A Deep Regression Model for Seed Identification in Prostate Brachytherapy
Pith reviewed 2026-05-25 16:38 UTC · model grok-4.3
The pith
A 3D deep convolutional network regresses CT images to seed probability maps and detects 94.1 percent of implanted brachytherapy seeds.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
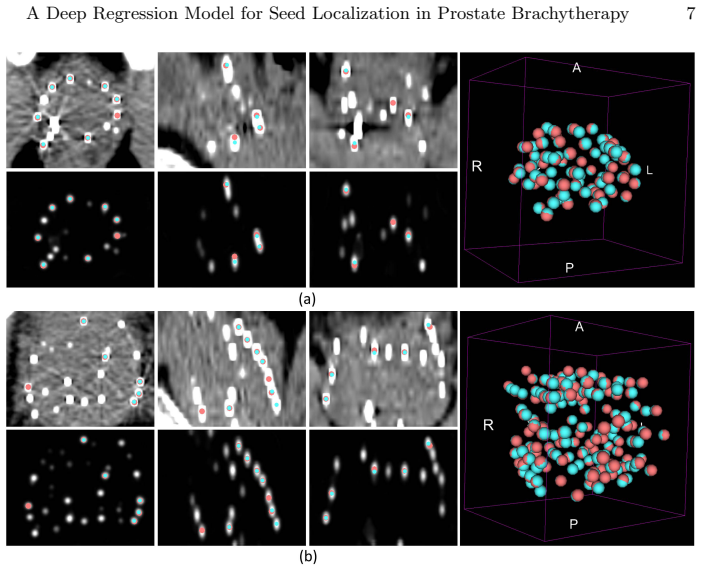
The central claim is that the 3D deep fully convolutional network, trained to map each input CT volume to a corresponding probability volume where each voxel value indicates the chance it belongs to a seed, correctly identifies 2150 of 2286 seeds (94.1 percent) in the held-out test patients and improves detection by 16 percent relative to the VariSeed commercial finder.
What carries the argument
The 3D deep fully convolutional network that outputs a probability map for seed voxels.
If this is right
- The probability map output suppresses metal artifacts and overlapping seed appearances, so downstream localization steps become simpler and more controllable.
- The same trained network can process a clinical database containing thousands of seeds across many patients without per-case manual tuning.
- Detection performance improves by 16 percent over the widely used commercial seed finder on the reported test set.
- The regression formulation avoids direct classification of every voxel and therefore reduces false positives from artifact patterns.
Where Pith is reading between the lines
- The same regression-to-probability-map strategy could be tested on other small metallic objects in artifact-heavy CT scans such as vascular stents or orthopedic hardware.
- If the model maintains accuracy across scanner vendors, clinics could adopt it to shorten the time between seed implantation and final dosimetry review.
- Performance on future patients might drop if CT acquisition protocols or seed types differ from those in the 100-patient training set.
Load-bearing premise
The locations used as ground truth for training and testing are accurate and the 30 test patients match the distribution of future clinical cases.
What would settle it
Running the trained model on a new cohort of patients whose seed positions have been verified by at least two independent observers or by an orthogonal imaging modality and obtaining a detection rate below 85 percent.
Figures
read the original abstract
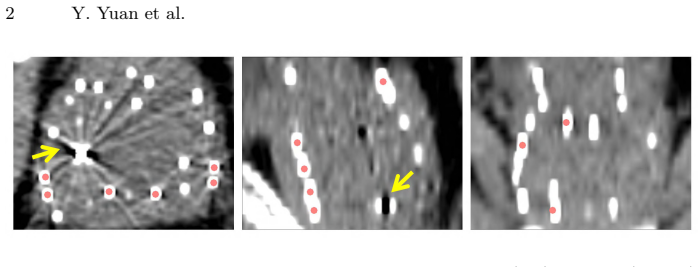
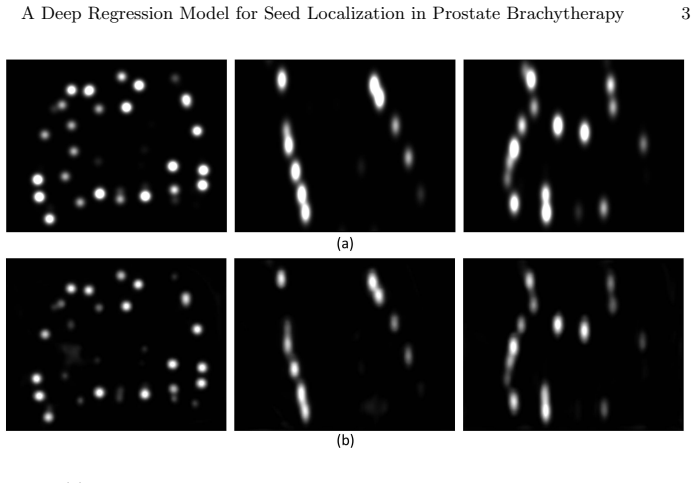
Post-implant dosimetry (PID) is an essential step of prostate brachytherapy that utilizes CT to image the prostate and allow the location and dose distribution of the radioactive seeds to be directly related to the actual prostate. However, it it a very challenging task to identify these seeds in CT images due to the severe metal artifacts and high-overlapped appearance when multiple seeds clustered together. In this paper, we propose an automatic and efficient algorithm based on 3D deep fully convolutional network for identifying implanted seeds in CT images. Our method models the seed localization task as a supervised regression problem that projects the input CT image to a map where each element represents the probability that the corresponding input voxel belongs to a seed. This deep regression model significantly suppresses image artifacts and makes the post-processing much easier and more controllable. The proposed method is validated on a large clinical database with 7820 seeds in 100 patients, in which 5534 seeds from 70 patients were used for model training and validation. Our method correctly detected 2150 of 2286 (94.1%) seeds in the 30 testing patients, yielding 16% improvement as compared to a widely-used commercial seed finder software (VariSeed, Varian, Palo Alto, CA).
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript presents a 3D deep fully convolutional network that models seed localization in post-implant CT as a supervised regression task producing a per-voxel probability map. On a clinical database of 7820 seeds across 100 patients (5534 from 70 patients for training/validation), the method detects 2150 of 2286 seeds (94.1 %) in the 30-patient held-out test set and reports a 16 % improvement over the VariSeed commercial software.
Significance. If the reported detection rate holds under transparent evaluation, the approach could reduce manual effort and improve consistency in post-implant dosimetry, a critical step in prostate brachytherapy. The scale of the clinical dataset (100 patients) is a positive feature of the empirical evaluation.
major comments (3)
- [Abstract] Abstract: the 94.1 % detection rate and 16 % improvement over VariSeed are reported without any description of how the 7820 ground-truth seed locations were established (number of annotators, consensus procedure, or distance tolerance for a correct detection). Because both the proposed regressor and the commercial comparator are scored against the same reference, any systematic bias in the labels renders the delta uninterpretable.
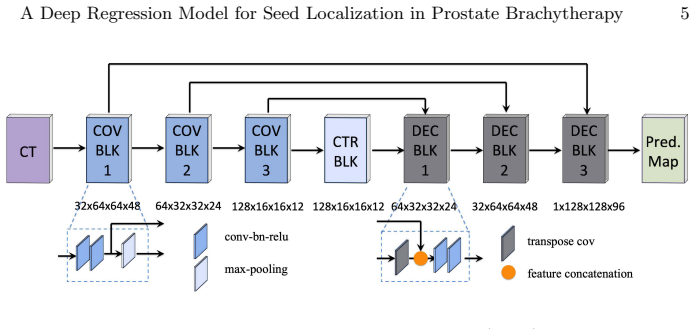
- [Abstract] Abstract (methods section implied by the patient split): no architecture diagram, loss function, optimizer, training schedule, data augmentation, or cross-validation procedure is supplied, so the regression model itself cannot be assessed or reproduced.
- [Abstract] Abstract: the 70/30 patient split is presented without scanner model, imaging protocol, slice thickness, or institution details, leaving the assumption that the test distribution matches future clinical cases unsupported.
minor comments (1)
- [Abstract] Abstract: typographical error 'it it a very challenging task' should read 'it is a very challenging task'.
Simulated Author's Rebuttal
We thank the referee for the constructive feedback. We will revise the manuscript to provide the requested details on ground truth annotation, model implementation, and dataset characteristics.
read point-by-point responses
-
Referee: [Abstract] Abstract: the 94.1 % detection rate and 16 % improvement over VariSeed are reported without any description of how the 7820 ground-truth seed locations were established (number of annotators, consensus procedure, or distance tolerance for a correct detection). Because both the proposed regressor and the commercial comparator are scored against the same reference, any systematic bias in the labels renders the delta uninterpretable.
Authors: We agree that details on how the ground-truth seed locations were established are necessary to interpret the detection rates and the improvement over VariSeed. We will add this information to the revised manuscript, specifying the annotation protocol, number of annotators, consensus procedure, and distance tolerance. This will demonstrate that the same reference was used for both the proposed method and the commercial software, making the comparison valid. revision: yes
-
Referee: [Abstract] Abstract (methods section implied by the patient split): no architecture diagram, loss function, optimizer, training schedule, data augmentation, or cross-validation procedure is supplied, so the regression model itself cannot be assessed or reproduced.
Authors: We acknowledge the lack of these methodological details in the current manuscript. The revised version will include an architecture diagram and a comprehensive description of the loss function, optimizer, training schedule, data augmentation strategies, and cross-validation procedure to allow full assessment and reproduction of the regression model. revision: yes
-
Referee: [Abstract] Abstract: the 70/30 patient split is presented without scanner model, imaging protocol, slice thickness, or institution details, leaving the assumption that the test distribution matches future clinical cases unsupported.
Authors: We will include the missing information on the imaging acquisition in the revised Data section, detailing the scanner model, imaging protocol, slice thickness, and institution. This will support the relevance of the 70/30 split to clinical practice. revision: yes
Circularity Check
No circularity; purely empirical ML performance report on held-out data
full rationale
The paper trains a 3D FCN regression model on 5534 seeds from 70 patients and reports detection performance (2150/2286 seeds, 94.1%) on an independent 30-patient test set. No equations, derivations, fitted parameters renamed as predictions, or self-citation chains appear. The central claim is a direct empirical measurement against a commercial baseline on held-out cases; it does not reduce to its own inputs by construction. Ground-truth label quality is a separate validity concern outside the circularity definition.
Axiom & Free-Parameter Ledger
free parameters (1)
- network weights and hyperparameters
axioms (1)
- domain assumption Ground-truth seed locations in the CT volumes are accurate and free of labeling bias
Reference graph
Works this paper leans on
-
[1]
L., et al.: Cancer Statistics, 2019
Siegel, R. L., et al.: Cancer Statistics, 2019. Cancer J Clin. 69, 7–34 (2019)
work page 2019
-
[2]
Chin, J., et al.: Brachytherapy for patients with prostate cancer: american society of clinical oncology/cancer care ontario joint guideline update. J. Clin Oncol. 35, 1737-43 (2017)
work page 2017
-
[3]
Eur Urology 41, 434-439 (2002)
Stock, R., et al.: Importance of post-implant dosimetry in permanent prostate brachytherapy. Eur Urology 41, 434-439 (2002)
work page 2002
-
[4]
Phys Med Biol 48(9), 1191 - 1203 (2003)
Liu, H., et al.: Automatic localization of implanted seeds from post-implant CT images. Phys Med Biol 48(9), 1191 - 1203 (2003)
work page 2003
-
[5]
J., et al.: An automatic seed finer for brachytherapy CT postplans based on the Hough transform
Holupka, E. J., et al.: An automatic seed finer for brachytherapy CT postplans based on the Hough transform. Med Phys. 31(9), 2672-2679 (2004)
work page 2004
-
[6]
Nguyen, H. G., et al.: Automatic 3D seed location and orientation detection in CT image for prostate brachytherapy. In: IEEE ISBI 2014, pp. 1320-1323. (2014)
work page 2014
-
[7]
Zhang, G., et al.: Automatic seed picking for brachytherapy postimplant validation with 3D CT images. Int J CARS. 12, 1985 - 1993 (2017)
work page 1985
-
[8]
Litjens, et al.: A survey on deep learning in medical image analysis. Med Imag Anal. 42, 60-88 (2017)
work page 2017
-
[9]
Setio, A., et al.: Validation, comparison, and combination of algorithms for au- tomatic detection of pulmonary nodules in computed tomography images: the LUNA16 challenge. Med Imag Anal. 42, 1 - 13 (2017)
work page 2017
-
[10]
Xu, Y., et al: Gland instance segmentation using deep multichannel neural net- works. IEEE Trans. Med. Imaging 64(12), 2901-2912 (2017)
work page 2017
-
[11]
: The liver tumor segmentation benchmark (LiTS)
Bilic, P., et al. : The liver tumor segmentation benchmark (LiTS). arXiv preprint arXiv:1901.04056 (2019)
-
[12]
Yuan, Y., et al.: Automatic skin lesion segmentation using deep fully convolutional networks with Jaccard distance. IEEE Trans. Med. Imaging 36(9), 1876-1886 (2017)
work page 2017
-
[13]
: Automated melanoma recognition in dermoscopy images via very deep residual networks
Yu, L., et al. : Automated melanoma recognition in dermoscopy images via very deep residual networks. IEEE Trans. Med. Imaging 36(4), 994-1004 (2017)
work page 2017
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.