks like ClinPivot could be extended to measure correlation with actual clinical outcomes in prospective studies.
Load-bearing premise
The pivoted patient contexts constructed in ClinPivot from biomedical relations accurately represent real clinical scenarios in which treatment decisions should change.
What would settle it
A controlled study in which expert clinicians review model outputs on real patient cases with documented context shifts and find that models failing ClinPivot still make the correct treatment changes would falsify the central claim.
Figures

read the original abstract
Clinical foundation models are evaluated with factual or exam-style medical QA, but treatment decisions must change when patient context changes. We introduce ClinPivot, an auditable treatment-decision benchmark built from biomedical relations and pivoted patient contexts. ClinPivot asks whether models change treatment choices when new clinical constraints shift the action space. We find that strong medical QA performance does not reliably predict decision-making performance: frontier models and task-adapted Qwen variants often fail to change decisions correctly, and model rankings shift across evaluation regimes. Decision-structured supervision improves pivot-sensitive decision-making and medical QA under matched knowledge budgets, while lightweight replay reduces losses in general assistant ability.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper introduces ClinPivot, an auditable benchmark constructed from biomedical relations and pivoted patient contexts, to test whether clinical models appropriately alter treatment decisions when new constraints shift the action space. It claims that strong medical QA performance does not reliably predict decision-making performance, that frontier models and task-adapted Qwen variants frequently fail to change decisions correctly, that model rankings shift across evaluation regimes, and that decision-structured supervision improves pivot-sensitive decision-making while preserving general capabilities under matched knowledge budgets.
Significance. If the benchmark construction is shown to produce valid instances of treatment change, the result would demonstrate a meaningful gap between standard medical QA evaluations and clinical decision-making requirements, with implications for how clinical foundation models are assessed and trained. The use of relation-based pivots for an auditable benchmark is a constructive methodological contribution.
major comments (2)
- [ClinPivot benchmark construction] ClinPivot benchmark construction (abstract and methods): the central claim that QA performance fails to predict decision-making performance rests on the assumption that pivoted contexts constitute realistic scenarios where treatment should change due to clinical constraints; however, the construction extracts relations and applies pivots without described independent validation against expert judgment or real patient trajectories, raising the risk that observed failures and ranking shifts are artifacts of synthetic benchmark design rather than generalizable findings.
- [Evaluation and results] Evaluation and results sections: the reported shifts in model rankings across QA and decision-making regimes, and the claim that decision-structured supervision improves performance, require explicit details on sample sizes, statistical tests for ranking changes, error analysis, and controls for knowledge overlap between QA and pivot tasks to establish that the disconnect is not driven by mismatched difficulty or data leakage.
minor comments (2)
- [Abstract] The abstract states findings on frontier models and Qwen variants but does not specify the exact models, number of pivots, or decision categories evaluated; adding these details would improve clarity.
- [Introduction] Notation for 'pivoted patient contexts' and 'action space' shifts could be defined more explicitly on first use to aid readers unfamiliar with the benchmark.
Simulated Author's Rebuttal
We thank the referee for the detailed and constructive report. We address the two major comments point-by-point below. We agree that both points require additional detail and will revise the manuscript accordingly.
read point-by-point responses
-
Referee: [ClinPivot benchmark construction] ClinPivot benchmark construction (abstract and methods): the central claim that QA performance fails to predict decision-making performance rests on the assumption that pivoted contexts constitute realistic scenarios where treatment should change due to clinical constraints; however, the construction extracts relations and applies pivots without described independent validation against expert judgment or real patient trajectories, raising the risk that observed failures and ranking shifts are artifacts of synthetic benchmark design rather than generalizable findings.
Authors: The benchmark is deliberately synthetic and constructed from publicly verifiable biomedical relations (e.g., drug-disease, contraindication triples drawn from established KBs) so that every pivot instance remains fully auditable. We acknowledge that the current manuscript does not describe an independent expert validation step. In revision we will add (i) an explicit description of the pivot-generation algorithm, (ii) the criteria used to select clinically meaningful constraints, and (iii) results of a small-scale expert review (n=50 instances) confirming that the pivoted contexts are plausible and that the expected treatment change is clinically justified. This will be reported without claiming equivalence to real patient trajectories. revision: yes
-
Referee: [Evaluation and results] Evaluation and results sections: the reported shifts in model rankings across QA and decision-making regimes, and the claim that decision-structured supervision improves performance, require explicit details on sample sizes, statistical tests for ranking changes, error analysis, and controls for knowledge overlap between QA and pivot tasks to establish that the disconnect is not driven by mismatched difficulty or data leakage.
Authors: We agree that these details are necessary. The revised manuscript will report: exact sample sizes per regime, Spearman rank correlation and paired statistical tests (McNemar / Wilcoxon) for ranking shifts, a categorized error analysis of failure modes, and explicit controls showing that QA and pivot tasks use disjoint relation sets with no entity overlap. These additions will be placed in the Evaluation and Results sections and will be accompanied by the corresponding numbers and p-values. revision: yes
Circularity Check
No circularity: benchmark construction and evaluation are independent of tested models
full rationale
The paper constructs ClinPivot from external biomedical relations and pivoted contexts, then empirically evaluates frontier and adapted models on decision-change tasks versus QA. No equations or steps reduce by construction to fitted inputs, self-definitions, or self-citation chains; the benchmark is presented as an external test set whose validity is separate from model outputs. Central findings (ranking shifts, failure to change decisions) are reported as observed results rather than tautologies. This matches the default case of a self-contained empirical study with no load-bearing circular reductions.
Axiom & Free-Parameter Ledger
invented entities (1)
-
ClinPivot benchmark
no independent evidence
Reference graph
Works this paper leans on
-
[1]
Forget forgetting: Continual learning in a world of abundant memory, 2026
Building a knowledge graph to enable pre- cision medicine.Scientific Data, 10(1):67. Dongkyu Cho, Taesup Moon, Rumi Chunara, Kyunghyun Cho, and Sungmin Cha. 2026a. Forget forgetting: Continual learning in a world of abundant memory.Preprint, arXiv:2502.07274. Dongkyu Cho, Amy B. Z. Zhang, Bilel Fehri, Sheng Wang, Rumi Chunara, Hengrui Cai, and Rui Song. 2...
-
[2]
Towards Generalist Biomedical AI,
Towards generalist biomedical ai.Preprint, arXiv:2307.14334. Hang Wu, Wenqi Shi, Anirudh Choudhary, and May D Wang. 2024a. Clinical decision making under un- certainty: a bootstrapped counterfactual inference approach.BMC Medical Informatics and Decision Making, 24(1):275. Tongtong Wu, Linhao Luo, Yuan-Fang Li, Shirui Pan, Thuy-Trang Vu, and Gholamreza Ha...
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.