EmbodiedUS-FS: Fast Slow Intelligence for Ultrasound Robotics
Pith reviewed 2026-06-26 10:41 UTC · model grok-4.3
The pith
A fast-slow hierarchical embodied system improves success rates and reduces safety violations in robotic ultrasound scanning.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
The central discovery is that combining Slow Brain task-graph planning from implicit instructions, Fast Brain multimodal feedback for local refinements and recoveries, and a Safety Shield with escalation policy allows the robot to handle clinical workflow reasoning and dynamic execution challenges, leading to higher success rates and lower safety violations in evaluated scenarios.
What carries the argument
The fast-slow hierarchy consisting of the Slow Brain for intent parsing and plan verification, the Fast Brain for image-quality-guided recovery, and the Safety Shield for constraining actions.
If this is right
- Plans generated from natural-language instructions become executable and verifiable.
- Multimodal feedback enables recovery from perturbations like patient motion.
- Safety mechanisms reduce violations by triggering interventions before risks escalate.
- Overall task success improves in closed-loop settings with dynamic changes.
Where Pith is reading between the lines
- The design might extend to other image-guided robotic procedures beyond ultrasound.
- Physicians could interact more naturally without needing to specify every detail.
- Testing in varied clinical sites would reveal if the knowledge corpus covers enough cases.
Load-bearing premise
The system components will integrate and perform reliably when faced with real patient variability and unstated physician intentions not present in the test setups.
What would settle it
A trial where the robot encounters patient motions or anatomical variations outside the experiment conditions and the success rate drops or safety violations increase significantly.
Figures
read the original abstract
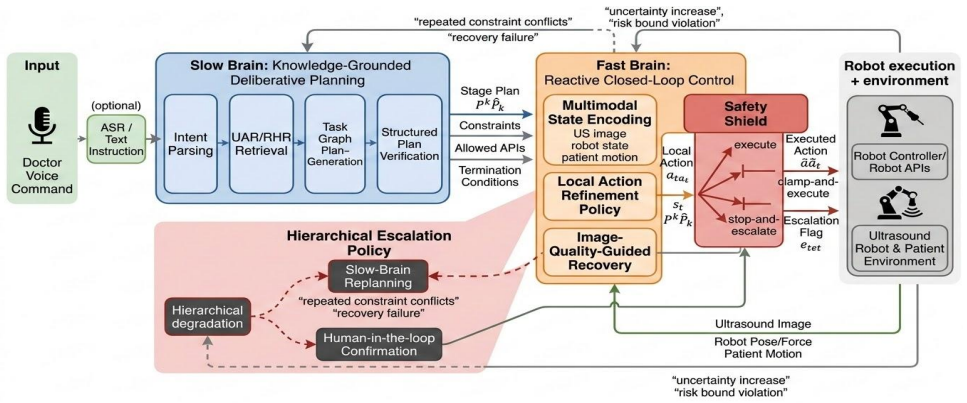
Robotic ultrasound scanning in real clinical environments requires both high-level clinical workflow reasoning and low-level closed-loop execution. Physicians natural-language instructions often contain implicit anatomical targets, procedural logic, image-quality requirements, and safety constraints, while execution is affected by patient motion, contact variations, and target drift. We propose a fast and slow hierarchical embodied ultrasound system for safe and interpretable robotic ultrasound assistance. The Slow Brain performs intent parsing and stage-wise task planning with knowledge augmentation from an API and handbook corpus, and generates executable plans through task-graph construction and structured plan verification. The Fast Brain fuses multimodal feedback, including ultrasound images, robot pose and force states, and patient-motion information, to refine local actions and perform image-quality-guided recovery behaviors. The system further integrates a Safety Shield and a hierarchical escalation policy to constrain risky actions and trigger replanning or human confirmation under persistent failures or safety-bound violations. Experiments on planning evaluation, closed-loop execution under dynamic perturbations, and safety-mechanism validation demonstrate that the proposed hierarchical design improves task success rates while reducing safety violations.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript proposes EmbodiedUS-FS, a hierarchical fast-slow embodied system for robotic ultrasound assistance. The Slow Brain parses physician natural-language instructions, augments knowledge from an API and handbook corpus, constructs task graphs, and performs structured plan verification. The Fast Brain fuses ultrasound images, robot pose/force, and patient-motion data for local action refinement and image-quality-guided recovery. A Safety Shield with hierarchical escalation constrains risky actions and triggers replanning or human confirmation on persistent failures. Experiments on planning evaluation, closed-loop execution under dynamic perturbations, and safety-mechanism validation are claimed to show that the hierarchical design improves task success rates while reducing safety violations.
Significance. If the experimental results are quantitatively robust, statistically significant, and generalize beyond the tested perturbations, the work could advance safe, interpretable robotic ultrasound systems by integrating high-level clinical reasoning with low-level multimodal control and explicit safety constraints. The approach directly targets documented clinical challenges (implicit targets, patient motion, contact variation, target drift). Strengths include the explicit separation of planning and execution layers plus the safety escalation policy; however, the absence of any reported metrics, baselines, or perturbation details in the manuscript text prevents evaluation of whether these strengths translate into measurable gains.
major comments (2)
- [Abstract] Abstract: The central claim that 'experiments ... demonstrate that the proposed hierarchical design improves task success rates while reducing safety violations' supplies no quantitative results, baselines, error bars, trial counts, statistical tests, or exclusion criteria. Without these, the performance improvement cannot be assessed and the soundness of the experimental validation is compromised.
- [Abstract] Abstract: The experiments are described only at the level of 'planning evaluation, closed-loop execution under dynamic perturbations, and safety-mechanism validation' without specifying perturbation distributions, patient-model diversity, or comparison to non-hierarchical baselines. This leaves the generalization step to real clinical environments (patient motion, contact variations, target drift, implicit anatomical targets) unsupported by the reported evidence.
minor comments (1)
- [Abstract] The abstract would be strengthened by including at least one key quantitative outcome (e.g., success-rate delta or safety-violation reduction) so readers can immediately gauge the magnitude of the reported improvement.
Simulated Author's Rebuttal
We thank the referee for the detailed feedback on the abstract. The comments correctly identify that the abstract currently provides only a high-level summary of the experimental claims without supporting quantitative details. We will revise the abstract in the next version to incorporate key metrics, baselines, and experimental specifications drawn from the body of the manuscript. Point-by-point responses follow.
read point-by-point responses
-
Referee: [Abstract] Abstract: The central claim that 'experiments ... demonstrate that the proposed hierarchical design improves task success rates while reducing safety violations' supplies no quantitative results, baselines, error bars, trial counts, statistical tests, or exclusion criteria. Without these, the performance improvement cannot be assessed and the soundness of the experimental validation is compromised.
Authors: We agree that the abstract as written does not supply the requested quantitative elements. The manuscript body contains the full experimental results (including success rates under the tested conditions, baseline comparisons, trial counts, and safety-violation counts), but these were not summarized in the abstract. In the revised version we will add a concise quantitative statement to the abstract that reports the observed improvements, trial numbers, and any statistical comparisons performed. revision: yes
-
Referee: [Abstract] Abstract: The experiments are described only at the level of 'planning evaluation, closed-loop execution under dynamic perturbations, and safety-mechanism validation' without specifying perturbation distributions, patient-model diversity, or comparison to non-hierarchical baselines. This leaves the generalization step to real clinical environments (patient motion, contact variations, target drift, implicit anatomical targets) unsupported by the reported evidence.
Authors: We accept that the abstract's experimental description is too terse. The body of the manuscript specifies the perturbation ranges, the patient phantoms used, and the non-hierarchical baselines against which the hierarchical system was compared. We will expand the abstract to include brief but concrete statements of these elements (perturbation distributions, model diversity, and baseline comparisons) so that the generalization argument is supported at the abstract level as well. revision: yes
Circularity Check
No circularity: architecture and experimental claims are independent of self-referential reductions
full rationale
The paper describes a hierarchical embodied system (Slow Brain task-graph planning with knowledge augmentation, Fast Brain multimodal recovery, Safety Shield with escalation) and reports that experiments on planning evaluation, closed-loop execution under dynamic perturbations, and safety validation show improved success rates and fewer violations. No equations, fitted parameters, predictions, or self-citations appear in the abstract or described content. The claims rest on experimental outcomes rather than any derivation that reduces by construction to its own inputs. This is a standard systems-description paper with no load-bearing circular steps.
Axiom & Free-Parameter Ledger
Reference graph
Works this paper leans on
-
[1]
Basics of ultrasound imaging,
V . Chan and A. Perlas, “Basics of ultrasound imaging,” inAtlas of ultrasound-guided procedures in interventional pain management. Springer, 2010, pp. 13–19
2010
-
[2]
Thoracic ultrasonog- raphy: a narrative review,
P. Mayo, R. Copetti, D. Feller-Kopman, G. Mathis, E. Maury, S. Mon- godi, F. Mojoli, G. V olpicelli, and M. Zanobetti, “Thoracic ultrasonog- raphy: a narrative review,”Intensive care medicine, vol. 45, no. 9, pp. 1200–1211, 2019
2019
-
[3]
An ultra-fast intrinsic contact sensing method for medical instruments with arbitrary shape,
G. Cao, M. Chen, J. Hu, and H. Liu, “An ultra-fast intrinsic contact sensing method for medical instruments with arbitrary shape,”RAL, vol. 8, no. 11, pp. 6955–6962, 2023
2023
-
[4]
Full-coverage path planning and stable interaction control for automated robotic breast ultrasound scanning,
Z. Wang, B. Zhao, P. Zhang, L. Yao, Q. Wang, B. Li, M. Q.-H. Meng, and Y . Hu, “Full-coverage path planning and stable interaction control for automated robotic breast ultrasound scanning,”IEEE Transactions on Industrial Electronics, vol. 70, no. 7, pp. 7051–7061, 2022
2022
-
[5]
Vision-language embodiment for monocular depth estimation,
J. Zhang and G. Lu, “Vision-language embodiment for monocular depth estimation,” inCVPR, 2025
2025
-
[6]
Automated genomic interpreta- tion via concept bottleneck models for medical robotics,
Z. Li, J. Zhang, M. Zhang, and G. Lu, “Automated genomic interpreta- tion via concept bottleneck models for medical robotics,”arXiv preprint arXiv:2510.01618, 2025
-
[7]
Recovering from failure by asking for help,
R. A. Knepper, S. Tellex, A. Li, N. Roy, and D. Rus, “Recovering from failure by asking for help,”Autonomous Robots, vol. 39, no. 3, pp. 347– 362, 2015
2015
-
[8]
A robotic ultrasound scanner for automatic vessel tracking and three-dimensional reconstruction of b-mode images,
S. Merouche, L. Allard, E. Montagnon, G. Soulez, P. Bigras, and G. Cloutier, “A robotic ultrasound scanner for automatic vessel tracking and three-dimensional reconstruction of b-mode images,”TUSON, 2015
2015
-
[9]
Real-time tissue tracking with b-mode ultrasound using speckle and visual servoing,
A. Krupa, G. Fichtinger, and G. D. Hager, “Real-time tissue tracking with b-mode ultrasound using speckle and visual servoing,” inMICCAI. Springer, 2007
2007
-
[10]
Image-guided control of a robot for medical ultrasound,
P. Abolmaesumi, S. E. Salcudean, W.-H. Zhu, M. R. Sirouspour, and S. P. DiMaio, “Image-guided control of a robot for medical ultrasound,” TRO, 2002
2002
-
[11]
Intensity-based direct visual servoing of an ultrasound probe,
C. Nadeau and A. Krupa, “Intensity-based direct visual servoing of an ultrasound probe,” inICRA. IEEE, 2011
2011
-
[12]
Automatic force-compliant robotic ultrasound screening of abdominal aortic aneurysms,
S. Virga, O. Zettinig, M. Esposito, K. Pfister, B. Frisch, T. Neff, N. Navab, and C. Hennersperger, “Automatic force-compliant robotic ultrasound screening of abdominal aortic aneurysms,” inIROS. IEEE, 2016
2016
-
[13]
A robotics-based flat-panel ultrasound device for continuous intraoperative transcutaneous imaging,
J. D. Gumprecht, T. Bauer, J.-U. Stolzenburg, and T. C. Lueth, “A robotics-based flat-panel ultrasound device for continuous intraoperative transcutaneous imaging,” inEMBC. IEEE, 2011
2011
-
[14]
Dual-robot ultrasound-guided needle placement: closing the planning-imaging-action loop,
R. Kojcev, B. Fuerst, O. Zettinig, J. Fotouhi, S. C. Lee, B. Frisch, R. Taylor, E. Sinibaldi, and N. Navab, “Dual-robot ultrasound-guided needle placement: closing the planning-imaging-action loop,”Interna- tional journal of computer assisted radiology and surgery, vol. 11, no. 6, pp. 1173–1181, 2016
2016
-
[15]
Pre-trained language models for interactive decision-making,
S. Li, X. Puig, C. Paxton, Y . Du, C. Wang, L. Fan, T. Chen, D.-A. Huang, E. Aky ¨urek, A. Anandkumaret al., “Pre-trained language models for interactive decision-making,”NeurPS, 2022
2022
-
[16]
Language to rewards for robotic skill synthesis,
W. Yu, N. Gileadi, C. Fu, S. Kirmani, K.-H. Lee, M. G. Arenas, H.- T. L. Chiang, T. Erez, L. Hasenclever, J. Humpliket al., “Language to rewards for robotic skill synthesis,”arXiv preprint arXiv:2306.08647, 2023
-
[17]
Task and motion planning with large language models for object rearrangement,
Y . Ding, X. Zhang, C. Paxton, and S. Zhang, “Task and motion planning with large language models for object rearrangement,” inIROS. IEEE, 2023
2023
-
[18]
Roco: Dialectic multi-robot collabora- tion with large language models,
Z. Mandi, S. Jain, and S. Song, “Roco: Dialectic multi-robot collabora- tion with large language models,” inICRA. IEEE, 2024
2024
-
[19]
Transforming sur- gical interventions with embodied intelligence for ultrasound robotics,
H. Xu, J. Wu, G. Cao, Z. Chen, Z. Lei, and H. Liu, “Transforming sur- gical interventions with embodied intelligence for ultrasound robotics,” inMICCAI. Springer, 2024
2024
-
[20]
Uspilot: An em- bodied robotic assistant ultrasound system with a large language model enhanced graph planner,
M. Chen, S. Fan, G. Cao, Y .-h. Liu, and H. Liu, “Uspilot: An em- bodied robotic assistant ultrasound system with a large language model enhanced graph planner,”RAL, 2025
2025
-
[21]
Correcting robot plans with natural language feedback,
P. Sharma, B. Sundaralingam, V . Blukis, C. Paxton, T. Hermans, A. Torralba, J. Andreas, and D. Fox, “Correcting robot plans with natural language feedback,”arXiv preprint arXiv:2204.05186, 2022
-
[22]
C- pack: Packed resources for general chinese embeddings,
S. Xiao, Z. Liu, P. Zhang, N. Muennighoff, D. Lian, and J.-Y . Nie, “C- pack: Packed resources for general chinese embeddings,” inProceedings of the 47th international ACM SIGIR conference on research and development in information retrieval, 2024, pp. 641–649
2024
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.