AI-driven Optimisation of Quality of Recovery (QoR) in Remote Patient Monitoring
Pith reviewed 2026-06-26 08:17 UTC · model grok-4.3
The pith
A five-item subset of the QoR-15 predicts recovery severity as accurately as the full survey.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
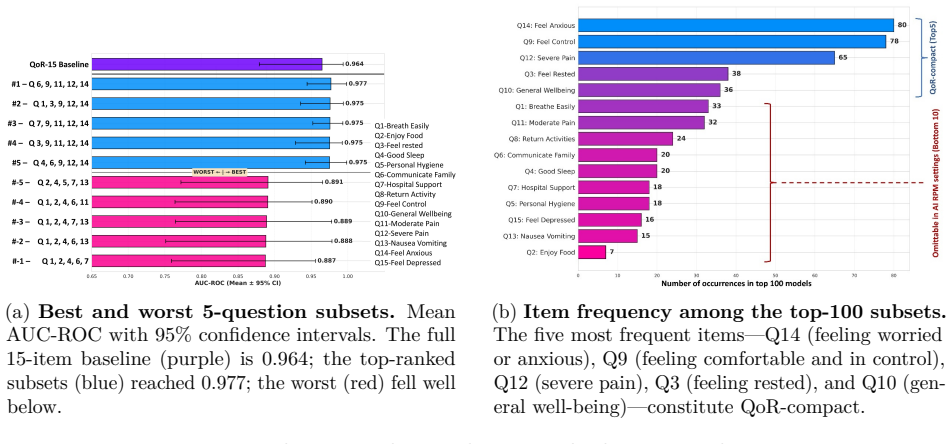
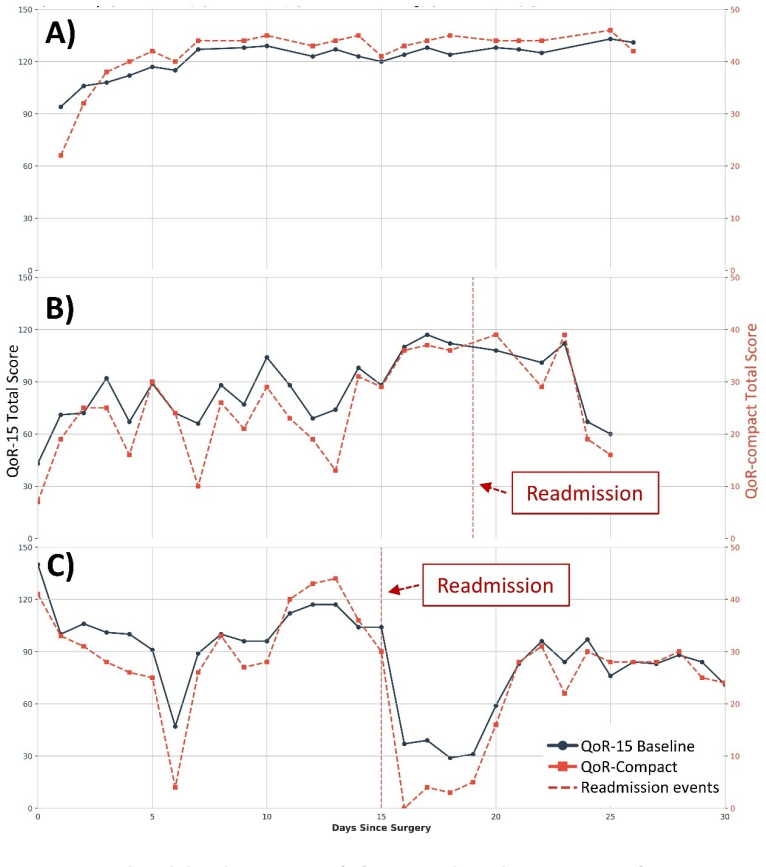
QoR-compact, identified by evaluating all possible five-item subsets of the QoR-15, achieves a mean AUC-ROC of 0.968 (95% CI 0.915-0.988) in predicting recovery severity, statistically comparable to the 0.964 baseline from one-third of the items, and tracks readmission events similarly in patient-level backtesting.
What carries the argument
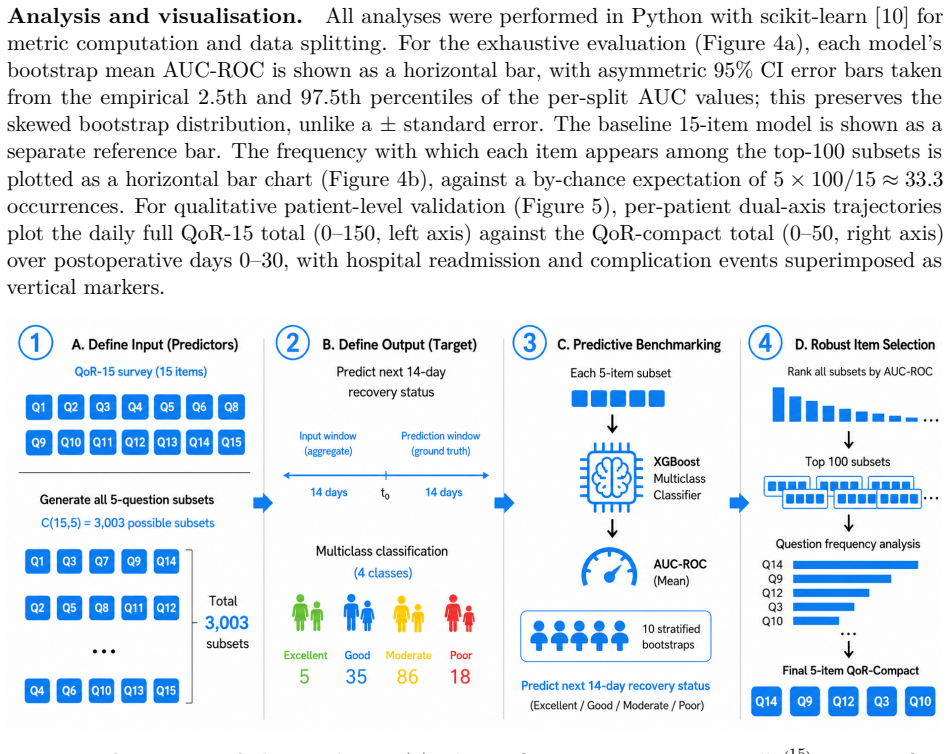
Exhaustive search over all 3,003 possible five-question subsets of the QoR-15 to select the subset that best matches the full instrument's predictive performance for postoperative recovery severity.
If this is right
- QoR-compact provides a shorter daily input that maintains predictive parity with the full QoR-15 for remote monitoring.
- The five items span physical and psychological recovery axes.
- Patient-level tracking of readmission events remains faithful to the full form.
- This parity supports testing whether lighter input increases daily completion rates.
Where Pith is reading between the lines
- Completion rates in daily remote monitoring may rise with fewer items per day.
- External validation across different surgical cohorts and settings is needed to confirm generalizability.
- The exhaustive subset search method could apply to other multi-item patient-reported outcome measures.
Load-bearing premise
The five-item subset selected from one post-surgical deployment cohort will perform equally well in other patient populations and in ongoing daily remote monitoring.
What would settle it
Measuring the AUC-ROC of QoR-compact on an independent cohort of patients from a different hospital or surgical type and finding it significantly below the full survey's performance.
Figures
read the original abstract
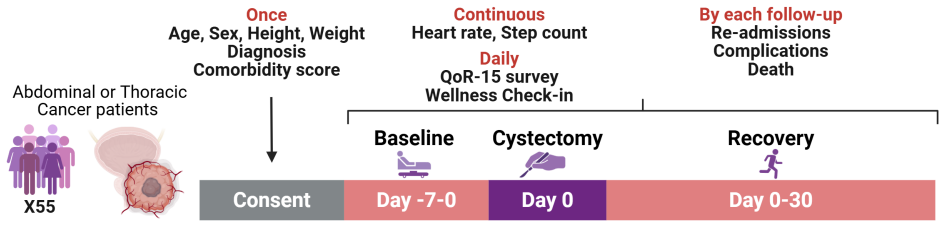
Remote patient monitoring depends on patient-reported data to capture the subjective dimension of recovery that devices cannot measure. The Quality of Recovery (QoR-15) survey is the gold-standard instrument for this purpose. It was designed and validated for occasional in-hospital assessment, yet remote monitoring now administers it to patients daily. In our own post-surgical deployment, only 55% of patients submitted the survey more than 14 days of 30 monitoring days. We developed QoR-compact, a five-item daily input for the RPM prediction pathway. Setting a deployment-driven target of one-third of the daily items, we exhaustively evaluated all 3,003 five-question subsets of the QoR-15 and tested whether the best of them matches the full instrument in predicting near-term postoperative recovery severity. QoR-compact achieves a mean AUC-ROC of 0.968 (95% CI 0.915-0.988), statistically comparable to the 0.964 baseline obtained with one-third of the items. Patient-level backtesting indicates that it tracks readmission events as faithfully as the full form. Its five items span the physical and psychological axes of recovery: Q3 (feeling rested), Q9 (feeling comfortable and in control), Q10 (general well-being), Q12 (severe pain), and Q14 (feeling worried or anxious). The QoR-15 remains the gold-standard measure of recovery; QoR-compact complements it as a shorter daily input designed for prediction. This parity provides the basis for a prospective study of whether a lighter daily input is, in turn, completed more consistently. External validation on larger cohorts is required before clinical use.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript claims that exhaustive enumeration of all 3,003 five-item subsets of the QoR-15 on a single post-surgical remote-monitoring deployment cohort yields a compact instrument (items Q3, Q9, Q10, Q12, Q14) whose AUC-ROC of 0.968 (95% CI 0.915-0.988) for predicting near-term recovery severity is statistically comparable to the 0.964 value obtained with one-third of the items; patient-level backtesting further indicates equivalent tracking of readmission events. The work positions QoR-compact as a lower-burden daily input that complements the full QoR-15 while preserving predictive utility.
Significance. If externally validated, the result would supply a practical, deployment-derived route to reducing daily patient burden from 15 to 5 items in remote monitoring without apparent loss of predictive signal for recovery severity, directly addressing the reported 55% compliance rate beyond 14 days. The transparent enumeration of all subsets and the explicit call for prospective studies on completion rates constitute concrete, falsifiable next steps.
major comments (2)
- [Abstract] Abstract: the reported AUC-ROC parity (0.968 vs 0.964) and the claim that the selected five-item subset 'tracks readmission events as faithfully as the full form' rest on exhaustive subset selection followed by performance evaluation on the identical internal cohort, with no description of nested cross-validation, pre-specified hold-out, or external test set; this selection procedure is load-bearing for the generalization claim to prospective daily RPM use.
- [Abstract] Abstract: the manuscript supplies no cohort size, patient demographics, handling of missing data, or statistical test used to declare the two AUC values 'statistically comparable'; these omissions prevent assessment of whether the observed parity exceeds what would be expected from chance capitalization on cohort-specific correlations.
minor comments (1)
- [Abstract] Abstract: the parenthetical descriptions of the five retained items (e.g., 'Q3 (feeling rested)') are helpful but would benefit from an explicit table mapping each to the original QoR-15 wording and subscale for readers outside the immediate domain.
Simulated Author's Rebuttal
Thank you for the constructive review. We address each major comment below, agreeing that greater transparency on validation and methods is needed.
read point-by-point responses
-
Referee: [Abstract] Abstract: the reported AUC-ROC parity (0.968 vs 0.964) and the claim that the selected five-item subset 'tracks readmission events as faithfully as the full form' rest on exhaustive subset selection followed by performance evaluation on the identical internal cohort, with no description of nested cross-validation, pre-specified hold-out, or external test set; this selection procedure is load-bearing for the generalization claim to prospective daily RPM use.
Authors: We agree that subset selection and evaluation were performed on the same internal cohort without nested cross-validation, hold-out set, or external testing. This limits generalization claims and risks cohort-specific overfitting. We will revise the abstract, methods, and discussion to explicitly describe the procedure as internal validation only, qualify the readmission tracking as cohort backtesting, and strengthen emphasis on the need for prospective external validation before clinical deployment. revision: yes
-
Referee: [Abstract] Abstract: the manuscript supplies no cohort size, patient demographics, handling of missing data, or statistical test used to declare the two AUC values 'statistically comparable'; these omissions prevent assessment of whether the observed parity exceeds what would be expected from chance capitalization on cohort-specific correlations.
Authors: We will add these details in revision: cohort size and demographics in Methods/Results, missing data handling (e.g., exclusion or imputation rules), and the statistical test for AUC comparability (e.g., bootstrap or DeLong test). The abstract will reference the updated methods to allow assessment of chance capitalization risk. revision: yes
Circularity Check
No significant circularity; empirical selection and evaluation on internal cohort with no equations or self-citation chains
full rationale
The paper contains no equations, derivations, or first-principles claims. It describes an exhaustive enumeration of 3003 five-item subsets on the authors' single post-surgical deployment cohort, followed by direct reporting of AUC-ROC performance for the selected subset on that same data. This is a standard (if optimistic) empirical feature-selection procedure rather than any reduction of a claimed prediction to its inputs by construction. No self-citations, uniqueness theorems, or ansatzes are invoked as load-bearing steps. The result is therefore self-contained as a data-driven report on the deployment cohort without circularity under the enumerated patterns.
Axiom & Free-Parameter Ledger
Reference graph
Works this paper leans on
-
[1]
Shaik T, Tao X, Higgins N, et al. Remote patient monitoring using artificial intelligence: Current state, applications, and challenges.WIREs Data Mining and Knowledge Discovery. 2023;13(2):e1485. doi:https://doi.org/10.1002/widm.1485
-
[2]
Churruca K, Pomare C, Ellis LA, et al. Patient-reported outcome measures (PROMs): A review of generic and condition-specific measures and a discussion of trends and issues.Health Expectations. 2021;24(4):1015–1024. doi:https://doi.org/10.1111/hex.13254
-
[3]
Stark PA, Myles PS, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score: the QoR-15.Anesthesiology. 2013;118(6):1332–1340. doi:https://doi. org/10.1097/ALN.0b013e318289b84b
-
[4]
Myles PS, Shulman MA, Reilly J, Kasza J, Romero L. Measurement of quality of recovery after surgery using the 15-item quality of recovery scale: a systematic review and meta-analysis. British Journal of Anaesthesia. 2022;128(6):1029–1039. doi:https://doi.org/10.1016/j.bja. 2022.03.009
-
[5]
Semple C, Bhatt B, Sharpe S, et al. Using a mobile app for monitoring post-operative quality of recovery of patients at home: a feasibility study.Journal of Medical Internet Research. 2015;17(7):e168. doi:https://doi.org/10.2196/jmir.3851
-
[6]
Temple-Oberle C, Shea-Budgell MA, Tan M, et al. Effect of Smartphone App Postoperative Home Monitoring After Oncologic Surgery on Quality of Recovery: A Randomized Clinical Trial. JAMA Surgery. 2023;158(11):1181–1188. doi:https://doi.org/10.1001/jamasurg.2023.4145
-
[7]
Jour- nal of Systems and Software225, 112326 (2025) https://doi.org/10.1016/j.jss
Kleif J, Gögenur I. Severity classification of the quality of recovery-15 score—An observational study.Journal of Surgical Research. 2018;225:101–107. doi:https://doi.org/10.1016/j.jss. 2017.12.040
-
[8]
Multi-Modal AI for Remote Patient Monitoring in Cancer Care.arXiv preprintarXiv:2512.00949
Liu Y, Stafford R, Khetrapal P, et al. Multi-Modal AI for Remote Patient Monitoring in Cancer Care.arXiv preprintarXiv:2512.00949. 2025.https://arxiv.org/abs/2512.00949
arXiv 2025
-
[9]
HALO-X: A full-stack remote patient monitoring platform for post-cancer recovery
Stafford R, Liu Y, Khetrapal P, Carvalho G, Kocadag H, Surrao D, McBain H, Winter P, Jackson-Spence F, Powles T, Kelly JD, Drobnjak I. HALO-X: A full-stack remote patient monitoring platform for post-cancer recovery. Manuscript under review, 2025. 9
2025
-
[10]
Scikit-learn: Machine Learning in Python
Pedregosa F, Varoquaux G, Gramfort A, et al. Scikit-learn: Machine Learning in Python. Journal of Machine Learning Research. 2011;12:2825–2830
2011
-
[11]
Coste J, Guillemin F, Pouchot J, Fermanian J. Methodological approaches to shortening composite measurement scales.Journal of Clinical Epidemiology. 1997;50(3):247–252. doi:https: //doi.org/10.1016/S0895-4356(97)90533-8
-
[12]
Multimodal strategies to improve surgical outcome.American Journal of Surgery
Kehlet H, Wilmore DW. Multimodal strategies to improve surgical outcome.American Journal of Surgery. 2002;183(6):630–641. doi:https://doi.org/10.1016/S0002-9610(02)00412-3
-
[13]
AI-driven Optimisation of Quality of Recovery (QoR) in Remote Patient Monitoring [abstract]
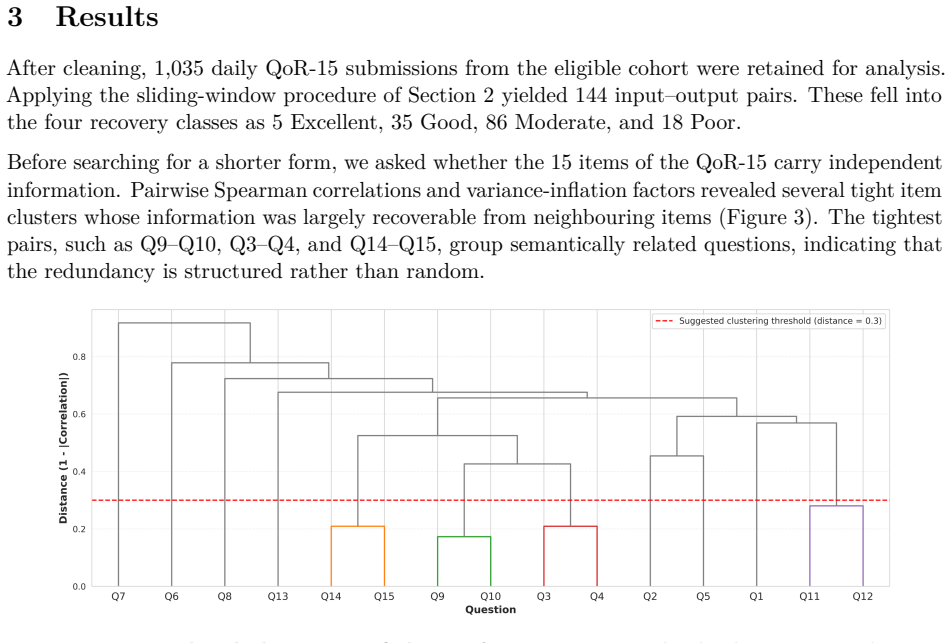
Lin LH, Liu Y, Khetrapal P, et al. AI-driven Optimisation of Quality of Recovery (QoR) in Remote Patient Monitoring [abstract]. Accepted as a poster at AI in Medicine 2026, Polish Institute for Evidence Based Medicine. Available at: piebm.org/abstracts/qor-remote-patient- monitoring Supplementary Material Figure S1:Lower-triangle Spearman correlation matr...
2026
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.