Explaining Unsupervised Disease Staging in Huntington's Disease: Insights into Model Representations and Clusters
Pith reviewed 2026-06-27 22:19 UTC · model grok-4.3
The pith
Unsupervised embeddings for Huntington's disease staging align with clinical motor and functional scores.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
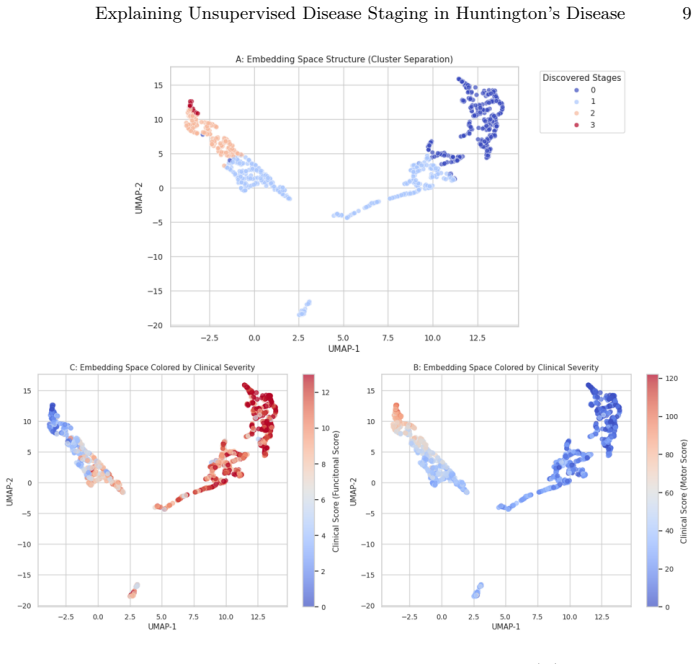
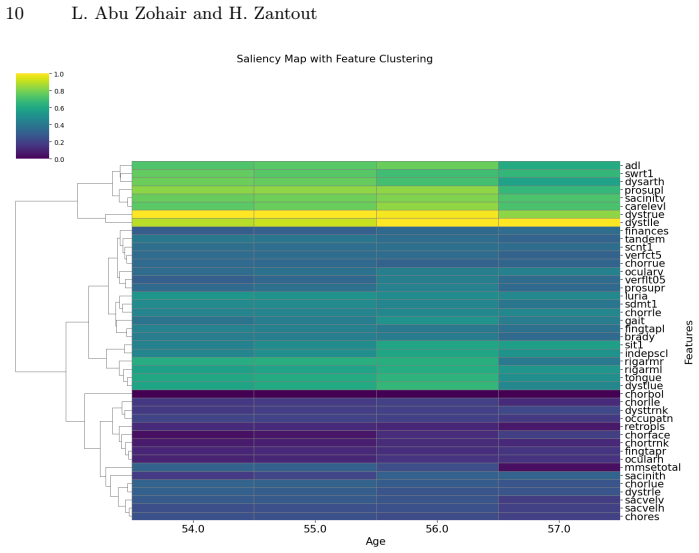
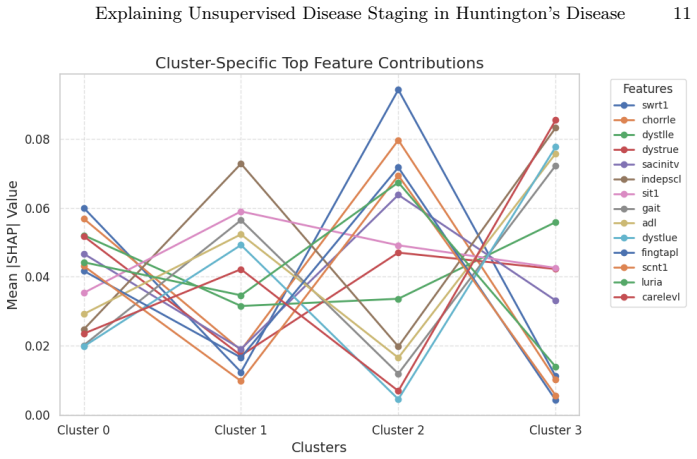
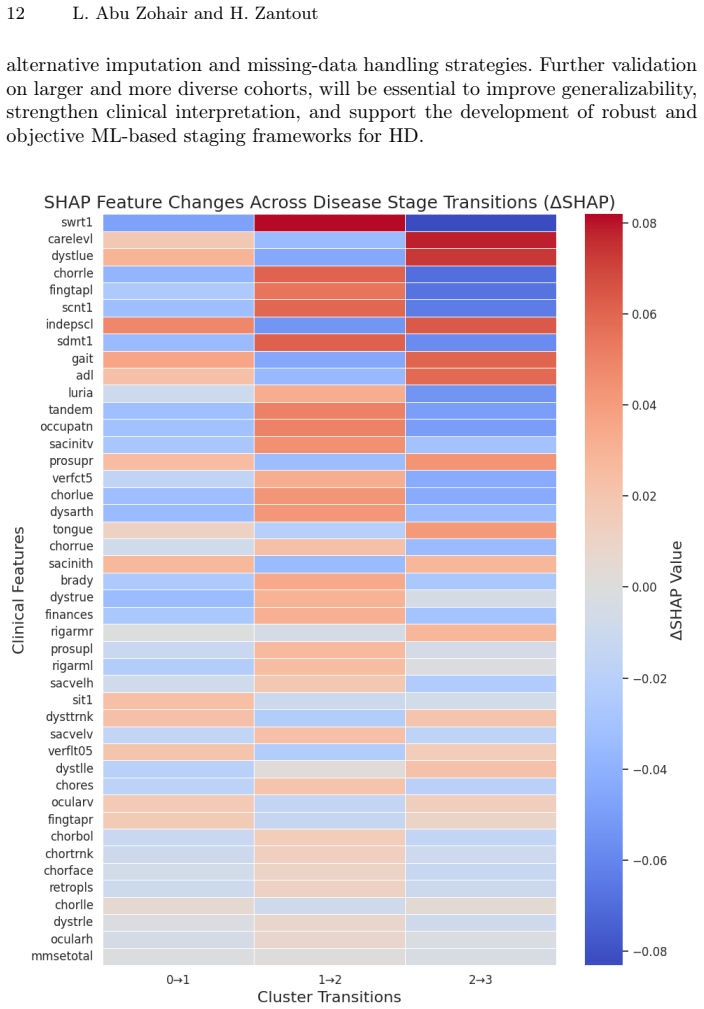
The explainability analysis indicates that the learned embeddings capture clinically meaningful disease structure, aligning with established motor and functional severity scores and exhibiting progressive deterioration across clusters. SHAP reveals a stratification of disease stages, ranging from early cognitive-motor impairment to severe functional dependency, consistent with known clinical progression patterns, while also highlighting intra-stage variability.
What carries the argument
Surrogate classifier with SHAP applied to the unsupervised embeddings to quantify feature contributions to cluster assignments.
If this is right
- The discovered clusters exhibit progressive deterioration consistent with clinical measures.
- Motor and functional scores are the primary drivers of the learned embeddings over time.
- SHAP identifies transitions between stages from early impairment to severe dependency.
- The embeddings exhibit intra-stage variability within the overall progression pattern.
Where Pith is reading between the lines
- The same explainability approach could be applied to unsupervised staging models for other progressive diseases to check for similar clinical alignment.
- If the surrogate approximation holds, the identified features could be prioritized in future data collection for HD monitoring.
- The stratification suggests the model could support finer-grained tracking of stage transitions in longitudinal studies.
Load-bearing premise
The surrogate classifier produces SHAP values that accurately reflect the original unsupervised model's internal feature contributions.
What would settle it
Re-training a different surrogate model on the same embeddings yields substantially different SHAP rankings for the same clusters, or new patient data shows clusters that fail to align with motor and functional severity scores.
Figures
read the original abstract
Huntington's disease (HD) is a progressive neurodegenerative disorder that affects motor, cognitive, and behavioral functions, where accurate characterization of disease progression remains essential to improve patient outcome and quality of life. Unsupervised machine learning (ML) approaches have demonstrated the ability to uncover disease progression trajectories and meaningful latent stages from longitudinal data; however, their limited interpretability restricts clinical trust and translation. We extend a previously proposed ML-based disease staging framework by applying an explainability analysis to the extracted feature representations and discovered disease stages. Applied to the Enroll-HD dataset, we first project the learned representations into a lower-dimensional space to intuitively assess whether the resulting clusters align with the progression of established clinical measures. We then use saliency maps to identify the clinical features that most strongly contribute to the learned embeddings over time. Finally, we train a surrogate classifier and apply SHAP to quantify feature importance for cluster assignments and to analyze which clinical variables drive transitions between disease stages. The explainability analysis indicates that the learned embeddings capture clinically meaningful disease structure, aligning with established motor and functional severity scores and exhibiting progressive deterioration across clusters. Within this analysis, SHAP reveals a stratification of disease stages, ranging from early cognitive-motor impairment to severe functional dependency, consistent with known clinical progression patterns, while also highlighting intra-stage variability.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript extends a prior unsupervised ML disease staging framework for Huntington's disease by applying explainability methods to embeddings learned from the Enroll-HD longitudinal dataset. It projects embeddings to assess cluster alignment with clinical progression, uses saliency maps to identify feature contributions to embeddings over time, and trains a surrogate classifier to enable SHAP analysis of feature importance for cluster assignments and stage transitions. The central claim is that the embeddings capture clinically meaningful structure (aligning with motor/functional scores and showing progressive deterioration) and that SHAP reveals stratification from early cognitive-motor impairment to severe functional dependency consistent with known patterns.
Significance. If the surrogate-based SHAP attributions and alignment claims hold after verification, the work would strengthen interpretability of unsupervised disease staging models, potentially increasing clinical trust and translation for progressive disorders like HD by linking latent representations to established clinical measures.
major comments (3)
- [Abstract / Methods] Abstract and Methods (surrogate classifier description): The central claim that SHAP 'reveals a stratification of disease stages' and 'quantif[ies] feature importance for cluster assignments' rests on a surrogate classifier trained to predict the unsupervised clusters, yet no fidelity metrics (accuracy, calibration, or agreement with original embedding geometry) are reported; any systematic mismatch would directly distort the reported feature importances and intra-stage variability.
- [Abstract] Abstract (results claims): The assertion that embeddings 'align with established motor and functional severity scores' and exhibit 'progressive deterioration across clusters' is presented without quantitative support such as correlation coefficients, statistical tests, or error bars, which is load-bearing for the 'clinically meaningful disease structure' conclusion.
- [Abstract / Discussion] Abstract / Discussion: The analysis learns representations from the same clinical features later used to evaluate alignment with motor/functional scores and to interpret SHAP values, creating a circularity risk that is not addressed with controls or sensitivity checks; this undermines the independence of the 'consistent with known clinical progression patterns' claim.
minor comments (1)
- [Abstract] The abstract would be clearer if it specified the number of discovered clusters/stages, the exact clinical scores (e.g., UHDRS motor, TFC), and the dimensionality reduction technique used for visualization.
Simulated Author's Rebuttal
We thank the referee for their constructive feedback, which highlights important aspects of methodological transparency and claim support. We address each major comment below with point-by-point responses. Revisions will be incorporated to strengthen the manuscript where indicated.
read point-by-point responses
-
Referee: [Abstract / Methods] Abstract and Methods (surrogate classifier description): The central claim that SHAP 'reveals a stratification of disease stages' and 'quantif[ies] feature importance for cluster assignments' rests on a surrogate classifier trained to predict the unsupervised clusters, yet no fidelity metrics (accuracy, calibration, or agreement with original embedding geometry) are reported; any systematic mismatch would directly distort the reported feature importances and intra-stage variability.
Authors: We agree that fidelity metrics are critical to validate the surrogate and ensure SHAP attributions are trustworthy. The full manuscript describes the surrogate training but does not explicitly tabulate fidelity metrics in the provided sections. In the revision, we will add a dedicated subsection reporting accuracy, calibration plots, and agreement (e.g., adjusted Rand index) between surrogate predictions and original cluster assignments, confirming high fidelity to support the reported SHAP results. revision: yes
-
Referee: [Abstract] Abstract (results claims): The assertion that embeddings 'align with established motor and functional severity scores' and exhibit 'progressive deterioration across clusters' is presented without quantitative support such as correlation coefficients, statistical tests, or error bars, which is load-bearing for the 'clinically meaningful disease structure' conclusion.
Authors: We acknowledge that the abstract would benefit from explicit quantitative anchors. The full manuscript contains correlation analyses and statistical tests in the Results, but these are not summarized numerically in the abstract. We will revise the abstract to include key quantitative results (e.g., Spearman correlation coefficients with motor/functional scores and associated p-values) while maintaining brevity. revision: yes
-
Referee: [Abstract / Discussion] Abstract / Discussion: The analysis learns representations from the same clinical features later used to evaluate alignment with motor/functional scores and to interpret SHAP values, creating a circularity risk that is not addressed with controls or sensitivity checks; this undermines the independence of the 'consistent with known clinical progression patterns' claim.
Authors: This concern about circularity is substantive. The unsupervised model discovers latent structure without supervision from the clinical scores, and post-hoc alignment with specific motor/functional measures is a standard validation approach. However, to directly address potential dependence, the revised manuscript will include sensitivity analyses (e.g., ablation of motor/functional features from the input set followed by re-evaluation of cluster alignment) and report whether progressive patterns remain consistent. revision: yes
Circularity Check
No significant circularity; external clinical benchmarks keep derivation independent
full rationale
The paper applies unsupervised clustering to Enroll-HD longitudinal data, projects embeddings for visual alignment against established motor/functional severity scores, generates saliency maps on the learned representations, and trains a surrogate classifier solely to enable SHAP interpretation of the resulting cluster labels. These steps compare discovered structure to independent clinical measures and known progression patterns rather than deriving claims tautologically from fitted inputs or self-citations. No equations reduce a claimed prediction to its own training targets by construction, no uniqueness theorems are imported from prior author work, and no ansatz is smuggled via citation. The chain remains self-contained against external benchmarks.
Axiom & Free-Parameter Ledger
Reference graph
Works this paper leans on
-
[1]
org/10.1016/S0166-2236(00)01568-X
Jakel,R.J.,Maragos,W.F.:NeuronalcelldeathinHuntington’sdisease:apotential role for dopamine.Trends in Neurosciences23(6), 239–245 (2000).https://doi. org/10.1016/S0166-2236(00)01568-X
-
[2]
Abu Zohair, L.M., Zantout, H., Vallejo, M., Uddin, M.A., Mahmoud, A.: Arti- ficial intelligence and machine learning for the diagnosis of Huntington disease: a narrative review.Journal of Medical Artificial Intelligence9(2025).https: //jmai.amegroups.org/article/view/10176
2025
-
[3]
Abu Zohair, L.M., Zantout, H., Vallejo, M., Uddin, M.A.: Unsupervised machine learning using cerebrospinal fluid proteomics for understanding Parkinson’s disease progression.Proceedings of the AAAI Symposium Series6(1),72–74(2025).https: //doi.org/10.1609/aaaiss.v6i1.36033
-
[4]
Ross, C.A., Tabrizi, S.J.: Huntington’s disease: from molecular pathogenesis to clinical treatment.The Lancet Neurology10(1), 83–98 (2011).https://doi.org/ 10.1016/S1474-4422(10)70245-3
-
[5]
Shoulson, I., Fahn, S.: Huntington disease: clinical care and evaluation.Neurology 29(1), 1–3 (1979).https://doi.org/10.1212/WNL.29.1.1
-
[6]
Tabrizi,S.J.etal.:AbiologicalclassificationofHuntington’sdisease:theIntegrated Staging System.The Lancet Neurology21(7), 632–644 (2022).https://doi.org/ 10.1016/S1474-4422(22)00120-X
-
[7]
et al.: Rating scales for cognition in Huntington’s disease: critique and recommendations.Movement Disorders33(2) (2018).https://doi.org/10
Mestre, T.A. et al.: Rating scales for cognition in Huntington’s disease: critique and recommendations.Movement Disorders33(2) (2018).https://doi.org/10. 1002/mds.27227
2018
-
[8]
https://doi.org/10.1002/mdc3.12618 14 L
Winder, J.Y., Roos, R.A.C., Burgunder, J.-M., Marinus, J., Reilmann, R.: Inter- rater reliability of the Unified Huntington’s Disease Rating Scale – Total Motor Score certification.Movement Disorders Clinical Practice5(3), 290–295 (2018). https://doi.org/10.1002/mdc3.12618 14 L. Abu Zohair and H. Zantout
-
[9]
Sampaio, C. et al.: Refining the language of Huntington’s disease progression with HD-ISS.Journal of Huntington’s Disease13(2), 115–118 (2024).https://doi. org/10.3233/JHD-240043
-
[10]
et al.: Classification of manifest Huntington disease using vowel distor- tion measures
Romana, A. et al.: Classification of manifest Huntington disease using vowel distor- tion measures. In:Interspeech(2020), pp. 4966–4970.https://doi.org/10.21437/ Interspeech.2020-2724
2020
-
[11]
Paulsen, J.S., Burks, D.K.: Revised diagnostic criteria for Huntington disease.Neu- rology Clinical Practice15(2), e200430 (2025).https://doi.org/10.1212/CPJ. 0000000000200430
work page doi:10.1212/cpj 2025
-
[12]
Abu Zohair, L.M., Vallejo, M., Uddin, M.A., Woodward, J.R., Zantout, H.: A Machine Learning-Based Framework for Discovering Huntington’s Disease Stages: Integrating Graph Representation Learning and Clustering to Uncover Pro- gression Dynamics in Longitudinal Enroll-HD Dataset. 2026. arXiv:2606.06196. https://arxiv.org/abs/2606.06196
work page internal anchor Pith review Pith/arXiv arXiv 2026
-
[13]
Lubna Mahmoud Abuzohair, Hind Zantout, Md Azher Uddin et al. A Novel Dy- namic Graph Architecture for Staging Parkinson’s Disease Progression Using Cere- brospinal Fluids Longitudinal Profiles, 08 March 2026, PREPRINT (Version 1) availableatResearchSquareResearch Square(2026).https://doi.org/10.21203/ rs.3.rs-9034342/v1
2026
-
[14]
Ren, Z. et al.: Regularized feature reconstruction for spatio-temporal saliency de- tection.IEEE Transactions on Image Processing22(8), 3120–3132 (2013).https: //doi.org/10.1109/TIP.2013.2259837
-
[15]
UMAP: Uniform Manifold Approximation and Projection for Dimension Reduction
McInnes, L., Healy, J., Melville, J.: UMAP: Uniform Manifold Approximation and Projection for Dimension Reduction. arXiv preprint arXiv:1802.03426 (2020). https://arxiv.org/abs/1802.03426
work page internal anchor Pith review Pith/arXiv arXiv 2020
-
[16]
Enroll-HD: Enroll-HD Data Dictionary. (2025).https:// enroll-hd.org/for-researchers/data-support-documentation/ #documentation/doc-details2/68b60a0a59371b02d0740572/kn-asset/ 103-206-137-68b609da96de8802d6a30de6/enrollhd_datadictionary_ 20250807.xlsx
2025
-
[17]
CHDI Foundation: PDS7 Overview: Dataset overview. (2025).https: //enroll-hd.org/for-researchers/data-support-documentation/ #documentation/doc-details2/68ac787cf252ac044f5a0833/kn-asset/ 103-206-137-6900e9ff885d080310120b70/enrollhd_pds7overview_20251028. pdf
2025
-
[18]
CHDI Foundation: Enroll-HD acknowledgement list.https:// enroll-hd.org/for-researchers/data-support-documentation/ #documentation/doc-details2/68ac76f628f56202b991fc57/kn-asset/ 103-206-137-68ac76cc1c6fff02b835133a/enrollhd_acknowledgementlist_ 20250821.pdf
-
[19]
Deep Inside Convolutional Networks: Visualising Image Classification Models and Saliency Maps
Simonyan, K., Vedaldi, A., Zisserman, A.: Deep inside convolutional networks: visualising saliency maps. arXiv preprint arXiv:1312.6034 (2014).https://arxiv. org/abs/1312.6034
work page internal anchor Pith review Pith/arXiv arXiv 2014
-
[20]
et al.: From clustering to cluster explanations via neural networks
Kauffmann, J. et al.: From clustering to cluster explanations via neural networks. IEEE Transactions on Neural Networks and Learning Systems35(2), 1926–1940 (2024).https://doi.org/10.1109/TNNLS.2022.3185901
-
[21]
Ross, C.A., Aylward, E.H., Wild, E.J., Langbehn, D.R., Long, J.D., Warner, J.H., Scahill, R.I., Leavitt, B.R., Stout, J.C., Paulsen, J.S., Reilmann, R., Unschuld, P.G., Wexler, A., Margolis, R.L., Tabrizi, S.J.: Huntington disease: natural history, biomarkers and prospects for therapeutics.Nature Reviews Neurology10(4), 204– 216 (2014).https://doi.org/10....
-
[22]
The Huntington’s Disease Collaborative Research Group: Huntington disease.Na- ture Reviews Disease Primers1, 15052 (2015).https://doi.org/10.1038/nrdp. 2015.52
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.