Therapist-Exoskeleton-Patient Interaction for Gait Therapy
Pith reviewed 2026-05-21 23:10 UTC · model grok-4.3
The pith
Virtual spring-damper links between therapist and patient exoskeletons improve stroke gait recovery over standard treadmill guidance.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
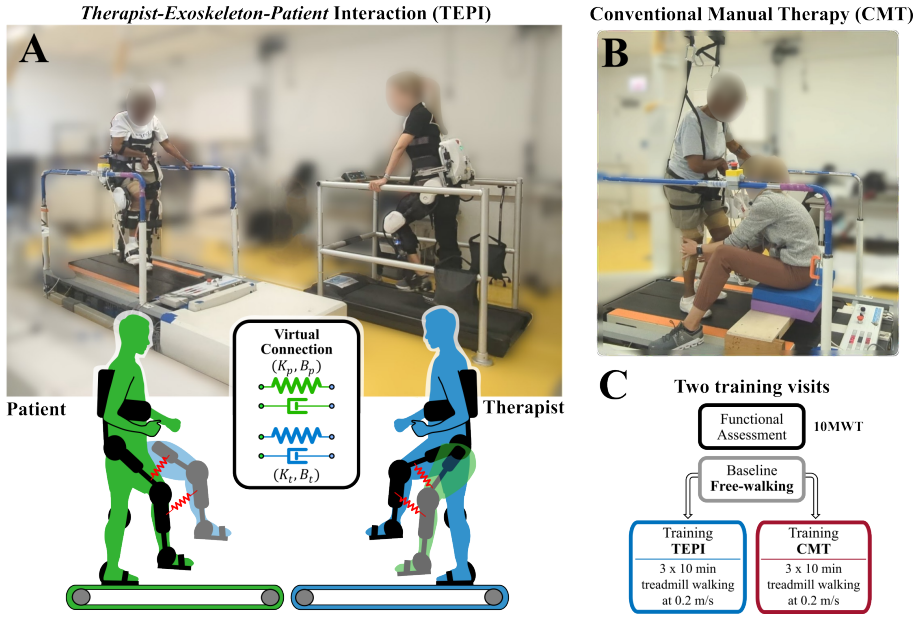
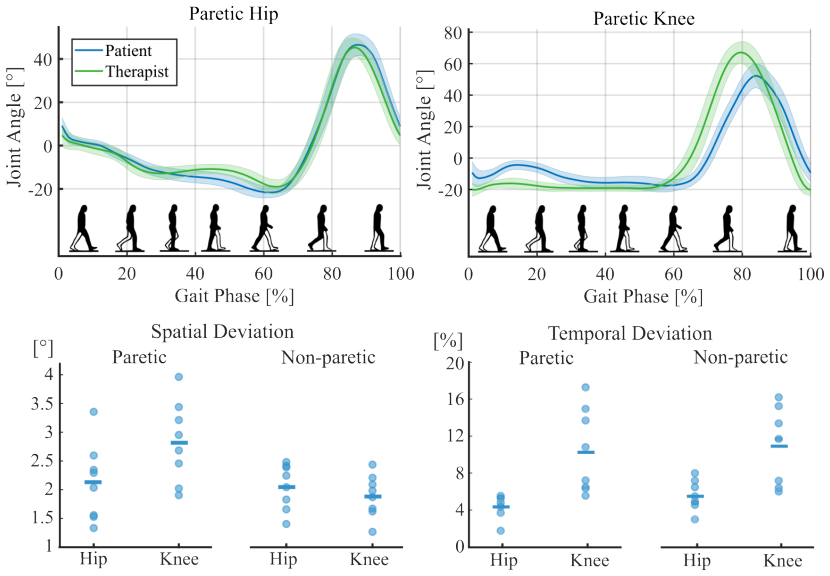
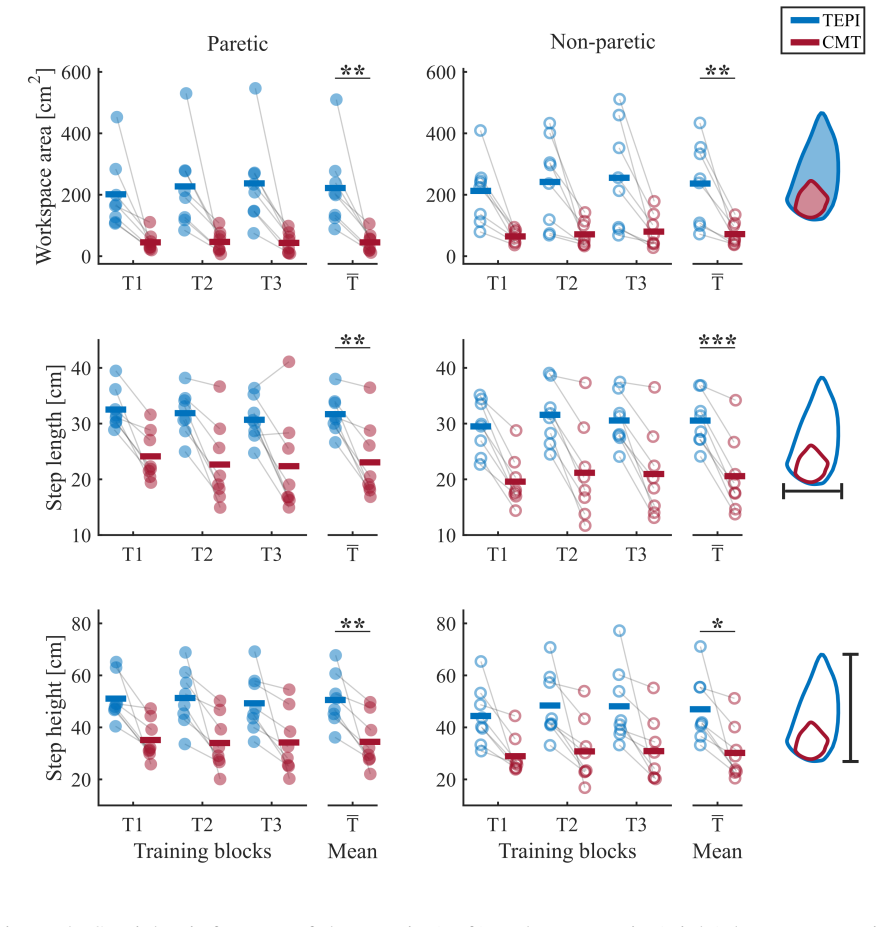
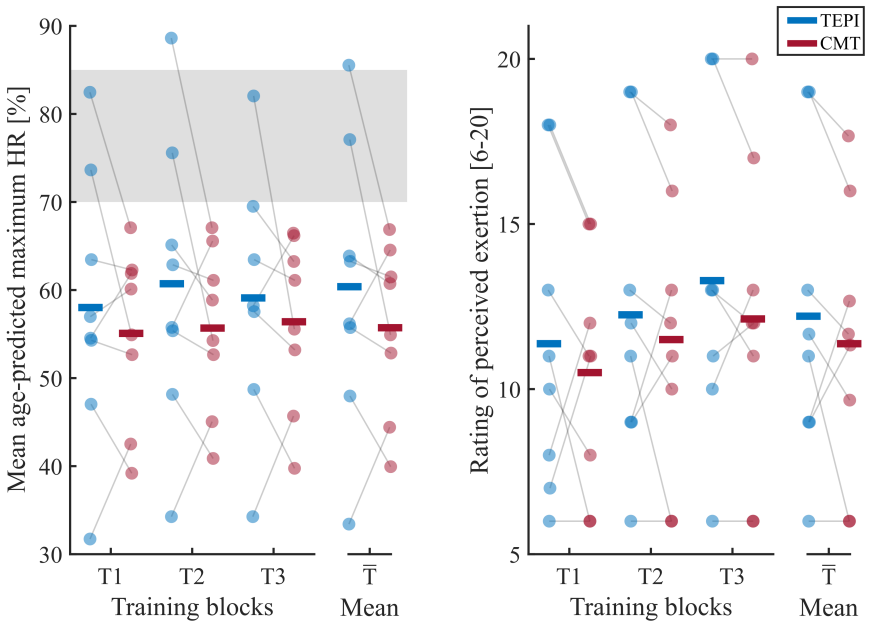
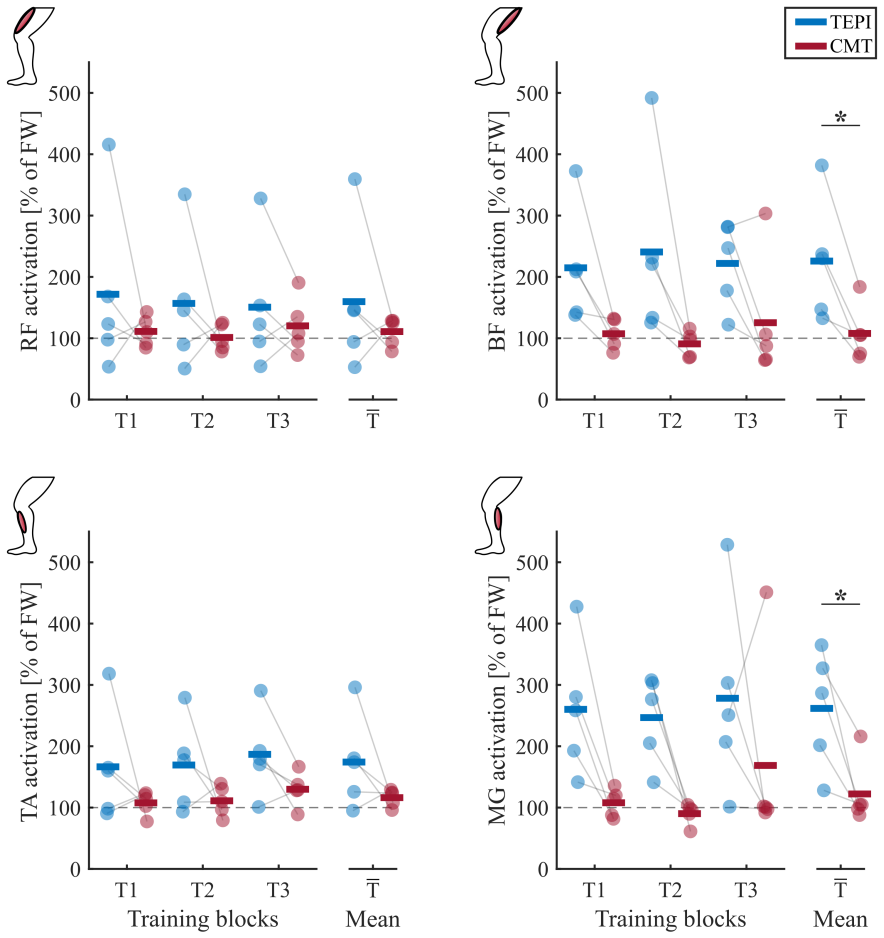
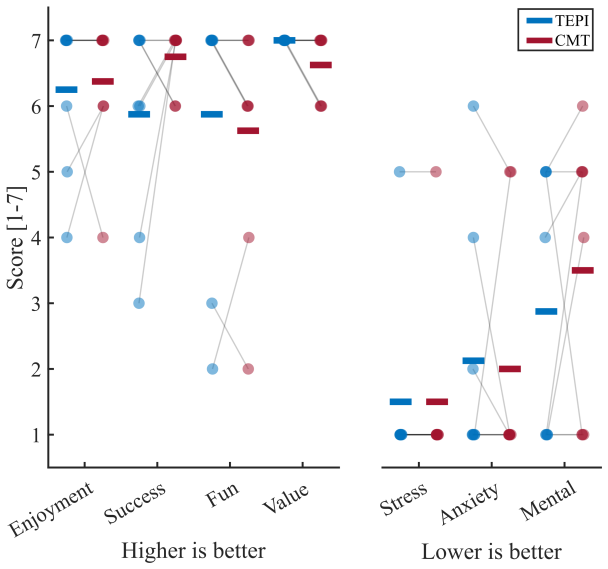
The authors claim that physical Human-Robot-Human Interaction achieved by connecting the exoskeletons of therapist and patient with virtual spring-damper elements at the hips and knees produces bidirectional haptic guidance that yields superior improvements in joint range of motion, step length and symmetry, muscle activation patterns, and patient motivation compared with conventional therapist-guided treadmill walking in eight chronic stroke patients.
What carries the argument
The virtual spring-damper elements that connect the two exoskeletons at the hips and knees and transmit forces bidirectionally so the therapist can both guide and receive real-time haptic feedback from the patient's movements.
If this is right
- Therapists can assist multiple joints at once while experiencing lower physical strain than with direct manual support.
- The robotic system supplies objective measurements that can guide real-time adjustments during a session.
- Patient motivation increases when the therapist's guidance is felt through the haptic channel rather than through spoken cues alone.
- Rehabilitation sessions can combine the precision of robotic actuators with the adaptability of human clinical judgment.
Where Pith is reading between the lines
- One therapist could potentially supervise several patients at the same time if the virtual connections are networked across multiple exoskeletons.
- The same bidirectional link approach could be tested for upper-limb reaching tasks or standing balance training.
- Adaptive controllers might eventually learn from repeated therapist haptic inputs to automate portions of the guidance.
Load-bearing premise
The measured gains in patient performance arise specifically from the bidirectional haptic forces created by the virtual connections rather than from placebo effects, differences in session length, or unmeasured variations in therapist effort.
What would settle it
A follow-up trial that keeps the exoskeletons and therapist present but disables the virtual spring-damper connections and checks whether the advantages in joint motion, stepping, and muscle activity disappear.
Figures
read the original abstract
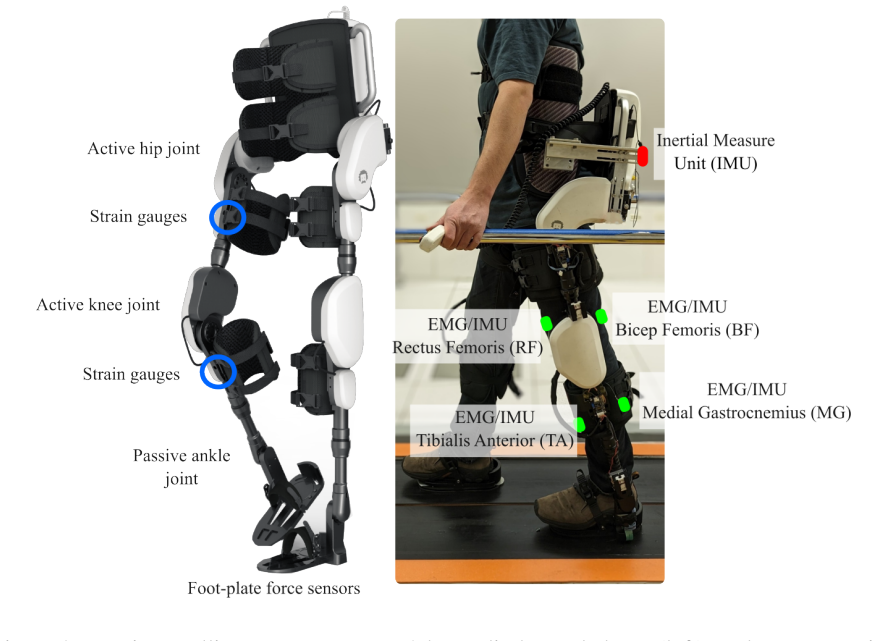
Following a stroke, individuals often experience mobility and balance impairments due to lower-limb weakness and loss of independent joint control. Gait recovery is a key goal of rehabilitation, traditionally achieved through high-intensity therapist-led training. However, manual assistance can be physically demanding and limits the therapist's ability to interact with multiple joints simultaneously. Robotic exoskeletons offer multi-joint support, reduce therapist strain, and provide objective feedback, but current control strategies often limit therapist involvement and adaptability. We present a novel gait rehabilitation paradigm based on physical Human-Robot-Human Interaction (pHRHI), where both the therapist and the post-stroke individual wear lower-limb exoskeletons virtually connected at the hips and knees via spring-damper elements. This enables bidirectional interaction, allowing the therapist to guide movement and receive haptic feedback. In a study with eight chronic stroke patients, pHRHI training outperformed conventional therapist-guided treadmill walking, leading to increased joint range of motion, step metrics, muscle activation, and motivation. These results highlight pHRHI's potential to combine robotic precision with therapist intuition for improved rehabilitation outcomes.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript introduces a physical Human-Robot-Human Interaction (pHRHI) paradigm for post-stroke gait rehabilitation. Both therapist and patient wear lower-limb exoskeletons virtually linked at the hips and knees by spring-damper elements to enable bidirectional haptic guidance and feedback. In a study of eight chronic stroke patients, pHRHI training produced greater gains in joint range of motion, step metrics, muscle activation, and motivation than conventional therapist-guided treadmill walking.
Significance. If the specific contribution of the bidirectional virtual connection can be isolated, the work would offer a meaningful advance in rehabilitation robotics by allowing therapists to provide precise, multi-joint haptic cues while receiving real-time feedback, thereby reducing physical strain and increasing adaptability. The directional improvements reported for n=8 are promising but remain preliminary.
major comments (2)
- [Methods] Methods section (experimental protocol): The sole control condition is conventional therapist-guided treadmill walking without exoskeletons. This design cannot separate the therapeutic effect of the virtual spring-damper bidirectional coupling from the general presence of powered multi-joint exoskeleton assistance, differences in total contact time, or novelty effects. A sham-connection or exoskeleton-only arm is required to support the central claim that the pHRHI interaction itself drives the observed gains in ROM, step metrics, EMG, and motivation.
- [Results] Results and Abstract: Positive directional outcomes are stated for n=8 without reported statistical tests, p-values, effect sizes, error bars, blinding information, or controls for session duration and intensity. These omissions limit the ability to assess the reliability and magnitude of the claimed superiority of pHRHI.
minor comments (1)
- [Abstract] Abstract: The statement that pHRHI 'outperformed' conventional training would be strengthened by inclusion of at least summary quantitative metrics or effect-size information.
Simulated Author's Rebuttal
We thank the referee for their constructive and insightful comments, which have helped us improve the clarity and rigor of the manuscript. We address each major comment below and indicate the revisions made.
read point-by-point responses
-
Referee: [Methods] Methods section (experimental protocol): The sole control condition is conventional therapist-guided treadmill walking without exoskeletons. This design cannot separate the therapeutic effect of the virtual spring-damper bidirectional coupling from the general presence of powered multi-joint exoskeleton assistance, differences in total contact time, or novelty effects. A sham-connection or exoskeleton-only arm is required to support the central claim that the pHRHI interaction itself drives the observed gains in ROM, step metrics, EMG, and motivation.
Authors: We agree that the present design compares pHRHI against standard therapist-guided treadmill walking and therefore cannot fully isolate the contribution of the bidirectional virtual spring-damper coupling from exoskeleton assistance or novelty. This is an inherent limitation of the current preliminary protocol. In the revised manuscript we have added an explicit limitations paragraph in the Discussion that acknowledges this point and outlines planned follow-up experiments that will incorporate an exoskeleton-only arm and a sham-connection condition. We retain the comparison to conventional care because it remains clinically relevant, but we no longer claim that the observed gains are attributable solely to the pHRHI interaction. revision: partial
-
Referee: [Results] Results and Abstract: Positive directional outcomes are stated for n=8 without reported statistical tests, p-values, effect sizes, error bars, blinding information, or controls for session duration and intensity. These omissions limit the ability to assess the reliability and magnitude of the claimed superiority of pHRHI.
Authors: We have revised the Results section and Abstract to include the appropriate statistical tests, p-values, effect sizes, and error bars for all reported outcome measures. Session durations and intensities were matched between conditions; we have now added this detail to the Methods. Full blinding of participants and therapists is not feasible given the physical nature of the intervention, but we have noted this limitation and described the steps taken to minimize bias (e.g., standardized instructions and blinded outcome assessors). revision: yes
Circularity Check
No circularity: empirical outcomes from direct measurements
full rationale
The paper reports results from a controlled study with eight stroke patients comparing pHRHI exoskeleton training against conventional treadmill walking. Central claims rest on measured quantities (joint ROM, step length/cadence, EMG activation, motivation scales) collected during sessions. No equations, parameter fitting, or derivations are presented that could reduce a 'prediction' to its own inputs by construction. No self-citation chains or uniqueness theorems are invoked to justify the core result. The design is self-contained against external benchmarks (pre/post measurements and between-condition comparisons), so the reader's circularity score of 1.0 is consistent with a finding of zero load-bearing circularity.
Axiom & Free-Parameter Ledger
axioms (1)
- domain assumption Exoskeleton assistance and haptic feedback can meaningfully alter gait kinematics and muscle activation in chronic stroke patients.
Lean theorems connected to this paper
-
IndisputableMonolith/Cost/FunctionalEquation.leanwashburn_uniqueness_aczel unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
virtual springs and dampers rendered between their hip and knee joints... τ̂*t = Kt(θ̃p − θt) + Bt(ω̃p − ωt)
-
IndisputableMonolith/Foundation/RealityFromDistinction.leanreality_from_one_distinction unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
pHRHI training outperformed conventional therapist-guided treadmill walking... increased joint range of motion, step metrics, muscle activation
What do these tags mean?
- matches
- The paper's claim is directly supported by a theorem in the formal canon.
- supports
- The theorem supports part of the paper's argument, but the paper may add assumptions or extra steps.
- extends
- The paper goes beyond the formal theorem; the theorem is a base layer rather than the whole result.
- uses
- The paper appears to rely on the theorem as machinery.
- contradicts
- The paper's claim conflicts with a theorem or certificate in the canon.
- unclear
- Pith found a possible connection, but the passage is too broad, indirect, or ambiguous to say the theorem truly supports the claim.
Reference graph
Works this paper leans on
- [1]
-
[2]
N. S ´anchez, A. M. Acosta, R. Lopez-Rosado, A. H. Stienen, J. P. Dewald, Lower extremity motor impairments in ambulatory chronic hemiparetic stroke: evidence for lower extremity weakness and abnormal muscle and joint torque coupling patterns,Neurorehabilitation and neural repair 31, 814 (2017). 28
work page 2017
-
[3]
A.-S. Rudberg, et al., Stroke survivors’ priorities for research related to life after stroke, Topics in stroke rehabilitation28, 153 (2021)
work page 2021
-
[4]
J.-M. Belda-Lois, et al., Rehabilitation of gait after stroke: a review towards a top-down approach, Journal of neuroengineering and rehabilitation 8, 1 (2011)
work page 2011
-
[5]
B. McCrory, et al., Proceedings of the Human Factors and Ergonomics Society Annual Meeting (SAGE Publications Sage CA: Los Angeles, CA, 2014), vol. 58, pp. 1072–1076
work page 2014
-
[6]
K. M. Stephan, D. P ´erennou, Mobility after stroke: relearning to walk, Clinical pathways in stroke rehabilitation: evidence-based clinical practice recommendations pp. 123–147 (2021)
work page 2021
-
[7]
T. Moeller, et al., Use of lower limb exoskeletons as an assessment tool for human motor performance: a systematic review, Sensors 23, 3032 (2023)
work page 2023
-
[8]
R. Gassert, V . Dietz, Rehabilitation robots for the treatment of sensorimotor deficits: a neu- rophysiological perspective, Journal of neuroengineering and rehabilitation 15, 1 (2018)
work page 2018
- [9]
-
[10]
R. Baud, A. R. Manzoori, A. Ijspeert, M. Bouri, Review of control strategies for lower-limb exoskeletons to assist gait, Journal of NeuroEngineering and Rehabilitation 18, 1 (2021)
work page 2021
-
[11]
L. Marchal-Crespo, P. Tsangaridis, D. Obwegeser, S. Maggioni, R. Riener, Haptic error modulation outperforms visual error amplification when learning a modified gait pattern, Frontiers in neuroscience13, 61 (2019). 29
work page 2019
-
[12]
L. Marchal-Crespo, D. J. Reinkensmeyer, Review of control strategies for robotic move- ment training after neurologic injury, Journal of NeuroEngineering and Rehabilitation 6 (2009)
work page 2009
-
[13]
J. Zhang, et al., Human-in-the-loop optimization of exoskeleton assistance during walking, Science 356, 1280 (2017)
work page 2017
-
[14]
C. J. Hasson, J. Manczurowsky, E. C. Collins, M. Yarossi, Neurorehabilitation robotics: how much control should therapists have?, Frontiers in Human Neuroscience 17, 1179418 (2023)
work page 2023
-
[15]
C. Celian, et al. , A day in the life: a qualitative study of clinical decision-making and uptake of neurorehabilitation technology, Journal of neuroengineering and rehabilitation 18, 1 (2021)
work page 2021
-
[16]
E. B. K ¨uc ¸¨uktabak, S. J. Kim, Y . Wen, K. Lynch, J. L. Pons, Human-machine-human in- teraction in motor control and rehabilitation: a review, Journal of NeuroEngineering and Rehabilitation 18, 183 (2021)
work page 2021
-
[17]
E. L. Waters, R. J. Mendonca, P. Z. Cacchione, M. J. Johnson, 2024 10th IEEE RAS/EMBS International Conference for Biomedical Robotics and Biomechatronics (BioRob) (IEEE, 2024), pp. 1498–1503
work page 2024
-
[18]
G. Ganesh, et al., Two is better than one: Physical interactions improve motor performance in humans, Scientific Reports (2014)
work page 2014
- [19]
-
[20]
N. Beckers, E. H. F. van Asseldonk, H. van der Kooij, Haptic human–human interaction does not improve individual visuomotor adaptation, Scientific Reports 10, 19902 (2020)
work page 2020
- [21]
-
[22]
E. J. Avila Mireles, J. Zenzeri, V . Squeri, P. Morasso, D. De Santis, Skill learning and skill transfer mediated by cooperative haptic interaction, IEEE Transactions on Neural Systems and Rehabilitation Engineering 25, 832 (2017)
work page 2017
-
[23]
S. Kager, et al., The effect of skill level matching in dyadic interaction on learning of a tracing task, IEEE International Conference on Rehabilitation Robotics 2019-June, 824 (2019)
work page 2019
-
[24]
S. J. Kim, et al., A framework for dyadic physical interaction studies during ankle motor tasks, IEEE Robotics and Automation Letters 6, 6876 (2021)
work page 2021
-
[25]
S. J. Kim, et al., Effect of dyadic haptic collaboration on ankle motor learning and task performance, IEEE Transactions on Neural Systems and Rehabilitation Engineering 31, 416 (2023)
work page 2023
-
[26]
M. R. Short, et al., Haptic human-human interaction during an ankle tracking task: Effects of virtual connection stiffness, IEEE Transactions on Neural Systems and Rehabilitation Engineering 31, 3864 (2023)
work page 2023
-
[27]
M. R. Short, et al., Effects of uni-and bidirectional interaction during dyadic ankle and wrist tracking, IEEE Transactions on Neural Systems and Rehabilitation Engineering (2025). 31
work page 2025
-
[28]
E. B. K ¨uc ¸¨uktabak, et al. , 2023 International Conference on Rehabilitation Robotics (ICORR) (2023), pp. 1–6
work page 2023
-
[29]
L. Vianello, et al. , 2024 IEEE International Conference on Robotics and Automation (ICRA) (IEEE, 2024), pp. 4521–4527
work page 2024
-
[30]
M. H. Koh, et al., Exploiting telerobotics for sensorimotor rehabilitation: a locomotor em- bodiment, Journal of NeuroEngineering and Rehabilitation 18, 1 (2021)
work page 2021
-
[31]
G. A. BORG, Psychophysical bases of perceived exertion, Medicine & Science in Sports & Exercise 14 (1982)
work page 1982
-
[32]
E. McAuley, T. Duncan, V . V . Tammen, Psychometric properties of the intrinsic motivation inventory in a competitive sport setting: A confirmatory factor analysis,Research quarterly for exercise and sport 60, 48 (1989)
work page 1989
-
[33]
T. M. Sukal, J. P. Dewald, M. D. Ellis, 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference (IEEE, 2006), pp. 5032–5035
work page 2005
- [34]
-
[35]
G. Chen, C. Patten, D. H. Kothari, F. E. Zajac, Gait differences between individuals with post-stroke hemiparesis and non-disabled controls at matched speeds, Gait & posture 22, 51 (2005)
work page 2005
-
[36]
D. C. Kerrigan, E. P. Frates, S. Rogan, P. O. Riley, Spastic paretic stiff-legged gait: Biome- chanics of the unaffected limb: 1, American journal of physical medicine & rehabilitation 78, 354 (1999). 32
work page 1999
-
[37]
H. Souissi, R. Zory, J. Bredin, N. Roche, P. Gerus, Co-contraction around the knee and the ankle joints during post-stroke gait, European journal of physical and rehabilitation medicine 54 (2018)
work page 2018
-
[38]
H. Lim, B. Cleland, S. Madhavan, Functional connectivity of proximal and distal lower limb muscles and impact on gait variability in stroke, Gait & posture 99, 20 (2023)
work page 2023
-
[39]
M. M. Ouellette, et al., High-intensity resistance training improves muscle strength, self- reported function, and disability in long-term stroke survivors, Stroke 35, 1404 (2004)
work page 2004
- [40]
-
[41]
L. Amato, et al., Unidirectional human-robot-human physical interaction for gait training, arXiv preprint arXiv:2409.11510 (2024)
-
[42]
K. L. Poggensee, S. H. Collins, How adaptation, training, and customization contribute to benefits from exoskeleton assistance, Science Robotics 6, eabf1078 (2021)
work page 2021
-
[43]
J. Fong, et al. , CANopen Robot Controller (CORC): An open software stack for hu- man robot interaction development, The International Symposium on Wearable Robotics (WeRob2020) 2020 (2020)
work page 2020
-
[44]
Y . Li, Q. Wei, W. Gou, C. He, Effects of mirror therapy on walking ability, balance and lower limb motor recovery after stroke: a systematic review and meta-analysis of random- ized controlled trials, Clinical rehabilitation 32, 1007 (2018)
work page 2018
-
[45]
E. B. K ¨uc ¸¨uktabak, et al., Haptic transparency and interaction force control for a lower limb exoskeleton, IEEE Transactions on Robotics 40, 1842 (2024). 33
work page 2024
-
[46]
E. Tarihci Cakmak, A. Yaliman, G. Torna, E. I. Sen, The effectiveness of bodyweight- supported treadmill training in stroke patients: randomized controlled trial, Neurological Sciences 45, 3277 (2024). Supplementary Materials Patient Training Block 1 Training Block 2 Training Block 3 (10 mins) (10 mins) (10 mins) Kp[ Nm rad ] Kt[ Nm rad ] Kp[ Nm rad ] Kt[...
work page 2024
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.