"Where is this coming from?" Uncovering Trustworthiness Ideals in AI-powered Peripartum Information Seeking
Pith reviewed 2026-06-27 14:28 UTC · model grok-4.3
The pith
In maternal health, AI trustworthiness must be inspectable and not asserted by the system.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
In high-stakes health contexts shaped by historical inequities, trustworthiness must be inspectable and not asserted. While stakeholders diverge on what makes information credible, they converge on the need for transparency, recourse, and ecosystem complementarity. The analysis of the focus group discussions yields four themes and corresponding governance requirements: support for social and identity-based sensemaking, pluralistic verification practices, inspectable governance with recourse mechanisms, and ecosystem-aware integration that avoids shifting burden.
What carries the argument
Inductive thematic analysis of focus-group transcripts that extracts four governance requirements from stakeholder reactions to an AI factual-answering design probe.
If this is right
- AI systems for peripartum information should incorporate mechanisms that let users inspect how answers are generated and challenge them.
- Designs must accommodate pluralistic verification rather than enforcing a single source of authority.
- Integration of AI tools should complement rather than displace existing clinical and community support structures.
- Human-AI evaluation protocols should expand to include assessments of recourse and ecosystem fit.
Where Pith is reading between the lines
- The same inspectability requirements may surface in other high-stakes domains where historical distrust of institutions exists, such as mental health or chronic disease management.
- Developers could operationalize recourse through auditable logs or appeal channels that users can actually access without technical expertise.
- Testing whether systems built around these four requirements measurably reduce information disparities would provide a concrete next step.
Load-bearing premise
The patterns observed in four focus groups with 24 participants from three stakeholder groups are sufficient to identify general governance requirements that hold beyond this sample.
What would settle it
A larger study with additional stakeholder groups or different geographic settings that finds no convergence on the need for inspectable governance, transparency, and recourse would undermine the central claim.
Figures

read the original abstract
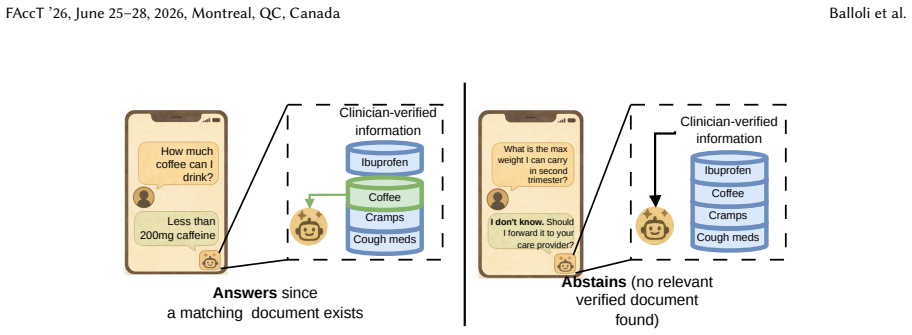
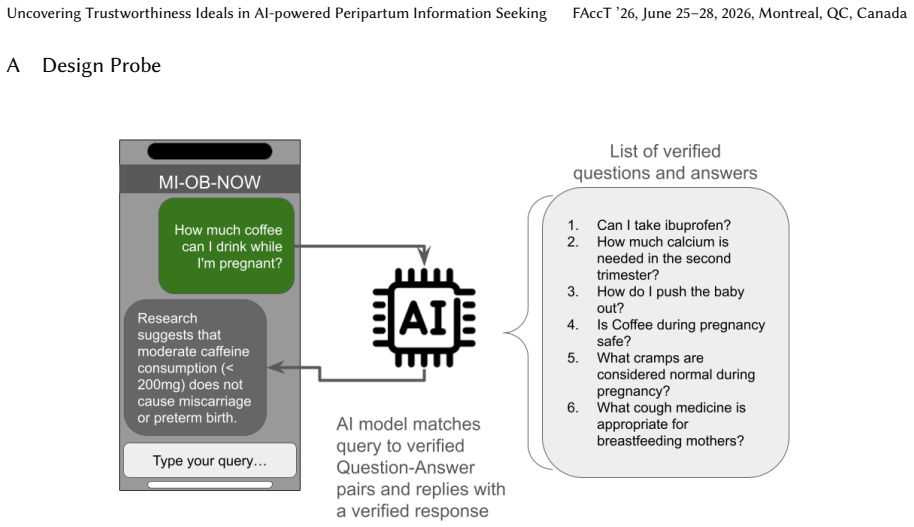
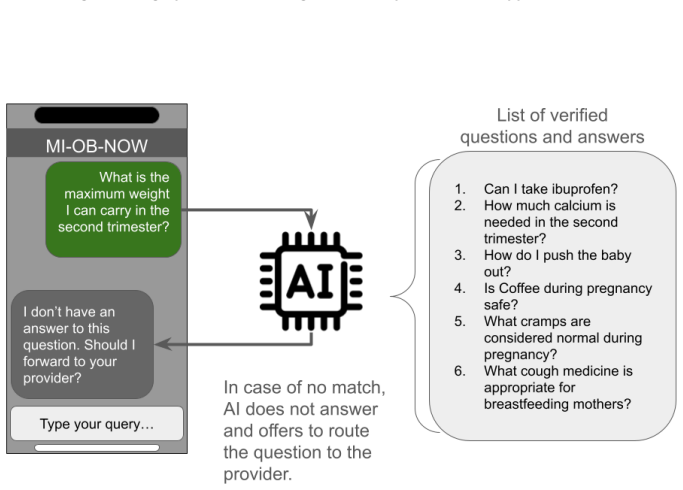
AI-powered tools increasingly promise to fill information gaps in health, especially in domains like maternal and reproductive health that demand timely, accurate, and actionable information. This is extremely important, as the United States leads peer nations in preventable deaths, with stark racial disparities. However, current AI and NLP-powered systems aim to improve access to vetted maternal health information by routing user queries to a factual response while under-specifying the socio-technical governance structures that shape trust, use, and harm in practice. We report findings from four synchronous focus groups ($n=24$) with three stakeholder groups central to peripartum information support: birthing people, clinicians, and health workers (e.g., doulas, social workers, community health workers) exploring topics around information seeking, experience with current clinical infrastructure, misinformation, and an AI-enabled factual answering tool design probe. Our inductive analysis surfaces a central finding: in high-stakes health contexts shaped by historical inequities, trustworthiness must be inspectable and not asserted. While stakeholders diverge on what makes information credible, they converge on the need for transparency, recourse, and ecosystem complementarity. Based on the discussions, we identify four themes and governance requirements: (1) support for social and identity-based sensemaking, (2) pluralistic verification practices, (3) inspectable governance with recourse mechanisms, and (4) ecosystem-aware integration that avoids shifting burden. Building on these findings, we propose design artifacts that are mistrust-aware and promote principled governance mechanisms for transparent, pluralistic AI systems. Finally, we discuss the implications of our findings for expanding human-AI evaluations and improving the transparency of deployed AI systems.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript reports results from four synchronous focus groups (n=24) with birthing people, clinicians, and health workers (doulas, social workers, community health workers). Using inductive thematic analysis of discussions on information seeking, clinical infrastructure, misinformation, and an AI factual-answering design probe, the authors surface the claim that trustworthiness in high-stakes peripartum AI systems must be inspectable rather than asserted. Stakeholders diverge on credibility criteria yet converge on transparency, recourse, and ecosystem complementarity; the analysis yields four themes and associated governance requirements, which the authors translate into mistrust-aware design artifacts and implications for human-AI evaluation.
Significance. If the themes are robust, the work supplies concrete, stakeholder-derived requirements for inspectable governance in AI health tools operating in contexts marked by historical inequities. It contributes to HCI and responsible-AI scholarship by linking transparency and recourse mechanisms to reduced burden-shifting and by proposing design artifacts that treat mistrust as a design input rather than a deficit to be corrected.
major comments (2)
- [Methods section (thematic analysis description)] Methods section (thematic analysis description): the inductive coding process, codebook development, inter-rater reliability statistics, member checking, and handling of divergent views are not reported. Because the central claim of convergence on transparency/recourse/ecosystem complementarity and the four governance requirements are derived directly from this analysis of n=24 transcripts, the absence of these details prevents verification that the themes are stable outputs rather than artifacts of the specific sample or analyst.
- [Findings and Implications sections] Findings and Implications sections: the manuscript moves from local observations in a convenience sample of three stakeholder groups to prescriptive “governance requirements” and design recommendations without reporting participant demographics (race, socioeconomic status, geography), recruitment strategy, or theoretical saturation. This step is load-bearing for the claim that the reported convergence applies beyond the sampled individuals and settings to broader AI governance in maternal health.
minor comments (2)
- [Abstract] Abstract: the phrase “four synchronous focus groups (n=24)” should clarify whether groups were homogeneous or mixed by stakeholder type, as this affects interpretation of divergence and convergence claims.
- [Methods] The design-probe description could include the exact prompt template or example outputs shown to participants to allow readers to assess how the probe may have shaped the elicited themes.
Simulated Author's Rebuttal
We thank the referee for the detailed and constructive report. The two major comments identify important gaps in reporting that affect the verifiability and scope of our claims. We respond to each below and indicate planned revisions.
read point-by-point responses
-
Referee: Methods section (thematic analysis description): the inductive coding process, codebook development, inter-rater reliability statistics, member checking, and handling of divergent views are not reported. Because the central claim of convergence on transparency/recourse/ecosystem complementarity and the four governance requirements are derived directly from this analysis of n=24 transcripts, the absence of these details prevents verification that the themes are stable outputs rather than artifacts of the specific sample or analyst.
Authors: We agree that greater transparency in the analytic process is needed. The revised manuscript will expand the Methods section to detail the iterative, team-based codebook development (two researchers independently coded a subset of transcripts, met to reconcile differences through discussion, and refined codes until consensus), how divergent views were resolved via team deliberation rather than statistical agreement, and the limited member-checking steps performed with two participants. Formal inter-rater reliability statistics were not calculated because the analysis was inductive and consensus-driven; we will state this rationale explicitly. revision: yes
-
Referee: Findings and Implications sections: the manuscript moves from local observations in a convenience sample of three stakeholder groups to prescriptive “governance requirements” and design recommendations without reporting participant demographics (race, socioeconomic status, geography), recruitment strategy, or theoretical saturation. This step is load-bearing for the claim that the reported convergence applies beyond the sampled individuals and settings to broader AI governance in maternal health.
Authors: We accept that these elements are necessary for readers to assess transferability. The revised manuscript will add a detailed description of the convenience sampling and recruitment strategy (via community organizations and clinical networks) and a statement on theoretical saturation (analysis continued until no new themes emerged across groups). However, granular demographic variables such as race, socioeconomic status, and geography were not collected, as the study design prioritized stakeholder role over individual identity characteristics; we will note this as a limitation and temper claims about broader applicability accordingly. revision: partial
Circularity Check
No circularity: inductive qualitative findings from focus groups
full rationale
The paper reports results of inductive thematic analysis on transcripts from four focus groups (n=24). No equations, fitted parameters, predictions, or derivations appear. The central claims (trustworthiness must be inspectable; convergence on transparency/recourse/ecosystem complementarity) are presented as outputs of the analysis rather than quantities defined in terms of the input data or reduced by self-citation. No load-bearing self-citation, ansatz smuggling, or renaming of known results is present in the provided text. The derivation chain is self-contained as standard qualitative reporting.
Axiom & Free-Parameter Ledger
axioms (1)
- domain assumption Inductive thematic analysis of focus-group transcripts produces reliable, generalizable governance requirements for AI systems.
Reference graph
Works this paper leans on
-
[1]
ACOG. [n. d.]. Dictionary. https://www.acog.org/womens-health/dictionary
-
[2]
Julia Adler-Milstein, Wendi Zhao, Rachel Willard-Grace, Margae Knox, and Kevin Grumbach. 2020. Electronic health records and burnout: time spent on the electronic health record after hours and message volume associated with exhaustion but not with cynicism among primary care clinicians.Journal of the American Medical Informatics Association27, 4 (2020), 531–538
2020
-
[3]
Alvarado, Lucy Lu Wang, and Irene Y
Maria Antoniak, Aakanksha Naik, Carla S. Alvarado, Lucy Lu Wang, and Irene Y. Chen. 2024. NLP for Maternal Healthcare: Perspectives and Guiding Principles in the Age of LLMs. InProceedings of the 2024 ACM Conference on Fairness, Accountability, and Transparency(Rio de Janeiro, Brazil)(FAccT ’24). Association for Computing Machinery, New York, NY, USA, 144...
-
[4]
Merrill, Kristi E Gamarel, and Oliver L
Laima Augustaitis, Leland A. Merrill, Kristi E Gamarel, and Oliver L. Haimson. 2021. Online Transgender Health Information Seeking: Facilitators, Barriers, and Future Directions. InProceedings of the 2021 CHI Conference on Human Factors in Computing Systems(Yokohama, Japan)(CHI ’21). Association for Computing Machinery, New York, NY, USA, Article 205, 14 ...
-
[5]
Emily P Backes, Susan C Scrimshaw, and National Academies of Sciences, Engineering, and Medicine and others. 2020. Maternal and newborn care in the United States. InBirth Settings in America: Outcomes, Quality, Access, and Choice. National Academies Press (US)
2020
-
[6]
Naveen Bagalkot, Syeda Zainab Akbar, Swati Sharma, Nicola Mackintosh, Deirdre Harrington, Paula Griffiths, Judith Angelitta Noronha, and Nervo Verdezoto. 2022. Embodied Negotiations, Practices and Experiences Interacting with Pregnancy Care Infrastructures in South India. InProceedings of the 2022 CHI Conference on Human Factors in Computing Systems(New O...
-
[7]
Zinzi D Bailey, Nancy Krieger, Madina Agénor, Jasmine Graves, Natalia Linos, and Mary T Bassett. 2017. Structural racism and health inequities in the USA: evidence and interventions.The lancet389, 10077 (2017), 1453–1463
2017
-
[8]
Gagan Bansal, Besmira Nushi, Ece Kamar, Eric Horvitz, and Daniel S Weld. 2021. Is the most accurate ai the best teammate? optimizing ai for teamwork. InProceedings of the AAAI Conference on Artificial Intelligence, Vol. 35. 11405–11414
2021
-
[9]
Barnes, Lesley Barclay, Kirsten McCaffery, and Parisa Aslani
Larisa A.J. Barnes, Lesley Barclay, Kirsten McCaffery, and Parisa Aslani. 2019. Complementary medicine products: Information sources, perceived benefits and maternal health literacy.Women and Birth32, 6 (2019), 493–520. doi:10.1016/j.wombi.2018.11.015
-
[10]
Abeba Birhane, William Isaac, Vinodkumar Prabhakaran, Mark Diaz, Madeleine Clare Elish, Iason Gabriel, and Shakir Mohamed. 2022. Power to the people? Opportunities and challenges for participatory AI. InProceedings of the 2nd ACM Conference on Equity and Access in Algorithms, Mechanisms, and Optimization. 1–8
2022
-
[11]
Elizabeth Bondi, Raphael Koster, Hannah Sheahan, Martin Chadwick, Yoram Bachrach, Taylan Cemgil, Ulrich Paquet, and Krishnamurthy Dvijotham. 2022. Role of human-AI interaction in selective prediction. InProceedings of the AAAI Conference on Artificial Intelligence, Vol. 36. 5286–5294
2022
-
[12]
Elizabeth Bondi, Lily Xu, Diana Acosta-Navas, and Jackson A Killian. 2021. Envisioning communities: a participatory approach towards AI for social good. InProceedings of the 2021 AAAI/ACM Conference on AI, Ethics, and Society. 425–436
2021
-
[13]
Zana Buçinca, Maja Barbara Malaya, and Krzysztof Z Gajos. 2021. To trust or to think: cognitive forcing functions can reduce overreliance on AI in AI-assisted decision-making.Proceedings of the ACM on Human-computer Interaction5, CSCW1 (2021), 1–21
2021
-
[14]
Ceren Budak, Brendan Nyhan, David M Rothschild, Emily Thorson, and Duncan J Watts. 2024. Misunderstanding the harms of online misinformation.Nature630, 8015 (2024), 45–53
2024
-
[15]
2006.Constructing grounded theory: A practical guide through qualitative analysis
Kathy Charmaz. 2006.Constructing grounded theory: A practical guide through qualitative analysis. sage
2006
-
[16]
Juanita J Chinn, Esther Eisenberg, Shavon Artis Dickerson, Rosalind B King, Nahida Chakhtoura, Issel Anne L Lim, Katherine L Grantz, Charisee Lamar, and Diana W Bianchi. 2020. Maternal mortality in the United States: research gaps, opportunities, and priorities. American journal of obstetrics and gynecology223, 4 (2020), 486–492
2020
-
[17]
Joia Crear-Perry, Rosaly Correa-de Araujo, Tamara Lewis Johnson, Monica R McLemore, Elizabeth Neilson, and Maeve Wallace. 2021. Social and structural determinants of health inequities in maternal health.Journal of women’s health30, 2 (2021), 230–235
2021
-
[18]
Dána-Ain Davis. 2019. Obstetric racism: the racial politics of pregnancy, labor, and birthing.Medical anthropology38, 7 (2019), 560–573
2019
-
[19]
Munmun De Choudhury, Meredith Ringel Morris, and Ryen W White. 2014. Seeking and sharing health information online: comparing search engines and social media. InProceedings of the SIGCHI conference on human factors in computing systems. 1365–1376
2014
-
[20]
Gunther Eysenbach, John Powell, Marina Englesakis, Carlos Rizo, and Anita Stern. 2004. Health related virtual communities and electronic support groups: systematic review of the effects of online peer to peer interactions.Bmj328, 7449 (2004), 1166
2004
-
[21]
Centers for Disease Control and Prevention (CDC). 2024. HEAR HER Campaign. https://www.cdc.gov/hearher/index.html
2024
-
[22]
Adam Fourney, Ryen W. White, and Eric Horvitz. 2015. Exploring Time-Dependent Concerns about Pregnancy and Childbirth from Search Logs. InProceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems(Seoul, Republic of Korea)(CHI ’15). Association for Computing Machinery, New York, NY, USA, 737–746. doi:10.1145/2702123.2702427
-
[23]
Derek M Griffith, Erin M Bergner, Alecia S Fair, and Consuelo H Wilkins. 2021. Using mistrust, distrust, and low trust precisely in medical care and medical research advances health equity.American journal of preventive medicine60, 3 (2021), 442–445
2021
-
[24]
Jacaranda Health. 2023. Jacaranda Health publications in maternal and newborn care. https://jacarandahealth.org/content_type/ publications/
2023
-
[25]
Hilary Hutchinson, Wendy Mackay, Bo Westerlund, Benjamin B Bederson, Allison Druin, Catherine Plaisant, Michel Beaudouin-Lafon, Stéphane Conversy, Helen Evans, Heiko Hansen, et al. 2003. Technology probes: inspiring design for and with families. InProceedings of the SIGCHI conference on Human factors in computing systems. 17–24
2003
-
[26]
Abigail Z. Jacobs and Hanna Wallach. 2021. Measurement and Fairness. InProceedings of the 2021 ACM Conference on Fairness, Accountability, and Transparency(Virtual Event, Canada)(FAccT ’21). Association for Computing Machinery, New York, NY, USA, 375–385. doi:10.1145/3442188.3445901
-
[27]
Jennifer N John, Sara Gorman, David Scales, and Jack Gorman. 2025. Online misleading information about women’s reproductive health: a narrative review.Journal of General Internal Medicine40, 5 (2025), 1123–1131. Uncovering Trustworthiness Ideals in AI-powered Peripartum Information Seeking FAccT ’26, June 25–28, 2026, Montreal, QC, Canada
2025
-
[28]
Grace J Johnson and Paul J Ambrose. 2006. Neo-tribes: The power and potential of online communities in health care.Commun. ACM 49, 1 (2006), 107–113
2006
-
[29]
Sadiya S Khan, Natalie A Cameron, and Kathryn J Lindley. 2023. Pregnancy as an early cardiovascular moment: peripartum cardiovascular health.Circulation research132, 12 (2023), 1584–1606
2023
-
[30]
Katy B Kozhimannil, Pinar Karaca-Mandic, Cori J Blauer-Peterson, Neel T Shah, and Jonathan M Snowden. 2017. Uptake and utilization of practice guidelines in hospitals in the United States: the case of routine episiotomy.The Joint Commission Journal on Quality and Patient Safety43, 1 (2017), 41–48
2017
-
[31]
Alyce Kuo and Stuti Dang. 2016. Secure messaging in electronic health records and its impact on diabetes clinical outcomes: a systematic review.Telemedicine and e-Health22, 9 (2016), 769–777
2016
-
[32]
Vivian Lai, Chacha Chen, Q Vera Liao, Alison Smith-Renner, and Chenhao Tan. 2021. Towards a science of human-ai decision making: a survey of empirical studies.arXiv preprint arXiv:2112.11471(2021)
arXiv 2021
-
[33]
Helen Levy and Alex Janke. 2016. Health literacy and access to care.Journal of health communication21, sup1 (2016), 43–50
2016
-
[34]
Q Vera Liao and S Shyam Sundar. 2022. Designing for responsible trust in AI systems: A communication perspective. InProceedings of the 2022 ACM conference on fairness, accountability, and transparency. 1257–1268
2022
-
[35]
Zachary J Madewell, Cynthia G Whitney, Sithembiso Velaphi, Portia Mutevedzi, Sana Mahtab, Shabir A Madhi, Ashleigh Fritz, Alim Swaray-Deen, Tom Sesay, Ikechukwu U Ogbuanu, et al. 2022. Prioritizing health care strategies to reduce childhood mortality.JAMA Network Open5, 10 (2022), e2237689–e2237689
2022
-
[36]
Elinor Mason. 2023. Value Pluralism. InThe Stanford Encyclopedia of Philosophy(Summer 2023 ed.), Edward N. Zalta and Uri Nodelman (Eds.). Metaphysics Research Lab, Stanford University
2023
-
[37]
Jonathan M Metzl and Helena Hansen. 2014. Structural competency: theorizing a new medical engagement with stigma and inequality. Social science & medicine103 (2014), 126–133
2014
-
[38]
Margaret Mitchell, Simone Wu, Andrew Zaldivar, Parker Barnes, Lucy Vasserman, Ben Hutchinson, Elena Spitzer, Inioluwa Deborah Raji, and Timnit Gebru. 2019. Model cards for model reporting. InProceedings of the conference on fairness, accountability, and transparency. 220–229
2019
-
[39]
Keisha E Montalmant and Anna K Ettinger. 2024. The racial disparities in maternal mortality and impact of structural racism and implicit racial bias on pregnant Black women: a review of the literature.Journal of racial and ethnic health disparities11, 6 (2024), 3658–3677
2024
-
[40]
Quynh C Nguyen, Elizabeth M Aparicio, Michelle Jasczynski, Amara Channell Doig, Xiaohe Yue, Heran Mane, Neha Srikanth, Francia Ximena Marin Gutierrez, Nataly Delcid, Xin He, et al. 2024. Rosie, a health education question-and-answer chatbot for new mothers: randomized pilot study.JMIR Formative Research8, 1 (2024), e51361
2024
-
[41]
Ziad Obermeyer, Brian Powers, Christine Vogeli, and Sendhil Mullainathan. 2019. Dissecting racial bias in an algorithm used to manage the health of populations.Science366, 6464 (2019), 447–453
2019
-
[42]
March of Dimes. [n. d.]. https://www.marchofdimes.org/maternity-care-deserts-report
-
[43]
American College of Obstetricians and Gynecologists (ACOG). 2020. Prenatal Care. https://www.acog.org/programs/redesigning- prenatal-care-initiative
2020
-
[44]
Vanessa O. Oguamanam, Natalie Hernandez, Rasheeta Chandler, Dominique Guillaume, Kai Mckeever, Morgan Allen, Sabreen Mo- hammed, and Andrea G Parker. 2023. An Intersectional Look at Use of and Satisfaction with Digital Mental Health Platforms: A Survey of Perinatal Black Women. InProceedings of the 2023 CHI Conference on Human Factors in Computing Systems...
-
[45]
2017.Medical bondage: Race, gender, and the origins of American gynecology
Deirdre Cooper Owens. 2017.Medical bondage: Race, gender, and the origins of American gynecology. University of Georgia Press
2017
-
[46]
Aasim I Padela, Liese Pruitt, and Saleha Mallick. 2017. The types of trust involved in American Muslim healthcare decisions: An exploratory qualitative study.Journal of religion and health56, 4 (2017), 1478–1488
2017
-
[47]
Saumya Pareek, Eduardo Velloso, and Jorge Goncalves. 2024. Trust Development and Repair in AI-Assisted Decision-Making during Complementary Expertise. InProceedings of the 2024 ACM Conference on Fairness, Accountability, and Transparency(Rio de Janeiro, Brazil)(FAccT ’24). Association for Computing Machinery, New York, NY, USA, 546–561. doi:10.1145/363010...
-
[48]
Alex Friedman Peahl, Alli Novara, Michele Heisler, Vanessa K Dalton, Michelle H Moniz, and Roger D Smith. 2020. Patient preferences for prenatal and postpartum care delivery: a survey of postpartum women.Obstetrics & Gynecology135, 5 (2020), 1038–1046
2020
-
[49]
Alex Friedman Peahl, Christopher M Zahn, Mark Turrentine, Wanda Barfield, Sean D Blackwell, Suni Jo Roberts, Allison R Powell, Vineet Chopra, and Steven J Bernstein. 2021. The Michigan plan for appropriate tailored healthcare in pregnancy prenatal care recommendations.Obstetrics & Gynecology138, 4 (2021), 593–602
2021
-
[50]
Cynthia Prather, Taleria R Fuller, William L Jeffries IV, Khiya J Marshall, A Vyann Howell, Angela Belyue-Umole, and Winifred King
-
[51]
Racism, African American women, and their sexual and reproductive health: a review of historical and contemporary evidence and implications for health equity.Health equity2, 1 (2018), heq–2017
2018
-
[52]
Farhat Tasnim Progga, Amal Khan, and Sabirat Rubya. 2024. Large language models and personalized storytelling for postpartum wellbeing. InCompanion Publication of the 2024 Conference on Computer-Supported Cooperative Work and Social Computing. 653–657. FAccT ’26, June 25–28, 2026, Montreal, QC, Canada Balloli et al
2024
-
[53]
Farhat Tasnim Progga, Avanthika Senthil Kumar, and Sabirat Rubya. 2023. Understanding the online social support dynamics for postpartum depression. InProceedings of the 2023 CHI Conference on Human Factors in Computing Systems. 1–17
2023
-
[54]
Mahima Pushkarna, Andrew Zaldivar, and Oddur Kjartansson. 2022. Data Cards: Purposeful and Transparent Dataset Documentation for Responsible AI. InProceedings of the 2022 ACM Conference on Fairness, Accountability, and Transparency(Seoul, Republic of Korea) (FAccT ’22). Association for Computing Machinery, New York, NY, USA, 1776–1826. doi:10.1145/3531146.3533231
-
[55]
Jean-Charles Rochet and Jean Tirole
Inioluwa Deborah Raji, Andrew Smart, Rebecca N. White, Margaret Mitchell, Timnit Gebru, Ben Hutchinson, Jamila Smith-Loud, Daniel Theron, and Parker Barnes. 2020. Closing the AI accountability gap: defining an end-to-end framework for internal algorithmic auditing. InProceedings of the 2020 Conference on Fairness, Accountability, and Transparency(Barcelon...
-
[56]
Pragnya Ramjee, Mehak Chhokar, Bhuvan Sachdeva, Mahendra Meena, Hamid Abdullah, Aditya Vashistha, Ruchit Nagar, and Mohit Jain. 2025. ASHABot: An LLM-Powered Chatbot to Support the Informational Needs of Community Health Workers. InProceedings of the 2025 CHI Conference on Human Factors in Computing Systems (CHI ’25). Association for Computing Machinery, ...
-
[57]
Leonardo Ranaldi and Giulia Pucci. 2023. When large language models contradict humans? large language models’ sycophantic behaviour.arXiv preprint arXiv:2311.09410(2023)
arXiv 2023
-
[58]
Raj M Ratwani. 2017. Electronic health records and improved patient care: opportunities for applied psychology.Current directions in psychological science26, 4 (2017), 359–365
2017
-
[59]
Joshua Jay Reicher and Murray Aaron Reicher. 2016. Implementation of certified EHR, patient portal, and “direct” messaging technology in a radiology environment enhances communication of radiology results to both referring physicians and patients.Journal of digital imaging29, 3 (2016), 337–340
2016
-
[60]
Sari L Reisner, Renee K Randazzo, Jaclyn M White Hughto, Sarah Peitzmeier, L Zachary DuBois, Dana J Pardee, Elliot Marrow, Sarah McLean, and Jennifer Potter. 2018. Sensitive health topics with underserved patient populations: Methodological considerations for online focus group discussions.Qualitative health research28, 10 (2018), 1658–1673
2018
-
[61]
Lisa S Rotenstein, A Jay Holmgren, N Lance Downing, and David W Bates. 2021. Differences in total and after-hours electronic health record time across ambulatory specialties.JAMA internal medicine181, 6 (2021), 863–865
2021
-
[62]
Andrew D Selbst, Danah Boyd, Sorelle A Friedler, Suresh Venkatasubramanian, and Janet Vertesi. 2019. Fairness and abstraction in sociotechnical systems. InProceedings of the conference on fairness, accountability, and transparency. 59–68
2019
-
[63]
Taylor Sorensen, Jared Moore, Jillian Fisher, Mitchell Gordon, Niloofar Mireshghallah, Christopher Michael Rytting, Andre Ye, Liwei Jiang, Ximing Lu, Nouha Dziri, et al. 2024. A roadmap to pluralistic alignment.arXiv preprint arXiv:2402.05070(2024)
Pith/arXiv arXiv 2024
-
[64]
Victor Suarez-Lledo and Javier Alvarez-Galvez. 2021. Prevalence of health misinformation on social media: systematic review.Journal of medical Internet research23, 1 (2021), e17187
2021
-
[65]
Northup, Kenneth Holstein, Haiyi Zhu, Hoda Heidari, and Hong Shen
Ningjing Tang, Jiayin Zhi, Tzu-Sheng Kuo, Calla Kainaroi, Jeremy J. Northup, Kenneth Holstein, Haiyi Zhu, Hoda Heidari, and Hong Shen. 2024. AI Failure Cards: Understanding and Supporting Grassroots Efforts to Mitigate AI Failures in Homeless Services(FAccT ’24). Association for Computing Machinery, New York, NY, USA, 713–732. doi:10.1145/3630106.3658935
-
[66]
Joanne Turnbull, Catherine Pope, Jane Prichard, Gemma McKenna, and Anne Rogers. 2019. A conceptual model of urgent care sense-making and help-seeking: a qualitative interview study of urgent care users in England.BMC Health Services Research19, 1 (2019), 481
2019
-
[67]
Tiffany C Veinot, Hannah Mitchell, and Jessica S Ancker. 2018. Good intentions are not enough: how informatics interventions can worsen inequality.Journal of the American Medical Informatics Association25, 8 (2018), 1080–1088
2018
-
[68]
Maaike Vogels-Broeke, Darie Daemers, Luc Budé, Raymond de Vries, and Marianne Nieuwenhuijze. 2022. Sources of information used by women during pregnancy and the perceived quality.BMC Pregnancy and Childbirth22, 1 (2022), 109
2022
-
[69]
Liang Wu, Fred Morstatter, Kathleen M Carley, and Huan Liu. 2019. Misinformation in social media: definition, manipulation, and detection.ACM SIGKDD explorations newsletter21, 2 (2019), 80–90
2019
-
[70]
Maie Zagloul, Buruj Mohammed, Nawara Abufares, Afsar Sandozi, Sarah Farhan, Saba Anwer, Shakirah Tumusiime, and Matida Bojang
-
[71]
Review of Muslim patient needs and its implications on healthcare delivery.Journal of Primary Care & Community Health15 (2024), 21501319241228740
2024
-
[72]
old school
Guido Zuccon, Bevan Koopman, and João Palotti. 2015. Diagnose This If You Can. InAdvances in Information Retrieval, Allan Hanbury, Gabriella Kazai, Andreas Rauber, and Norbert Fuhr (Eds.). Springer International Publishing, Cham, 562–567. Uncovering Trustworthiness Ideals in AI-powered Peripartum Information Seeking FAccT ’26, June 25–28, 2026, Montreal, ...
2015
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.