Alzheimer's Disease Diagnosis using a Multimodal Approach with 3D MRI and PET
Pith reviewed 2026-06-26 17:42 UTC · model grok-4.3
The pith
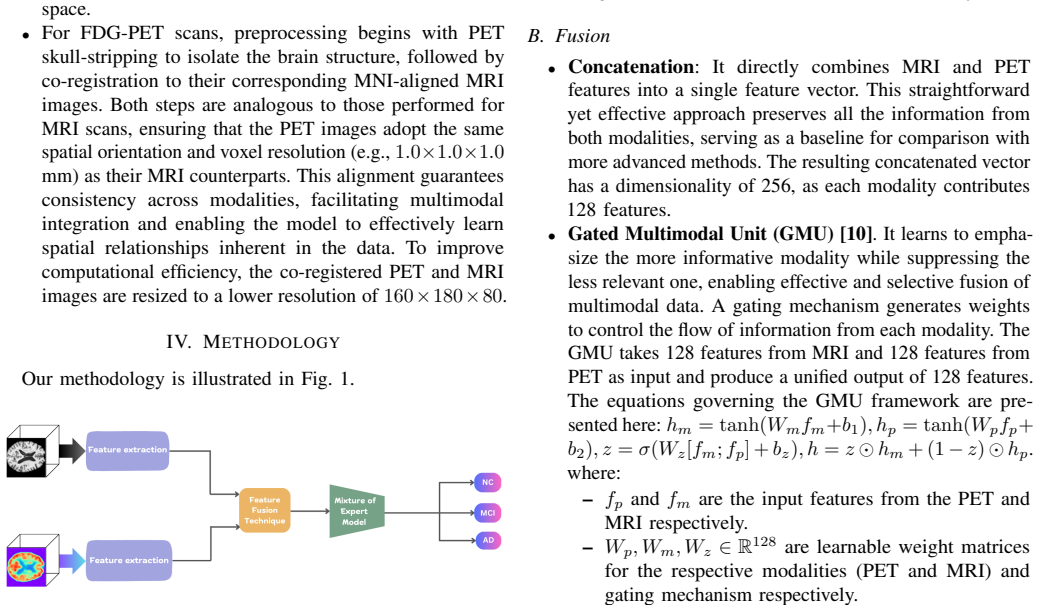
A multimodal model fuses 3D MRI and PET features with gated units or self-attention plus input-adaptive mixture-of-experts routing to classify normal cognition, mild impairment, and Alzheimer's disease.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
The paper establishes that the first reported combination of 3D convolutional feature extractors, concatenation/GMU/gated self-attention fusion, and a sparsely gated MoE classifier with input-adaptive routing produces the reported accuracies on the three binary tasks and that the MoE component consistently improves performance by selecting informative experts per subject.
What carries the argument
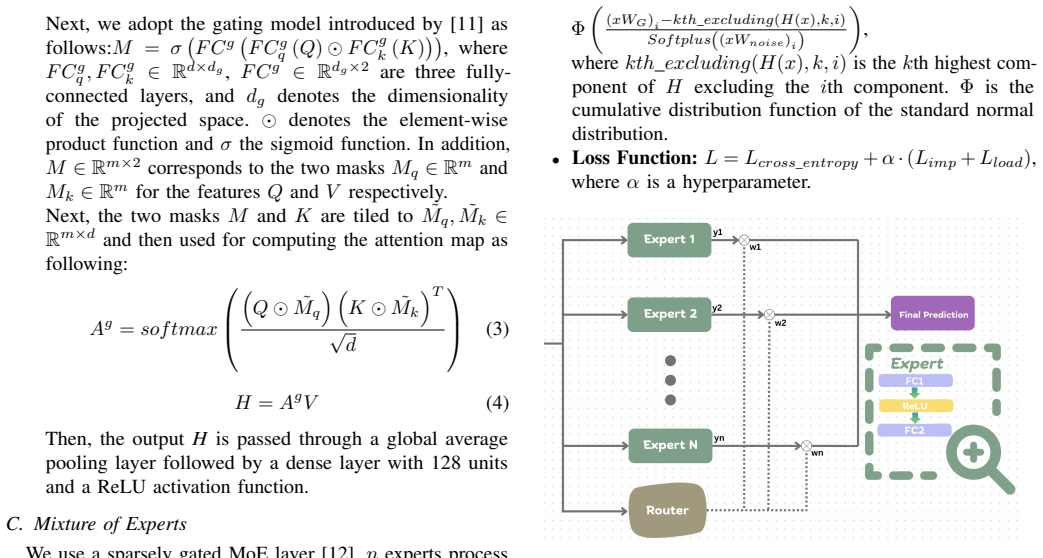
Sparsely gated Mixture-of-Experts classifier that performs input-adaptive routing, activating only the most informative experts per case.
If this is right
- GMU fusion reaches 80.46 percent accuracy separating normal cognition from mild cognitive impairment and 95.47 percent separating normal cognition from Alzheimer's.
- Gated self-attention reaches 82.08 percent accuracy separating mild cognitive impairment from Alzheimer's.
- Removing the mixture-of-experts component lowers accuracy on all three tasks.
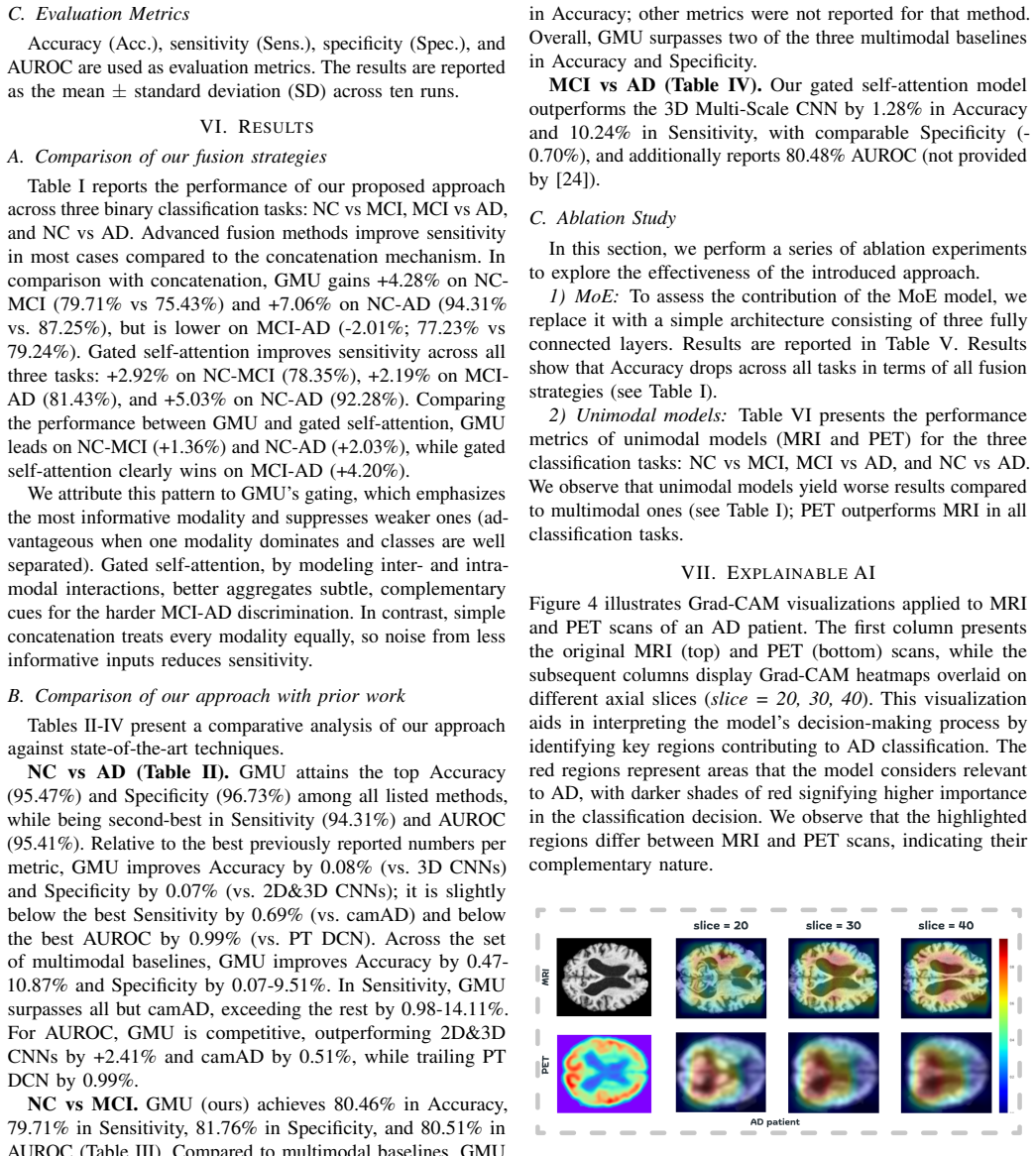
- Grad-CAM produces visualizations of disease-related brain regions.
Where Pith is reading between the lines
- Internal expert routing may supply partial robustness to scanner or site differences that would otherwise require separate domain-adaptation steps.
- The same architecture could be tested on longitudinal scans to predict conversion from mild impairment to Alzheimer's rather than cross-sectional classification alone.
Load-bearing premise
Performance on the three binary tasks from the study's dataset distribution is enough to claim robustness without external validation or explicit site-effect modeling.
What would settle it
A new multi-site test set in which the full model no longer exceeds a simple concatenation baseline or in which any task accuracy falls below 70 percent.
Figures
read the original abstract
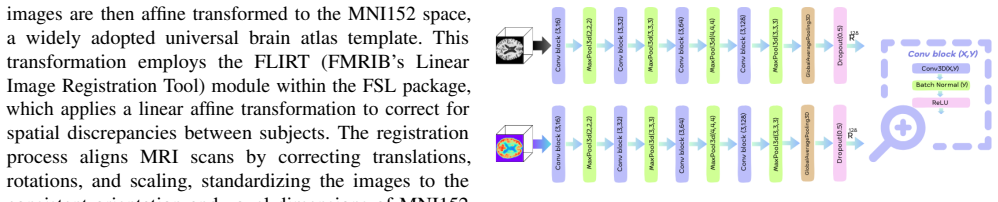
Alzheimer's disease (AD) is an irreversible neurodegenerative disorder and a leading cause of death worldwide. Early diagnosis plays an important part especially at the Mild Cognitive Impairment stage, where timely intervention can help slow its progression before it advances to AD. Neuroimaging data, like Magnetic Resonance Imaging (MRI) and Positron Emission Tomography (PET) scans, can help detect brain changes early by providing structural and functional brain changes related to the disease. Yet, many multimodal models still fuse MRI and PET with static concatenation and apply identical computation to all subjects, which limits robustness to patient/site heterogeneity and can waste computation. To address these limitations, we present the first study of combining 3D convolutional feature extractors with three fusion strategies - concatenation, Gated Multimodal Unit (GMU), and gated self-attention - and a sparsely gated Mixture-of-Experts (MoE) classifier that performs input-adaptive routing, activating only the most informative experts per case. Finally, we utilize Grad-CAM to visualize disease-related regions, ensuring model interpretability. Experiments are performed across three binary classification tasks (NC vs. MCI, MCI vs. AD, and NC vs. AD). Results show that GMU achieves accuracies of 80.46 % (NC vs. MCI) and 95.47 % (NC vs. AD), while gated self-attention attains 82.08 % on MCI vs. AD. Ablations show that removing the MoE consistently degrades accuracy across all tasks. These findings underscore the value of input-adaptive, multimodal modeling for AD diagnosis by leveraging the complementary nature of MRI and PET.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript proposes combining 3D CNN feature extractors from MRI and PET with three fusion strategies (concatenation, Gated Multimodal Unit (GMU), gated self-attention) and a sparsely gated Mixture-of-Experts (MoE) classifier for input-adaptive routing. It evaluates the approach on three binary classification tasks (NC vs. MCI, MCI vs. AD, NC vs. AD), reporting accuracies of 80.46% (GMU on NC vs. MCI), 95.47% (GMU on NC vs. AD), and 82.08% (gated self-attention on MCI vs. AD), with ablations indicating consistent degradation when MoE is removed. Grad-CAM visualizations are used for interpretability, and the work positions itself as addressing limitations of static fusion in handling patient/site heterogeneity.
Significance. If the empirical results can be reproduced with standard experimental controls, the adaptive multimodal fusion via MoE could offer a useful direction for improving robustness in AD neuroimaging models. The explicit comparison of multiple fusion mechanisms plus the ablation on MoE routing provides a concrete test of input-adaptive computation, which is a strength relative to many static multimodal baselines in the literature.
major comments (2)
- [Abstract] Abstract, results paragraph: accuracies (80.46% GMU NC vs. MCI; 95.47% GMU NC vs. AD; 82.08% gated self-attention MCI vs. AD) and the MoE ablation gains are reported without dataset name, subject counts, train/test split protocol, cross-validation method, baseline comparisons, confidence intervals, or statistical tests. These omissions are load-bearing for the central claim that the fusion strategies plus MoE demonstrate value for heterogeneity.
- [Abstract] Abstract and experimental description: the claim that internal MoE routing addresses robustness to patient/site heterogeneity is not supported by any external validation cohort, multi-site analysis, or explicit site-effect modeling. The three binary tasks on an unspecified data distribution therefore cannot be taken as evidence that performance differences arise from multimodal complementarity rather than in-distribution artifacts or leakage.
minor comments (1)
- [Abstract] The abstract states this is the 'first study' combining the listed components; a more detailed positioning against prior multimodal AD work (e.g., other GMU or attention-based fusions) would strengthen the introduction.
Simulated Author's Rebuttal
We thank the referee for the constructive feedback, which identifies key areas where the abstract and positioning of results can be strengthened for clarity and rigor. We respond to each major comment below.
read point-by-point responses
-
Referee: [Abstract] Abstract, results paragraph: accuracies (80.46% GMU NC vs. MCI; 95.47% GMU NC vs. AD; 82.08% gated self-attention MCI vs. AD) and the MoE ablation gains are reported without dataset name, subject counts, train/test split protocol, cross-validation method, baseline comparisons, confidence intervals, or statistical tests. These omissions are load-bearing for the central claim that the fusion strategies plus MoE demonstrate value for heterogeneity.
Authors: We agree that the abstract must supply sufficient context for the reported numbers. The full manuscript details the dataset, subject counts, train/test splits, cross-validation protocol, baselines, confidence intervals, and statistical tests in the Methods and Experiments sections. To address this directly, we will revise the abstract to include concise mentions of the dataset, evaluation protocol, and statistical significance of the MoE gains. revision: yes
-
Referee: [Abstract] Abstract and experimental description: the claim that internal MoE routing addresses robustness to patient/site heterogeneity is not supported by any external validation cohort, multi-site analysis, or explicit site-effect modeling. The three binary tasks on an unspecified data distribution therefore cannot be taken as evidence that performance differences arise from multimodal complementarity rather than in-distribution artifacts or leakage.
Authors: We acknowledge that the current experiments use a single dataset without external validation cohorts, multi-site analysis, or explicit site-effect modeling, and thus do not provide direct evidence against leakage or in-distribution artifacts. The MoE ablation results demonstrate the benefit of input-adaptive routing, but we agree this falls short of proving robustness to patient/site heterogeneity. We will revise the abstract, introduction, and discussion to tone down the claim, framing the MoE as a promising mechanism for handling heterogeneity and explicitly noting the need for future multi-site validation. revision: yes
Circularity Check
No circularity: purely empirical results from held-out evaluation
full rationale
The paper reports experimental accuracies from training and testing multimodal 3D CNN models (with GMU, gated self-attention, and MoE) on three binary AD classification tasks. No derivation chain, equations, or first-principles claims exist that could reduce to inputs by construction. Ablation results and Grad-CAM visualizations are likewise direct empirical measurements. The work contains no self-definitional loops, fitted inputs renamed as predictions, or load-bearing self-citations that would trigger any of the enumerated circularity patterns. This is a standard empirical ML paper whose central claims rest on external data splits rather than internal redefinitions.
Axiom & Free-Parameter Ledger
free parameters (2)
- MoE routing and expert weights
- Fusion gate parameters in GMU and self-attention
axioms (1)
- domain assumption MRI and PET scans supply complementary structural and functional signals for AD staging
Reference graph
Works this paper leans on
-
[1]
Brain glucose metabolism in the early and specific diagnosis of alzheimer’s disease: Fdg-pet studies in mci and ad,
L. Mosconi, “Brain glucose metabolism in the early and specific diagnosis of alzheimer’s disease: Fdg-pet studies in mci and ad,”European journal of nuclear medicine and molecular imaging, vol. 32, no. 4, pp. 486–510, 2005
2005
-
[2]
Khan and R
R. Khan and R. C. Petersen,Mild Cognitive Impairment. Treasure Island, FL: StatPearls Publishing, 2024, available from: https://www.ncbi. nlm.nih.gov/books/NBK554221/
2024
-
[3]
The role of amyloid pet in imaging neurodegenerative disorders: a review,
M. Chapleau, L. Iaccarino, D. Soleimani-Meigooni, and G. D. Rabinovici, “The role of amyloid pet in imaging neurodegenerative disorders: a review,” Journal of Nuclear Medicine, vol. 63, no. Supplement 1, pp. 13S–19S, 2022
2022
-
[4]
Quantitative structural mri for early detection of alzheimer’s disease,
L. K. McEvoy and J. B. Brewer, “Quantitative structural mri for early detection of alzheimer’s disease,”Expert review of neurotherapeutics, vol. 10, no. 11, pp. 1675–1688, 2010
2010
-
[5]
Clinical translation of integrated pet-mri for neurodegenerative disease,
T. M. Shepherd and S. Dogra, “Clinical translation of integrated pet-mri for neurodegenerative disease,”Journal of Magnetic Resonance Imaging, 2025
2025
-
[6]
Multimodal deep learning models for early detection of alzheimer’s disease stage,
J. Venugopalan, L. Tong, H. R. Hassanzadeh, and M. D. Wang, “Multimodal deep learning models for early detection of alzheimer’s disease stage,”Scientific reports, vol. 11, no. 1, p. 3254, 2021
2021
-
[7]
Multimodal 3d deep learning for early diagnosis of alzheimer’s disease,
S. K. Kim, Q. A. Duong, and J. K. Gahm, “Multimodal 3d deep learning for early diagnosis of alzheimer’s disease,”IEEE Access, vol. 12, pp. 46 278–46 289, 2024
2024
-
[8]
Task-induced pyramid and attention gan for multimodal brain image imputation and classification in alzheimer’s disease,
X. Gao, F. Shi, D. Shen, and M. Liu, “Task-induced pyramid and attention gan for multimodal brain image imputation and classification in alzheimer’s disease,”IEEE Journal of Biomedical and Health Informatics, vol. 26, no. 1, pp. 36–43, 2022
2022
-
[9]
Multimodal medical image feature representation and fusion for ad early diagnosis,
J. Qu, Y . Qu, X. Bai, L. Xu, H. Wang, and G. Liu, “Multimodal medical image feature representation and fusion for ad early diagnosis,” in 2024 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), 2024, pp. 1645–1648. TABLE V: Ablation Study. Performance without the MoE framework. Results are averaged across 10 runs. Fusion Method Task ...
2024
-
[10]
Neural Computing and Applications32(14), 10209–10228 (Jul 2020)
J. Arevalo, T. Solorio, M. Montes-y Gómez, and F. A. González, “Gated multimodal networks,”Neural Comput. Appl., vol. 32, no. 14, p. 10209–10228, Jul. 2020. [Online]. Available: https: //doi.org/10.1007/s00521-019-04559-1
-
[11]
Multimodal unified attention networks for vision-and-language interactions,
Z. Yu, Y . Cui, J. Yu, D. Tao, and Q. Tian, “Multimodal unified attention networks for vision-and-language interactions,”arXiv preprint arXiv:1908.04107, 2019
arXiv 1908
-
[12]
Outrageously large neural networks: The sparsely-gated mixture-of-experts layer,
N. Shazeer, A. Mirhoseini, K. Maziarz, A. Davis, Q. Le, G. Hinton, and J. Dean, “Outrageously large neural networks: The sparsely-gated mixture-of-experts layer,” inInternational Conference on Learning Representations, 2017. [Online]. Available: https://openreview.net/forum? id=B1ckMDqlg
2017
-
[13]
Grad-cam: Visual explanations from deep networks via gradient-based localization,
R. R. Selvaraju, M. Cogswell, A. Das, R. Vedantam, D. Parikh, and D. Batra, “Grad-cam: Visual explanations from deep networks via gradient-based localization,” inProceedings of the IEEE International Conference on Computer Vision (ICCV), Oct 2017
2017
-
[14]
Random forest ensembles for detection and prediction of alzheimer’s disease with good between-cohort robustness,
A. V . Lebedev, E. Westman, G. J. P. Van Westen, M. G. Kramberger, A. Lundervold, D. Aarsland, and et al., “Random forest ensembles for detection and prediction of alzheimer’s disease with good between-cohort robustness,”NeuroImage: Clinical, vol. 6, pp. 115–125, 2014
2014
-
[15]
Predicting alzheimer’s disease: a neu- roimaging study with 3d convolutional neural networks,
A. Payan and G. Montana, “Predicting alzheimer’s disease: a neu- roimaging study with 3d convolutional neural networks,”arXiv preprint arXiv:1502.02506, 2015
Pith/arXiv arXiv 2015
-
[16]
S. Sarraf and G. Tofighi, “Classification of alzheimer’s disease using fmri data and deep learning convolutional neural networks,”arXiv preprint arXiv:1603.08631, 2016
Pith/arXiv arXiv 2016
-
[17]
A deep learning model for early diagnosis of alzheimer’s disease combined with 3d cnn and video swin transformer,
J. Zhou, Y . Wei, X. Li, W. Zhou, R. Tao, Y . Hua, and H. Liu, “A deep learning model for early diagnosis of alzheimer’s disease combined with 3d cnn and video swin transformer,”Scientific Reports, vol. 15, no. 1, p. 23311, 2025
2025
-
[18]
A deep learning-based ensemble method for early diagnosis of alzheimer’s disease using mri images,
S. Fathi, A. Ahmadi, A. Dehnad, M. Almasi-Dooghaee, M. Sadegh, and A. D. N. Initiative, “A deep learning-based ensemble method for early diagnosis of alzheimer’s disease using mri images,”Neuroinformatics, vol. 22, no. 1, pp. 89–105, 2024
2024
-
[19]
Bilstm-ann: early diagnosis of alzheimer’s disease using hybrid deep learning algorithms,
P. Matlani, “Bilstm-ann: early diagnosis of alzheimer’s disease using hybrid deep learning algorithms,”Multimedia tools and applications, vol. 83, no. 21, pp. 60 761–60 788, 2024
2024
-
[20]
A novel end-to-end hybrid network for alzheimer’s disease detection using 3d cnn and 3d clstm,
Z. Xia, G. Yue, Y . Xu, C. Feng, M. Yang, T. Wang, and B. Lei, “A novel end-to-end hybrid network for alzheimer’s disease detection using 3d cnn and 3d clstm,” in2020 IEEE 17th International Symposium on Biomedical Imaging (ISBI), 2020, pp. 1–4
2020
-
[21]
Early diagnosis of alzheimer’s disease with deep learning,
S. Liu, S. Liu, W. Cai, S. Pujol, R. Kikinis, and D. Feng, “Early diagnosis of alzheimer’s disease with deep learning,” in2014 IEEE 11th International Symposium on Biomedical Imaging (ISBI). Beijing, China: IEEE, 2014, pp. 1015–1018
2014
-
[22]
D. Lu, K. Popuri, G. W. Ding, R. Balachandar, and M. F. Beg, “Multimodal and multiscale deep neural networks for the early diagnosis of alzheimer’s disease using structural mr and fdg-pet images,” Scientific Reports, vol. 8, no. 1, p. 5697, 2018. [Online]. Available: https://doi.org/10.1038/s41598-018-22871-z
-
[23]
Diagnosis of alzheimer’s disease via multi-modality 3d convolutional neural network,
Y . Huang, J. Xu, Y . Zhou, T. Tong, X. Zhuang, and A. D. N. Initiative, “Diagnosis of alzheimer’s disease via multi-modality 3d convolutional neural network,”arXiv preprint arXiv:1902.09904, 2019
arXiv 1902
-
[24]
An effective multimodal image fusion method using mri and pet for alzheimer’s disease diagnosis,
J. Song, J. Zheng, P. Li, X. Lu, G. Zhu, and P. Shen, “An effective multimodal image fusion method using mri and pet for alzheimer’s disease diagnosis,”Frontiers in Digital Health, vol. 3, p. 637386, 2021
2021
-
[25]
Multimodal attention- based deep learning for alzheimer’s disease diagnosis,
M. Golovanevsky, C. Eickhoff, and R. Singh, “Multimodal attention- based deep learning for alzheimer’s disease diagnosis,”arXiv preprint arXiv:2206.08826v2, 2022. [Online]. Available: https://doi.org/10.48550/ arXiv.2206.08826
arXiv 2022
-
[26]
Automated detection of alzheimer’s disease: A multi-modal approach with 3d mri and amyloid pet,
G. Castellano, A. Esposito, E. Lella, G. Montanaro, and G. Vessio, “Automated detection of alzheimer’s disease: A multi-modal approach with 3d mri and amyloid pet,”Scientific Reports, vol. 14, no. 1, p. 5210, 2024
2024
-
[27]
The alzheimer’s disease neuroimaging initiative (adni): Mri methods,
C. R. Jack Jr, M. A. Bernstein, N. C. Fox, P. Thompson, G. Alexander, D. Harveyet al., “The alzheimer’s disease neuroimaging initiative (adni): Mri methods,”Journal of Magnetic Resonance Imaging, vol. 27, no. 4, pp. 685–691, 2008
2008
-
[28]
Multimodal deep learning models for detecting dementia from speech and transcripts,
L. Ilias and D. Askounis, “Multimodal deep learning models for detecting dementia from speech and transcripts,”Frontiers in Aging Neuroscience, vol. V olume 14 - 2022, 2022. [Online]. Available: https://www.frontiersin. org/journals/aging-neuroscience/articles/10.3389/fnagi.2022.830943
-
[29]
Experiment tracking with weights and biases,
L. Biewald, “Experiment tracking with weights and biases,” 2020, software available from wandb.com. [Online]. Available: https: //www.wandb.com/
2020
-
[30]
Pytorch: An imperative style, high- performance deep learning library,
A. Paszke, S. Gross, F. Massa, A. Lerer, J. Bradbury, G. Chanan, T. Killeen, Z. Lin, N. Gimelshein, L. Antiga, A. Desmaison, A. Kopf, E. Yang, Z. DeVito, M. Raison, A. Tejani, S. Chilamkurthy, B. Steiner, L. Fang, J. Bai, and S. Chintala, “Pytorch: An imperative style, high- performance deep learning library,” inAdvances in Neural Information Processing S...
2019
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.