A New Angle on Bones: Robust Pose Estimation in X-Ray and Ultrasound
Pith reviewed 2026-06-28 07:20 UTC · model grok-4.3
The pith
A learning-based point proposal step followed by robust line fitting estimates bone angles in X-rays and ultrasound to within clinical observer error.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
By generating point candidates with a learned model and then recovering bone axes through robust line estimation rather than least-squares or direct landmark regression, the pipeline produces angular measurements whose average errors on the three clinical tasks remain inside the range of human observer disagreement while exceeding the accuracy of landmark-only alternatives.
What carries the argument
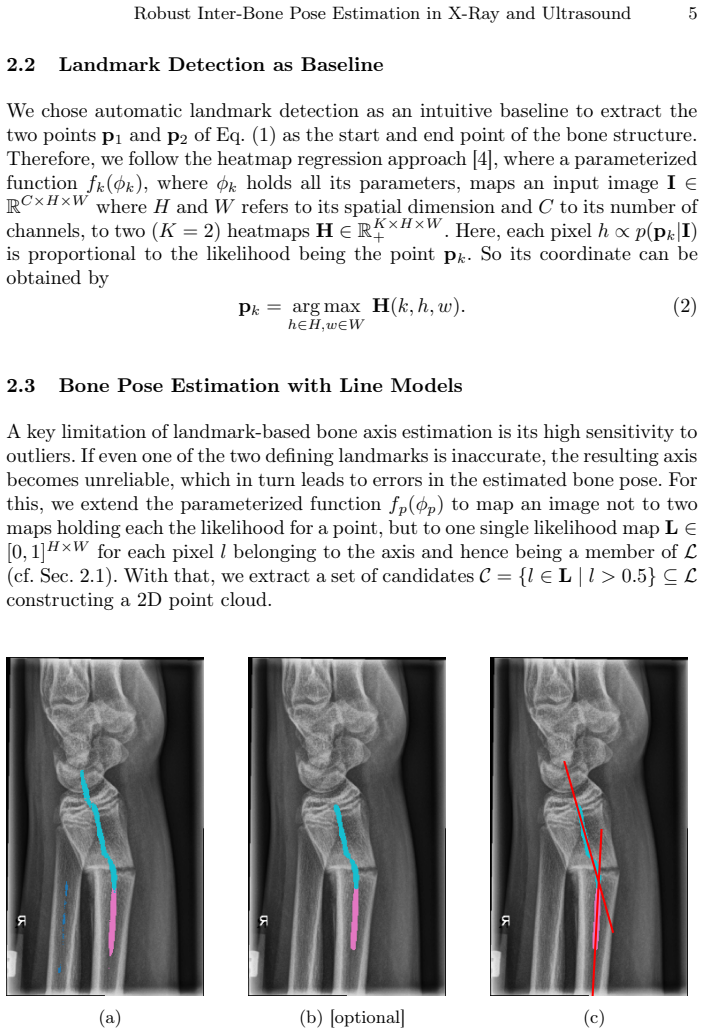
learning-based point candidate proposal followed by robust line fitting (RANSAC or Hough transform) to extract axis parameters
If this is right
- Angle measurements for fracture assessment and hip dysplasia screening can be obtained without manual landmark annotation on each new image.
- Reproducibility of paediatric orthopaedic metrics improves because the pipeline replaces variable human landmark placement with a fixed algorithmic procedure.
- The same two-stage design (point proposal then robust axis fit) can be retrained for additional bone structures once suitable annotated data exist.
- Clinical workflow time for quantitative angle reporting decreases because the pipeline runs end-to-end from image to numeric angle.
- Outlier rejection steps inside the line-fitting stage protect accuracy even when the point-proposal network produces occasional false positives.
Where Pith is reading between the lines
- The approach could be extended to three-dimensional volumetric data if the point-proposal network is replaced by a 3-D analogue and the line model becomes a plane or cylinder fit.
- Real-time use during ultrasound-guided procedures becomes feasible once the network is quantized and the fitting step is optimized for low latency.
- Systematic comparison against other robust estimators such as M-estimators or graph-cut methods would clarify whether RANSAC and Hough are the only viable choices for this domain.
- If the point-proposal network is trained on a broader mix of scanners and patient ages, the same pipeline might maintain accuracy across adult as well as paediatric populations.
Load-bearing premise
The learned point proposals supply enough inliers that robust fitting recovers the true bone axes without systematic offset from false positives or image artifacts.
What would settle it
On a held-out set of the same three tasks, if the method's angular errors rise above published clinical observer variability ranges or display consistent directional bias on images containing common artifacts, the central performance claim would be refuted.
Figures
read the original abstract
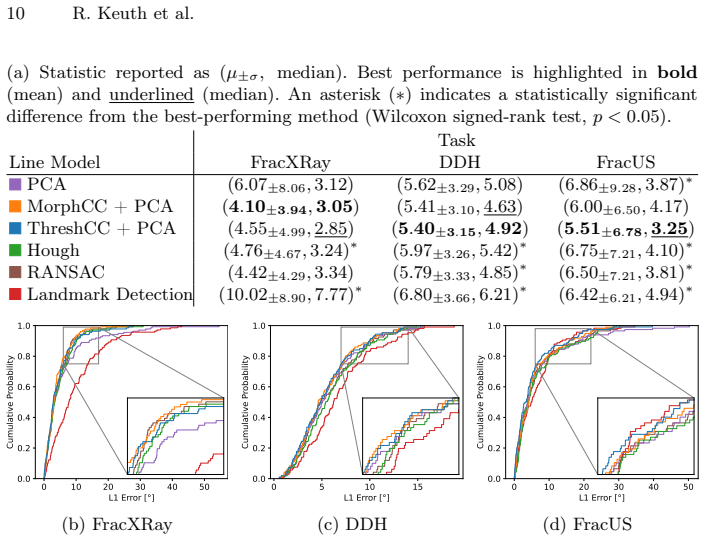
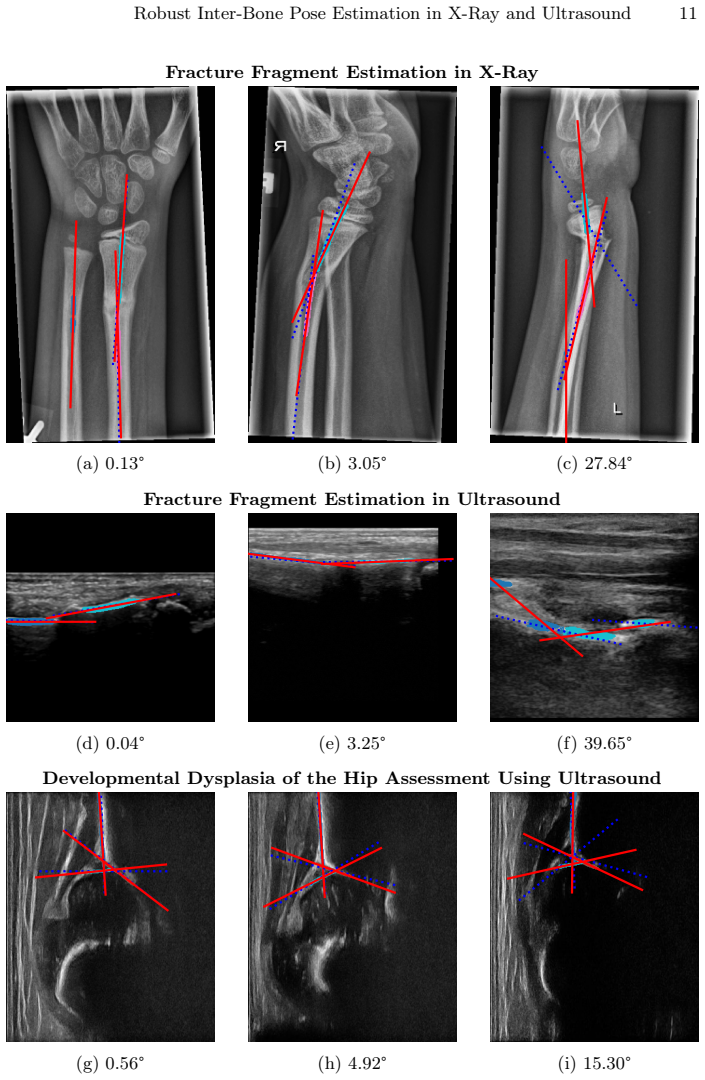
Measuring the angle between bone structures is a routine task in medical image analysis and provides a key quantitative parameter for diagnosis and treatment planning. Automated methods can reduce time and cost while improving reproducibility. In this work, we address automatic bone pose estimation using a learning-based point candidate proposal followed by a line model to extract axis parameters. Since conventional line models such as least squares are sensitive to outliers, we incorporate false-positive reduction strategies and robust fitting techniques, such as RANSAC and Hough transforms, to improve robustness. We evaluate our method on three clinically relevant paediatric angle estimation tasks: fracture fragment assessment in radiographs and ultrasound and developmental dysplasia of the hip evaluation in ultrasound using the Graf method. Our approach achieves mean errors of $4.1^\circ$, $5.4^\circ$, and $5.51^\circ$, respectively, not only remaining within the expected clinical observer variability, but also significantly outperforming landmark-based methods. Our code and annotations for fracture angle assessment in radiographs are publicly available on GitHub.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper proposes a two-stage approach for automatic bone axis and angle estimation in radiographs and ultrasound: a learning-based network proposes point candidates on bone structures, followed by robust line fitting (RANSAC or Hough) with false-positive reduction to recover axes. It reports evaluation on three paediatric tasks (fracture fragment assessment in X-ray, fracture assessment in ultrasound, and Graf-method DDH assessment in ultrasound), with mean angular errors of 4.1°, 5.4°, and 5.51° that are claimed to lie within clinical observer variability and to significantly outperform landmark-based baselines. Code and annotations for one task are released publicly.
Significance. If the performance claims are substantiated with proper statistical reporting and component ablations, the work would offer a practical, modality-robust tool for a routine clinical measurement task, potentially improving reproducibility in paediatric orthopaedics. The public release of code and annotations is a clear strength that supports reproducibility.
major comments (3)
- [Abstract] Abstract: the headline mean errors (4.1°, 5.4°, 5.51°) and the claim of statistically significant outperformance are presented without standard deviations, dataset sizes (train/test splits), number of images or patients, or any statistical test results. This directly weakens the assertion that the method remains within clinical observer variability and outperforms landmarks.
- [Abstract] Abstract / method description: the paper states that false-positive reduction strategies are incorporated, yet supplies no quantitative characterization of the proposal network (inlier ratio, precision, false-positive rate) on the test sets, nor any ablation that isolates the contribution of the robust fitting stage versus the network alone. Because the three tasks involve distinct artifact profiles, this leaves the central robustness claim untested.
- [Abstract] Abstract: no details are given on how the false-positive reduction was implemented or tuned, nor on whether the same hyper-parameters were used across the radiograph and ultrasound tasks. This information is load-bearing for the claim that the pipeline generalizes without systematic bias from network errors.
minor comments (1)
- [Abstract] The abstract mentions three tasks but does not name the exact clinical angles measured in each (e.g., which Graf angles or fracture angles); adding one sentence would improve clarity.
Simulated Author's Rebuttal
We thank the referee for the constructive comments, which identify opportunities to strengthen the abstract's support for our claims. We address each point below and will revise the abstract accordingly.
read point-by-point responses
-
Referee: [Abstract] Abstract: the headline mean errors (4.1°, 5.4°, 5.51°) and the claim of statistically significant outperformance are presented without standard deviations, dataset sizes (train/test splits), number of images or patients, or any statistical test results. This directly weakens the assertion that the method remains within clinical observer variability and outperforms landmarks.
Authors: We agree that the abstract would benefit from these details to better substantiate the claims. In the revised version we will incorporate the standard deviations, dataset sizes (including train/test splits, image and patient counts), and statistical test results (e.g., p-values from paired tests) directly into the abstract while preserving its conciseness. revision: yes
-
Referee: [Abstract] Abstract / method description: the paper states that false-positive reduction strategies are incorporated, yet supplies no quantitative characterization of the proposal network (inlier ratio, precision, false-positive rate) on the test sets, nor any ablation that isolates the contribution of the robust fitting stage versus the network alone. Because the three tasks involve distinct artifact profiles, this leaves the central robustness claim untested.
Authors: The manuscript contains ablations in the experiments section that compare the full pipeline against the proposal network alone. To address the abstract-level concern we will add concise quantitative metrics (inlier ratios, precision) and a note on the fitting-stage contribution to the revised abstract. revision: yes
-
Referee: [Abstract] Abstract: no details are given on how the false-positive reduction was implemented or tuned, nor on whether the same hyper-parameters were used across the radiograph and ultrasound tasks. This information is load-bearing for the claim that the pipeline generalizes without systematic bias from network errors.
Authors: We will revise the abstract to include a brief description of the false-positive reduction implementation, tuning procedure, and confirmation that consistent hyper-parameters were applied across tasks. revision: yes
Circularity Check
No circularity: empirical pipeline with independent validation
full rationale
The paper describes a two-stage method (learning-based point proposal + RANSAC/Hough robust fitting) and reports measured mean angular errors on three clinical tasks. No equations, fitted parameters, or self-citations are presented that reduce any claimed result or derivation to the inputs by construction. The performance numbers are post-hoc empirical outcomes, not quantities defined or forced by the method itself. The derivation chain is therefore self-contained and non-circular.
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.