A Pipeline for Generating Longitudinal Synthetic Clinical Notes Using Large Language Models
Pith reviewed 2026-06-29 04:59 UTC · model grok-4.3
The pith
A modular pipeline uses large language models to generate internally consistent longitudinal synthetic clinical notes across full patient journeys.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
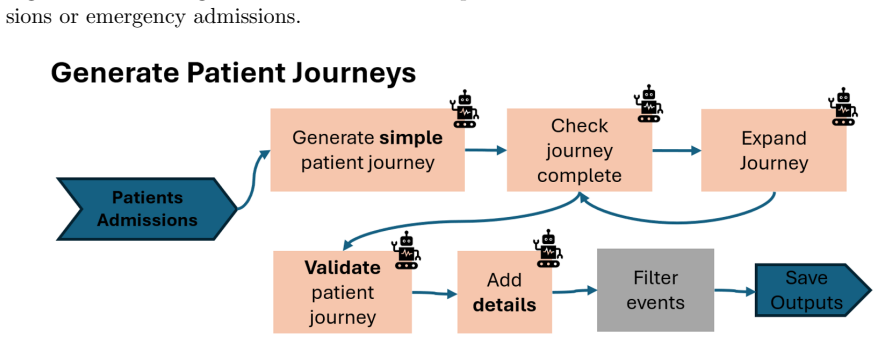
The pipeline produces internally consistent longitudinal synthetic clinical notes that capture variation in writing style, note structure, and clinical detail, enabling development of clinical AI systems without reliance on real patient data. It does this through a modular design that combines structured patient generation, semi-structured patient journey simulation, and unstructured note generation with large language models, plus additional LLM-based validation and augmentation mechanisms to improve faithfulness, realism, and diversity.
What carries the argument
The modular pipeline that links structured patient generation, semi-structured journey simulation, and LLM-driven note generation, together with separate validation and augmentation steps.
If this is right
- The released dataset of 70 patients with 20-50 notes each can be used directly to develop and evaluate summarisation tools, coding models, and decision support systems.
- Users can select different validation levels of the data to balance realism against the volume needed for their specific use case.
- The approach removes the need for real patient data, thereby avoiding associated privacy risks in clinical AI development.
- Internal consistency across longitudinal records is maintained while still allowing variation in style and clinical detail.
Where Pith is reading between the lines
- The same modular structure of patient generation followed by journey simulation and note creation could be tested in other domains that require longitudinal records, such as legal case files.
- If the pipeline's consistency mechanisms scale reliably, it might support repeated generation of larger cohorts for rare-disease or low-prevalence scenarios.
- Performance gaps between synthetic-trained and real-data-trained models could be measured on standard clinical NLP benchmarks to quantify the pipeline's practical limits.
Load-bearing premise
That the LLM generation steps plus validation and augmentation produce notes with enough faithfulness, realism, and diversity to be practically useful for training and evaluating clinical AI tools.
What would settle it
A blinded test in which clinicians rate the synthetic notes for realism and consistency against real notes, or an experiment showing whether models trained on the synthetic dataset achieve performance comparable to models trained on real clinical notes for tasks like summarization or coding.
Figures






read the original abstract
Synthetic data is increasingly used to enable the development and evaluation of AI systems in domains where access to real-world data is restricted. In healthcare, clinical documentation presents particular challenges due to its sensitivity. This work introduces a synthetic clinical notes pipeline and dataset designed to support the development of clinical AI tools while avoiding the privacy risks associated with real patient data. The dataset is generated using a modular pipeline that combines structured patient generation, semi-structured patient journey simulation, and unstructured clinical note generation using large language models. The pipeline is designed to prioritise internal consistency across longitudinal patient records, while also capturing variation in writing style, note structure, and clinical detail. Additional mechanisms, including LLM-based validation and augmentation steps, are used to improve faithfulness, realism, and diversity of the generated notes. We release a dataset of 70 synthetic patients, each associated with 20-50 clinical notes spanning a full hospital journey. The dataset is provided at multiple levels of validation, enabling users to balance realism and scalability depending on their use case. This dataset supports the development, testing, and evaluation of clinical AI systems, including summarisation tools, coding models, and decision support systems, without reliance on real patient data.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript describes a modular pipeline for generating longitudinal synthetic clinical notes using large language models. It combines structured patient generation, semi-structured patient journey simulation, and unstructured clinical note generation, augmented by LLM-based validation and augmentation steps intended to enforce internal consistency, realism, and diversity. The work releases a dataset of 70 synthetic patients, each with 20-50 notes spanning a full hospital journey, provided at multiple validation levels to support clinical AI development without real patient data.
Significance. If the pipeline's validation mechanisms demonstrably produce notes with sufficient faithfulness and longitudinal consistency, the released dataset could enable privacy-preserving development of clinical AI tools such as summarizers and coding models. The absence of any quantitative metrics, comparisons to real EHR distributions, or expert evaluations in the provided description, however, prevents assessment of whether these properties hold at scale.
major comments (1)
- [Abstract] Abstract: The claims that the pipeline produces 'internally consistent' longitudinal records that 'capture variation in writing style, note structure, and clinical detail' and that the LLM-based validation steps 'improve faithfulness, realism, and diversity' are presented without any supporting quantitative metrics, human clinician ratings, or distributional comparisons to real clinical corpora. This directly undercuts the central assertion that the notes are suitable for training and evaluating clinical AI systems.
Simulated Author's Rebuttal
We thank the referee for their review. We address the major comment below and will revise the manuscript accordingly.
read point-by-point responses
-
Referee: [Abstract] Abstract: The claims that the pipeline produces 'internally consistent' longitudinal records that 'capture variation in writing style, note structure, and clinical detail' and that the LLM-based validation steps 'improve faithfulness, realism, and diversity' are presented without any supporting quantitative metrics, human clinician ratings, or distributional comparisons to real clinical corpora. This directly undercuts the central assertion that the notes are suitable for training and evaluating clinical AI systems.
Authors: We agree that the abstract asserts these properties without quantitative support, metrics, ratings, or distributional comparisons. The manuscript describes the pipeline's modular design and validation mechanisms as intended to achieve internal consistency, stylistic variation, and improved faithfulness/realism/diversity, but does not include empirical evaluations of these outcomes. In revision we will edit the abstract to frame these as design goals of the pipeline rather than demonstrated results, and we will add a limitations section explicitly noting the lack of such quantitative validation or real-EHR comparisons. This will align the claims with the paper's actual scope as a pipeline and dataset release. revision: yes
Circularity Check
No circularity: descriptive engineering pipeline with no derivations or self-referential reductions
full rationale
The paper describes a modular pipeline for synthetic note generation using LLMs, structured patient simulation, and validation steps. No equations, fitted parameters, predictions, or uniqueness theorems appear. Claims rest on pipeline design choices and released data rather than any reduction of outputs to inputs by construction. No self-citation load-bearing steps or ansatz smuggling are present. The work is self-contained as an engineering contribution without mathematical derivation chains.
Axiom & Free-Parameter Ledger
axioms (1)
- domain assumption LLMs can generate realistic and consistent clinical notes when guided by structured patient data and validation steps
Reference graph
Works this paper leans on
-
[1]
Robust de-anonymization of large sparse datasets
Arvind Narayanan and Vitaly Shmatikov. Robust de-anonymization of large sparse datasets. In2008 IEEE Symposium on Security and Privacy (SP 2008), pages 111–125. IEEE, 2008
2008
-
[2]
Synthetic data generation: State of the art in health care domain.Computer Science Review, 48:100546, 2023
Hajra Murtaza, Musharif Ahmed, Naurin Farooq Khan, Ghulam Murtaza, Saad Zafar, and Ambreen Bano. Synthetic data generation: State of the art in health care domain.Computer Science Review, 48:100546, 2023
2023
-
[3]
Pezoulas, Dimitrios I
Vasileios C. Pezoulas, Dimitrios I. Zaridis, Eugenia Mylona, Christos Androutsos, Kosmas Apostolidis, Nikolaos S. Tachos, and Dimitrios I. Fotiadis. Synthetic data generation methods in healthcare: A review on open-source tools and methods.Computational and Structural Biotechnology Journal, 23:2892–2910, 2024
2024
-
[4]
Olatunji, Jens Rauch, Matthias Katzensteiner, and Megha Khosla
Iyiola E. Olatunji, Jens Rauch, Matthias Katzensteiner, and Megha Khosla. A review of anonymization for healthcare data.CoRR, abs/2104.06523, 2021
-
[5]
Artificial data pilot, 2025
NHS England Digital. Artificial data pilot, 2025. Accessed: 2026-05-13
2025
-
[6]
Synthea: Synthetic patient population simulator, 2026
The MITRE Corporation. Synthea: Synthetic patient population simulator, 2026. Accessed: 2026-05-13
2026
-
[7]
Agent hospital: A simulacrum of hospital with evolvable medical agents, 2025
Junkai Li, Yunghwei Lai, Weitao Li, Jingyi Ren, Meng Zhang, Xinhui Kang, Siyu Wang, Peng Li, Ya-Qin Zhang, Weizhi Ma, and Yang Liu. Agent hospital: A simulacrum of hospital with evolvable medical agents, 2025
2025
-
[8]
Sdv (synthetic data vault) developer documentation, 2026
DataCebo. Sdv (synthetic data vault) developer documentation, 2026. Accessed: 2026-05-13
2026
-
[9]
Swpc synthea: Uk adaptation of the synthea synthetic patient generator, 2026
NHS England. Swpc synthea: Uk adaptation of the synthea synthetic patient generator, 2026. Accessed: 2026-05-13. 16
2026
-
[10]
Springer Nature Switzerland, 2024
Gleb Kumichev, Pavel Blinov, Yulia Kuzkina, Vasily Goncharov, Galina Zubkova, Nikolai Zenovkin, Aleksei Goncharov, and Andrey Savchenko.MedSyn: LLM-Based Synthetic Medical Text Generation Framework, page 215–230. Springer Nature Switzerland, 2024
2024
-
[11]
A comprehensive taxonomy of hallucinations in large language models, 2025
Manuel Cossio. A comprehensive taxonomy of hallucinations in large language models, 2025
2025
-
[12]
Medical hallucination in foundation models and their impact on healthcare.medRxiv, 2025
Yubin Kim, Hyewon Jeong, Shan Chen, Shuyue Stella Li, Mingyu Lu, Kumail Alhamoud, Jimin Mun, Cristina Grau, Minseok Jung, Rodrigo Gameiro, Lizhou Fan, Eugene Park, Tristan Lin, Joonsik Yoon, Wonjin Yoon, Maarten Sap, Yulia Tsvetkov, Paul Liang, Xuhai Xu, Xin Liu, Daniel McDuff, Hyeonhoon Lee, Hae Won Park, Samir Tulebaev, and Cynthia Breazeal. Medical hal...
2025
-
[13]
Khaled Saab, Tao Tu, Wei-Hung Weng, Ryutaro Tanno, David Stutz, Ellery Wulczyn, Fan Zhang, Tim Strother, Chunjong Park, Elahe Vedadi, Juanma Zambrano Chaves, Szu-Yeu Hu, Mike Schaekermann, Aishwarya Kamath, Yong Cheng, David G. T. Barrett, Cathy Cheung, Basil Mustafa, Anil Palepu, Daniel McDuff, Le Hou, Tomer Golany, Luyang Liu, Jean baptiste Alayrac, Nei...
2024
-
[14]
Smith, Nima PourNejatian, Anthony B
Cheng Peng, Xi Yang, Aokun Chen, Kaleb E. Smith, Nima PourNejatian, Anthony B. Costa, Cheryl Martin, Mona G. Flores, Ying Zhang, Tanja Magoc, Gloria Lipori, Duane A. Mitchell, Naykky S. Ospina, Mustafa M. Ahmed, William R. Hogan, Elizabeth A. Shenkman, Yi Guo, Jiang Bian, and Yonghui Wu. A study of generative large language model for medical research and ...
2023
-
[15]
Chain-of-thought prompting elicits reasoning in large language models, 2023
Jason Wei, Xuezhi Wang, Dale Schuurmans, Maarten Bosma, Brian Ichter, Fei Xia, Ed Chi, Quoc Le, and Denny Zhou. Chain-of-thought prompting elicits reasoning in large language models, 2023
2023
- [16]
-
[17]
A survey of large language models for healthcare: from data, technology, and applications to accountability and ethics.Information Fusion, 118:102963, 2025
Kai He, Rui Mao, Qika Lin, Yucheng Ruan, Xiang Lan, Mengling Feng, and Erik Cambria. A survey of large language models for healthcare: from data, technology, and applications to accountability and ethics.Information Fusion, 118:102963, 2025
2025
-
[18]
Benchmarking retrieval-augmented generation for medicine, 2024
Guangzhi Xiong, Qiao Jin, Zhiyong Lu, and Aidong Zhang. Benchmarking retrieval-augmented generation for medicine, 2024. 17
2024
-
[19]
Reasoning-enhanced healthcare predictions with knowledge graph community retrieval, 2025
Pengcheng Jiang, Cao Xiao, Minhao Jiang, Parminder Bhatia, Taha Kass-Hout, Jimeng Sun, and Jiawei Han. Reasoning-enhanced healthcare predictions with knowledge graph community retrieval, 2025
2025
-
[20]
A survey on llm-as-a-judge, 2025
Jiawei Gu, Xuhui Jiang, Zhichao Shi, Hexiang Tan, Xuehao Zhai, Chengjin Xu, Wei Li, Yinghan Shen, Shengjie Ma, Honghao Liu, Saizhuo Wang, Kun Zhang, Yuanzhuo Wang, Wen Gao, Lionel Ni, and Jian Guo. A survey on llm-as-a-judge, 2025
2025
-
[21]
Justice or prejudice? quantifying biases in llm-as-a-judge, 2024
Jiayi Ye, Yanbo Wang, Yue Huang, Dongping Chen, Qihui Zhang, Nuno Moniz, Tian Gao, Werner Geyer, Chao Huang, Pin-Yu Chen, Nitesh V Chawla, and Xiangliang Zhang. Justice or prejudice? quantifying biases in llm-as-a-judge, 2024
2024
-
[22]
typo: A python package to simulate typographical errors, 2023
Ranvijay Kumar. typo: A python package to simulate typographical errors, 2023. Version 0.1.7. Accessed: 2026-05-13
2023
-
[23]
Evaluating gender bias in large language models in long-term care.BMC Medical Informatics and Decision Making, 25(1):274, 2025
Sam Rickman. Evaluating gender bias in large language models in long-term care.BMC Medical Informatics and Decision Making, 25(1):274, 2025. Published: 2025-08-11. 18
2025
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.