Incorporating vaccine effects into epidemiological models: common pitfalls and solutions
Pith reviewed 2026-05-20 01:25 UTC · model grok-4.3
The pith
Directly incorporating empirical vaccine effectiveness estimates into models underestimates the population impact of leaky vaccines.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
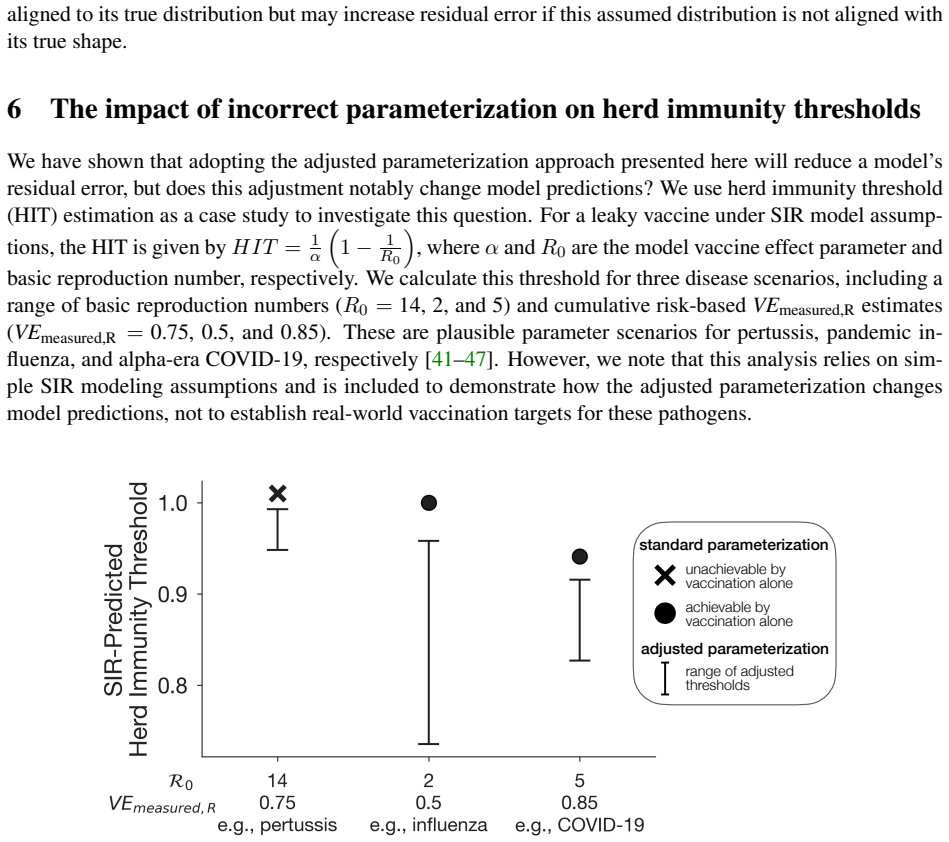
To accurately parameterize epidemiological models with vaccine protection, both the vaccine's mechanism of action and the statistic used to infer vaccine efficacy from data must be considered. For leaky vaccines, common empirical estimation methods do not yield directly applicable parameter values. Naive incorporation of these estimates underestimates population-level vaccine impact. The proposed adjusted parameterization aligns the modeled effect with empirical data, leading to predictions of fewer total infections and lower herd immunity thresholds for leaky vaccines.
What carries the argument
An adjusted parameterization approach that accounts for the mismatch between empirical vaccine efficacy statistics and model protection parameters for leaky vaccines.
If this is right
- Models with adjusted parameters predict fewer total infections compared to naive approaches.
- Lower herd immunity thresholds are estimated for leaky vaccines under the adjusted method.
- This leads to more accurate assessments of vaccine impact in public health planning.
- Decision making for vaccination strategies benefits from reduced bias in impact estimates.
Where Pith is reading between the lines
- Similar mismatches could exist in models of other partial interventions such as partial quarantine or treatment effects.
- Empirical studies might benefit from estimating VE in ways that directly match common model structures.
- Applying this adjustment could revise current estimates of required vaccination coverage for disease control.
Load-bearing premise
The vaccine mechanism is leaky protection, meaning it partially reduces individual infection risk, and the empirical VE statistic does not directly correspond to the model's protection parameter.
What would settle it
Comparing model predictions of total infections or the vaccination coverage needed for herd immunity using naive versus adjusted parameters against observed data from a real-world vaccination program for a leaky vaccine.
Figures





read the original abstract
Incorporating vaccination into mathematical models appears deceptively simple: models integrate vaccine-derived protections, such as reduced susceptibility to infection, using parameters informed by empirical estimates of vaccine efficacy or effectiveness (VE). In practice, however, empirical VE estimates often do not correspond directly to the parameters of epidemiological models. Here, we extend previous work to demonstrate that in order to accurately parameterize a model, one must consider both a vaccine's mechanism of action and the statistic used to infer VE from empirical data. When a vaccine confers leaky protection -- that is, vaccination partially rather than completely reduces individual infection risk -- we show that common empirical VE estimation methods do not provide directly applicable values for model parameters. Naive (i.e. direct) incorporation of these VE estimates into models results in an underestimate of population-level vaccine impact. To make progress when these estimates are the only available sources for VE, we introduce a parameterization approach which more accurately aligns the modeled effect of vaccination with empirical estimates. Under this adjusted parameterization approach, models predict fewer total infections and lower herd immunity thresholds for leaky vaccines than would be predicted under current parameterization practices. Our parameterization guidelines and adjustment approach can be used to improve accuracy in models that are used in vaccine decision making and public health planning.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript argues that empirical estimates of vaccine efficacy (VE) for leaky vaccines, which confer partial rather than complete protection, do not map directly onto the susceptibility-reduction parameters used in standard compartmental epidemiological models. Direct (naive) insertion of these VE values into models produces an underestimate of population-level vaccine impact. The authors derive and present an adjusted parameterization that corrects for the mismatch between the empirical statistic and the model parameter, yielding predictions of fewer total infections and lower herd-immunity thresholds than current practice.
Significance. If the central adjustment holds, the work would improve the fidelity of models that inform vaccine policy and public-health planning. It supplies concrete parameterization guidelines and demonstrates the directional bias that arises from the mismatch, thereby offering a practical correction that could alter quantitative conclusions about vaccine impact for partially effective products.
major comments (2)
- [§3.2] §3.2 (or equivalent section on empirical estimators): The mismatch and resulting underestimate are demonstrated for direct risk-ratio estimators, but the manuscript does not examine whether the same systematic discrepancy arises when VE is obtained from Cox proportional-hazards or Poisson regression models with time-varying hazards—the estimators most frequently reported in the VE literature. Because the direction and magnitude of the proposed correction rest on this mismatch, the generality of the adjustment requires explicit verification across these standard procedures.
- [§4] §4, derivation of the adjusted susceptibility parameter: The adjustment formula is presented under the assumption of a constant leaky protection mechanism; it is not shown whether the same closed-form correction remains valid when protection wanes, when there is heterogeneity in individual response, or when the model includes age structure or contact networks. These extensions are load-bearing for the claim that the adjusted parameterization should be adopted in routine modeling practice.
minor comments (2)
- Notation for the leaky protection parameter (e.g., the multiplier on susceptibility) is introduced without a clear side-by-side comparison to the empirical VE statistic; a small table or equation block making the distinction explicit would improve readability.
- [Results] The numerical examples in the results section would benefit from reporting both the naive and adjusted predictions on the same axes (or in a single table) so that the magnitude of the difference is immediately visible to readers.
Simulated Author's Rebuttal
We thank the referee for their insightful comments on our manuscript. We address each of the major comments below and outline the revisions we will make to improve the clarity and generality of our findings.
read point-by-point responses
-
Referee: [§3.2] §3.2 (or equivalent section on empirical estimators): The mismatch and resulting underestimate are demonstrated for direct risk-ratio estimators, but the manuscript does not examine whether the same systematic discrepancy arises when VE is obtained from Cox proportional-hazards or Poisson regression models with time-varying hazards—the estimators most frequently reported in the VE literature. Because the direction and magnitude of the proposed correction rest on this mismatch, the generality of the adjustment requires explicit verification across these standard procedures.
Authors: We acknowledge that our primary demonstrations in §3.2 use direct risk-ratio estimators for simplicity and to illustrate the core mismatch. However, the adjustment arises from the fundamental difference between the empirical VE (which measures relative reduction in infection probability or rate) and the model parameter (which scales the force of infection for vaccinated individuals in a leaky manner). For Cox proportional-hazards models, the estimated hazard ratio under proportional hazards directly informs the susceptibility reduction, but when embedded in a dynamic model, the population-level impact still requires the same correction to avoid underestimating vaccine effects. Similarly for Poisson regression. We will add an appendix with analytical arguments and numerical simulations confirming that the adjustment applies equivalently to these estimators, thereby strengthening the generality of our recommendations. revision: yes
-
Referee: [§4] §4, derivation of the adjusted susceptibility parameter: The adjustment formula is presented under the assumption of a constant leaky protection mechanism; it is not shown whether the same closed-form correction remains valid when protection wanes, when there is heterogeneity in individual response, or when the model includes age structure or contact networks. These extensions are load-bearing for the claim that the adjusted parameterization should be adopted in routine modeling practice.
Authors: The derivation in §4 is indeed for a basic model with constant leaky protection. We agree that demonstrating validity under waning immunity, response heterogeneity, age structure, or network contacts would further support broad adoption. The core adjustment corrects for the fact that empirical VE reflects an average effect that interacts with the nonlinear dynamics of transmission. In extensions, the same logic applies by adjusting the instantaneous susceptibility parameter at each time or for each subgroup. We will revise §4 and add a discussion section addressing these cases, providing guidance on how to apply the adjustment in more complex models without claiming a single closed-form for all scenarios. This addresses the load-bearing concern by clarifying the scope and providing a pathway for extensions. revision: partial
Circularity Check
No significant circularity; derivation self-contained
full rationale
The paper identifies an external mismatch between common empirical VE estimation procedures (e.g., risk-ratio based) and the protection parameters required by leaky-vaccine models, then proposes an adjusted parameterization to align them. This mismatch is demonstrated by comparing the statistic used in data inference against the model's susceptibility multiplier, without any reduction of the central claim to quantities defined inside the model by construction. No fitted inputs are relabeled as predictions, no uniqueness theorem is imported from self-citation, and the adjustment is presented as a guideline rather than a renaming of known results. The derivation relies on external benchmarks of VE methods and remains independent of any self-referential loop.
Axiom & Free-Parameter Ledger
axioms (1)
- domain assumption Vaccine confers leaky protection rather than all-or-nothing protection
Reference graph
Works this paper leans on
-
[1]
Immunization coverage.https://www.who.int/news-room/ fact-sheets/detail/immunization-coverage, 2024
World Health Organization. Immunization coverage.https://www.who.int/news-room/ fact-sheets/detail/immunization-coverage, 2024. Accessed: 2026-04-22
work page 2024
-
[2]
Bubar, Kyle Reinholt, Stephen M
Kate M. Bubar, Kyle Reinholt, Stephen M. Kissler, Marc Lipsitch, Sarah Cobey, Yonatan H. Grad, and Daniel B. Larremore. Model-informed COVID-19 vaccine prioritization strategies by age and serostatus.Science, 371(6532):916–921, feb 2021
work page 2021
-
[3]
Sam Moore, Edward M. Hill, Louise Dyson, Michael J. Tildesley, and Matt J. Keeling. Modelling opti- mal vaccination strategy for SARS-CoV-2 in the UK.PLOS Computational Biology, 17(5):e1008849, may 2021
work page 2021
-
[4]
Eva Kisdi. Optimal vaccination strategies for imperfect vaccines and variable host susceptibility.Jour- nal of Theoretical Biology, 594:111899, nov 2024
work page 2024
-
[5]
Al V . Taira, Christopher P. Neukermans, and Gillian D. Sanders. Evaluating human papillomavirus vaccination programs.Emerging Infectious Diseases, 10(11):1915–1923, 2004
work page 1915
-
[6]
Elamin H. Elbasha, Erik J. Dasbach, and Ralph P. Insinga. Model for assessing human papillomavirus vaccination strategies.Emerging Infectious Diseases, 13(1):28–41, 2007
work page 2007
-
[7]
R.M. Anderson and R.M. May. Vaccination against rubella and measles: quantitative investigations of different policies.Epidemiology & Infection, 90(2), 1983
work page 1983
-
[8]
Sam Moore, Edward M. Hill, Michael J. Tildesley, Louise Dyson, and Matt J. Keeling. Vaccination and non-pharmaceutical interventions for COVID-19: a mathematical modelling study.The Lancet Infectious Diseases, 21(6):793–802, june 2021
work page 2021
-
[9]
Kate M. Bubar, Casey E. Middleton, Kristen K. Bjorkman, Roy Parker, and Daniel B. Larremore. SARS-CoV-2 transmission and impacts of unvaccinated-only screening in populations of mixed vac- cination status.Nature Communications, 13(11):2777, may 2022
work page 2022
-
[10]
The theory of measles elimination: implications for the design of elimination strategies
Nigel J Gay. The theory of measles elimination: implications for the design of elimination strategies. The Journal of Infectious Diseases, 189(Supplement 1):S27–S35, 2004
work page 2004
-
[11]
J. Mossong and C. P. Muller. Estimation of the basic reproduction number of measles during an outbreak in a partially vaccinated population.Epidemiology & Infection, 124(2):273–278, 2000
work page 2000
-
[12]
Mathew V . Kiang, Kate M. Bubar, Yvonne Maldonado, Peter J. Hotez, and Nathan C. Lo. Modeling reemergence of vaccine-eliminated infectious diseases under declining vaccination in the US.JAMA, 333(24):2176, june 2025
work page 2025
-
[13]
Derek Weycker, John Edelsberg, M. Elizabeth Halloran, Ira M. Longini, Azhar Nizam, Vincent Ciuryla, and Gerry Oster. Population-wide benefits of routine vaccination of children against influenza. Vaccine, 23(10):1284–1293, 2005
work page 2005
-
[14]
Christina Atchison, Ben Lopman, and William John Edmunds. Modelling the seasonality of rotavirus disease and the impact of vaccination in England and Wales.Vaccine, 28(18):3118–3126, 2010
work page 2010
-
[15]
Marc Lipsitch. Vaccination against colonizing bacteria with multiple serotypes.Proceedings of the National Academy of Sciences, 94(12):6571–6576, 1997. 14
work page 1997
-
[16]
Frank Sandmann, Mark Jit, Nick Andrews, Hannah L. Buckley, Helen Campbell, Sonia Ribeiro, Bersabeh Sile, Julia Stowe, Elise Tessier, Mary Ramsay, Gayatri Amirthalingam, and Yoon H. Choi. Evaluating the impact of a continued maternal pertussis immunisation programme in England: A mod- elling study and cost-effectiveness analysis.Vaccine, 39(32):4500–4509, 2021
work page 2021
- [17]
-
[18]
M. Gabriela M. Gomes, Marc Lipsitch, Andrew R. Wargo, Gael Kurath, Carlota Rebelo, Graham F. Medley, and Antonio Coutinho. A missing dimension in measures of vaccination impacts.PLOS Pathogens, 10(3):e1003849, mar 2014
work page 2014
-
[19]
Ariel Nikas, Hasan Ahmed, and Veronika I. Zarnitsyna. Competing heterogeneities in vaccine effec- tiveness estimation.Vaccines, 11(8), july 2023
work page 2023
-
[20]
Kate E. Langwig, Andrew R. Wargo, Darbi R. Jones, Jessie R. Viss, Barbara J. Rutan, et al. Vaccine effects on heterogeneity in susceptibility and implications for population health management.mBio, 8(6):e00796–17, nov 2017
work page 2017
-
[21]
M. E. Halloran, M. Haber, and I. M. Longini. Interpretation and estimation of vaccine efficacy under heterogeneity.American Journal of Epidemiology, 136(3):328–343, aug 1992
work page 1992
-
[22]
M. E. Halloran, C. J. Struchiner, and I. M. Longini. Study designs for evaluating different efficacy and effectiveness aspects of vaccines.American Journal of Epidemiology, 146(10):789–803, nov 1997
work page 1997
-
[23]
Eunha Shim and Alison P. Galvani. Distinguishing vaccine efficacy and effectiveness.Vaccine, 30(47):6700–6705, oct 2012
work page 2012
-
[24]
Mammen, Gyan Ba- hadur Thapa, et al
Mrigendra Prasad Shrestha, Robert McNair Scott, Durga Man Joshi, Mammen P. Mammen, Gyan Ba- hadur Thapa, et al. Safety and efficacy of a recombinant hepatitis E vaccine.New England Journal of Medicine, 356(9):895–903, mar 2007
work page 2007
-
[25]
Fernando P. Polack, Stephen J. Thomas, Nicholas Kitchin, Judith Absalon, Alejandra Gurtman, et al. Safety and efficacy of the BNT162b2 mRNA COVID-19 vaccine.New England Journal of Medicine, 383(27):2603–2615, dec 2020
work page 2020
-
[26]
Paul T. Heath, Eva P. Galiza, David N. Baxter, Marta Boffito, Duncan Browne, et al. Safety and efficacy of NVX-CoV2373 COVID-19 vaccine.New England Journal of Medicine, 385(13):1172–1183, sept 2021
work page 2021
-
[27]
Michael L. Jackson, Jessie R. Chung, Lisa A. Jackson, C. Hallie Phillips, Joyce Benoit, et al. Influenza vaccine effectiveness in the United States during the 2015–2016 season.New England Journal of Medicine, 377(6):534–543, aug 2017
work page 2015
-
[28]
Jamie Lopez Bernal, Nick Andrews, Charlotte Gower, Eileen Gallagher, Ruth Simmons, Simon Thel- wall, Julia Stowe, Elise Tessier, Natalie Groves, et al. Effectiveness of COVID-19 vaccines against the B.1.617.2 (delta) variant.New England Journal of Medicine, 385(7), 2021
work page 2021
-
[29]
Chandra J. Cohen-Stavi, Ori Magen, Noam Barda, Shlomit Yaron, Alon Peretz, Doron Netzer, Carlo Giaquinto, Ali Judd, Leonard Leibovici, Miguel A. Hern ´an, Marc Lipsitch, Ben Y . Reis, Ran D. Bal- 15 icer, and Noa Dagan. BNT162b2 vaccine effectiveness against omicron in children 5 to 11 years of age.New England Journal of Medicine, 387(3):227–236, july 2022
work page 2022
-
[30]
Suzanne E. Ohmit, Joshua G. Petrie, Ryan E. Malosh, Benjamin J. Cowling, Mark G. Thompson, David K. Shay, and Arnold S. Monto. Influenza vaccine effectiveness in the community and the household.Clinical Infectious Diseases, 56:1363–1369, 2013
work page 2013
-
[31]
Mie Agermose Gram, Hanne-Dorthe Emborg, Astrid Blicher Schelde, Nikolaj Ulrik Friis, Ka- trine Finderup Nielsen, et al. Vaccine effectiveness against SARS-CoV-2 infection or COVID-19 hospitalization with the alpha, delta, or omicron SARS-CoV-2 variant: A nationwide Danish cohort study.PLOS Medicine, 19(9):e1003992, sept 2022
work page 2022
-
[32]
Joseph A Lewnard, Christine Tedijanto, Benjamin J Cowling, and Marc Lipsitch. Measure- ment of vaccine direct effects under the test-negative design.American Journal of Epidemiology, 187(12):2686–2697, 2018
work page 2018
-
[33]
Rebecca Kahn, Matt Hitchings, Rui Wang, Steven E Bellan, and Marc Lipsitch. Analyzing vac- cine trials in epidemics with mild and asymptomatic infection.American Journal of Epidemiology, 188(2):467–474, feb 2019
work page 2019
-
[34]
Rebecca Kahn, Stephanie J. Schrag, Jennifer R. Verani, and Marc Lipsitch. Identifying and alleviating bias due to differential depletion of susceptible people in postmarketing evaluations of COVID-19 vaccines.American Journal of Epidemiology, 191(5):800–811, 2022
work page 2022
-
[35]
Edward Goldstein, Virginia E. Pitzer, Justin J. O’Hagan, and Marc Lipsitch. Temporally vary- ing relative risks for infectious diseases: Implications for infectious disease control.Epidemiology, 28(1):136–144, jan 2017
work page 2017
-
[36]
Keeling and Pejman Rohani.Modeling Infectious Diseases in Humans and Animals
Matthew J. Keeling and Pejman Rohani.Modeling Infectious Diseases in Humans and Animals. Princeton University Press, Princeton, NJ, 2008
work page 2008
-
[37]
Eben Kenah, Marc Lipsitch, and James M. Robins. Generation interval contraction and epidemic data analysis.Mathematical Biosciences, 213(1):71–79, may 2008
work page 2008
-
[38]
N. Hens, M. Aerts, C. Faes, Z. Shkedy, O. Lejeune, P. Van Damme, and P. Beutels. Seventy- five years of estimating the force of infection from current status data.Epidemiology & Infection, 138(6):802–812, june 2010
work page 2010
-
[39]
Da In Lee, Anjalika Nande, Thayer L. Anderson, Michael Z. Levy, and Alison L. Hill. Vaccine failure mode determines population-level impact of vaccination campaigns during epidemics.Journal of The Royal Society Interface, 22(223):20240689, feb 2025
work page 2025
- [40]
- [41]
-
[42]
Helen J. Wearing and Pejman Rohani. Estimating the duration of pertussis immunity using epidemio- logical signatures.PLOS Pathogens, 5(10):e1000647, oct 2009. 16
work page 2009
-
[43]
Matthew Biggerstaff, Simon Cauchemez, Carrie Reed, Manoj Gambhir, and Lyn Finelli. Estimates of the reproduction number for seasonal, pandemic, and zoonotic influenza: a systematic review of the literature.BMC Infectious Diseases, 14(1):480, 2014
work page 2014
-
[44]
Michael T. Osterholm, Nicholas S. Kelley, Anne Sommer, and Edward P. Knighton. Efficacy and effectiveness of influenza vaccines: a systematic review and meta-analysis.The Lancet Infectious Diseases, 12(1):36–44, 2012
work page 2012
-
[45]
Ying Liu and Joacim Rockl ¨ov. The effective reproductive number of the omicron variant of SARS- CoV-2 is several times relative to delta.Journal of Travel Medicine, 29(3):taac037, 2022
work page 2022
-
[46]
Durability of 2024-2025 COVID-19 vaccines against JN.1 subvariants.JAMA Internal Medicine, 2025
Danyu Lin et al. Durability of 2024-2025 COVID-19 vaccines against JN.1 subvariants.JAMA Internal Medicine, 2025
work page 2024
-
[47]
Ruth Link-Gelles, Sean Chickery, Alexander Webber, Toan C. Ong, Elizabeth A.K. Rowley, et al. Interim estimates of 2024–2025 COVID-19 vaccine effectiveness among adults aged over 18 years — VISION and IVY networks, September 2024–January 2025.MMWR. Morbidity and Mortality Weekly Report, 74:73–82, 2025
work page 2024
-
[48]
Romain Ragonnet, James M. Trauer, Justin T. Denholm, Nicholas L. Geard, Margaret Hellard, and Emma S. McBryde. Vaccination programs for endemic infections: Modelling real versus apparent impacts of vaccine and infection characteristics.Scientific Reports, 5(1):15468, oct 2015
work page 2015
-
[49]
Michael Haber, Walter A. Orenstein, M. Elizabeth Halloran, and Ira M. Longini. The effect of disease prior to an outbreak on estimates of vaccine efficacy following the outbreak.American Journal of Epidemiology, 141(10):980–990, may 1995
work page 1995
-
[50]
James Wood, James McCaw, Niels Becker, Terry Nolan, and C. Raina MacIntyre. Optimal dosing and dynamic distribution of vaccines in an influenza pandemic.American Journal of Epidemiology, 169(12):1517–1524, june 2009
work page 2009
-
[51]
Epiengage: Measles decision support tool.https:// epiengage-measles.tacc.utexas.edu/, 2026
The University of Texas at Austin. Epiengage: Measles decision support tool.https:// epiengage-measles.tacc.utexas.edu/, 2026. Accessed: 2026-03-25
work page 2026
-
[52]
Paul T. Edlefsen. Leaky vaccines protect highly exposed recipients at a lower rate: Implications for vaccine efficacy estimation and sieve analysis.Computational and Mathematical Methods in Medicine, 2014:813789, 2014. 17 Supplemental Materials S1 Materials and Methods S1.1 CalculatingVEfrom a Bernoulli infection model To clearly demonstrate the drivers o...
work page 2014
-
[53]
and has a class-specificαofα k. The vaccinated population is thus divided into3Kcompartments {VS,k, V I,k , V R,k}, and the unvaccinated compartments{S, I, R}follow the same equations as before. The force of infection is λ(t) = β I(t) +PK k=1 VI,k(t) N ,(S20) 22 and the dynamics within each vaccinated stratum are dVS,k dt =−(1−α k)λ V S,k,(S21) dVI,k dt =...
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.