Tracing Like a Clinician: Anatomy-Guided Spatial Priors for Cephalometric Landmark Detection
Pith reviewed 2026-07-01 00:38 UTC · model grok-4.3
The pith
Anatomy-guided spatial priors used only at training time cut cephalometric landmark error to 1.04 mm while closing the validation-to-test gap.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
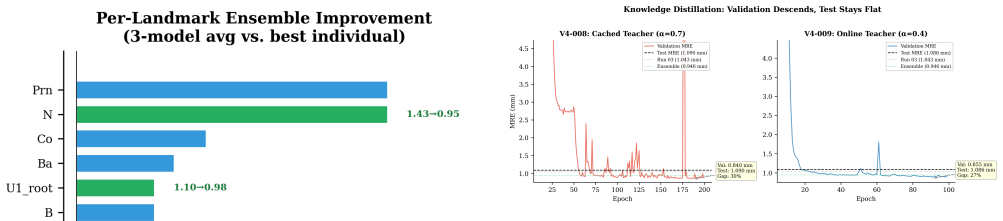
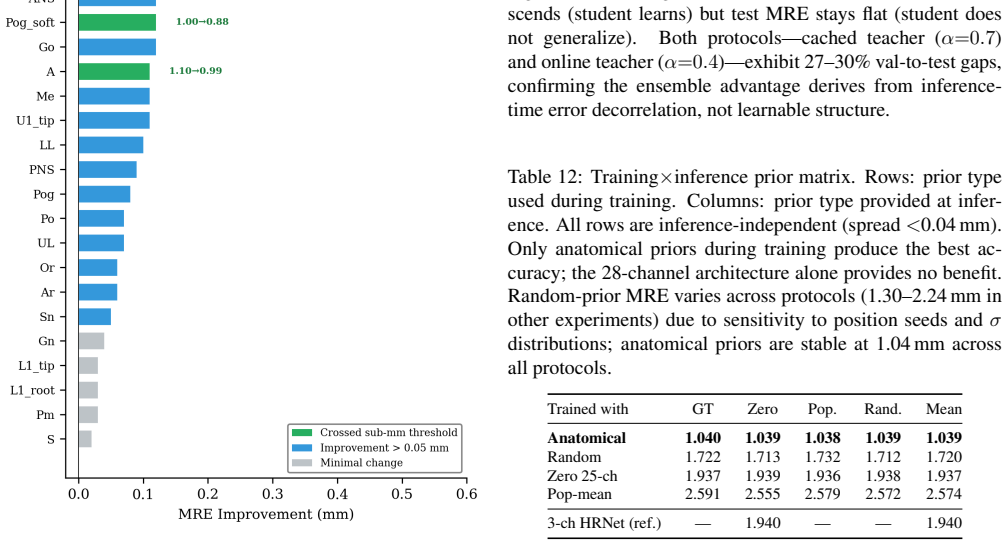
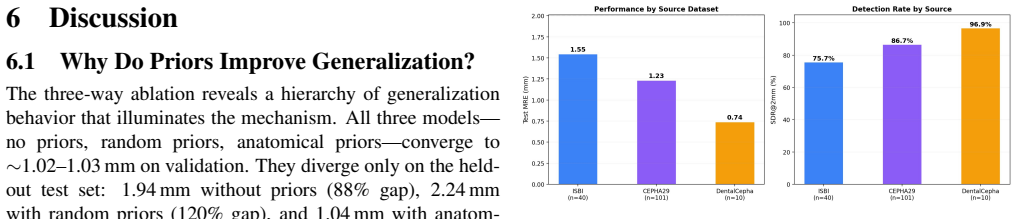
Only image-specific anatomically correct priors produce the 1.04 mm result, functioning as a training-time regularizer requiring no automated prior generation at deployment. The training x inference prior matrix isolates this mechanism: anatomical priors maintain a 1% validation-to-test gap versus 88% without priors, despite identical validation convergence; the expanded architecture alone provides no benefit; random priors yield partial but unstable improvement.
What carries the argument
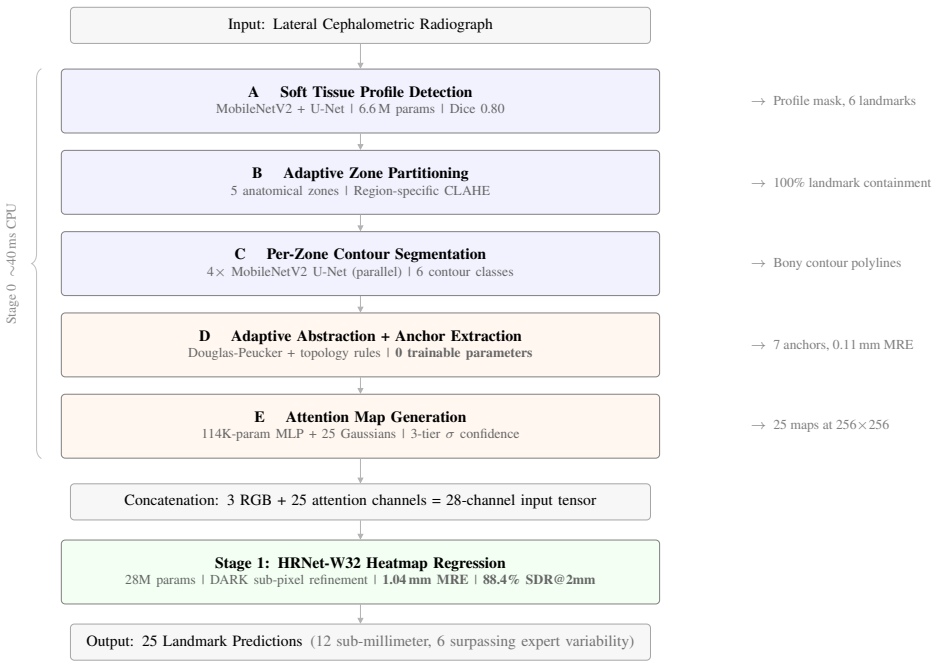
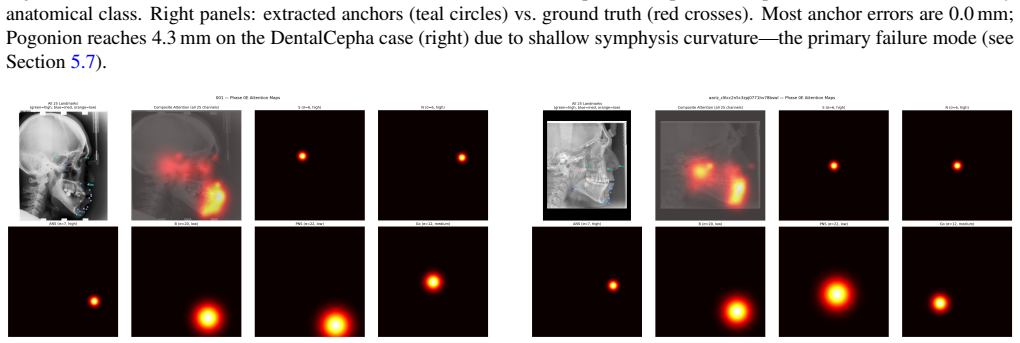
Five-phase anatomy-guided pipeline that produces confidence-weighted spatial priors to shape HRNet-W32 training.
If this is right
- Anatomical priors reduce the validation-to-test performance gap from 88% to 1% while random priors give only partial and unstable gains.
- The architecture expansion alone produces no accuracy benefit without the correct priors.
- The same prior mechanism improves landmark detection in echocardiography, cervical spine, and hand radiographs when spatial entropy is high.
- All trained models remain inference-independent once the priors have shaped the weights.
Where Pith is reading between the lines
- Training-time anatomical regularization may be useful for other structured medical landmark tasks where inference must stay lightweight.
- The observed scaling of prior benefit with spatial entropy suggests a way to decide in advance whether a new imaging domain will respond to this approach.
- Because the priors act only during training, the method could be retrofitted to existing networks without changing their deployment footprint.
Load-bearing premise
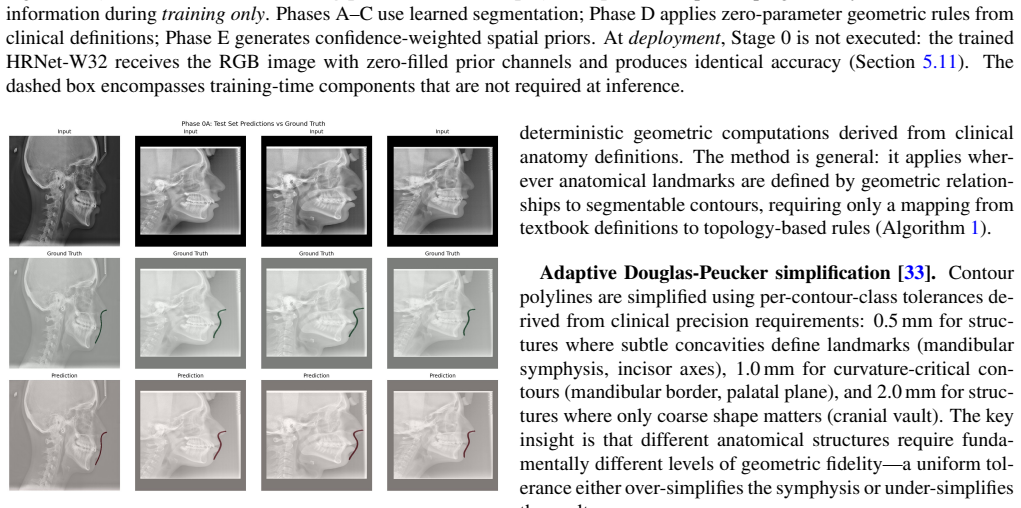
The five-phase pipeline generates priors that accurately reflect true anatomical structures in each radiograph without systematic bias or over-constraint.
What would settle it
Replacing the anatomy-guided priors with spatially plausible but anatomically incorrect priors and observing whether the 1.04 mm error and 1% gap both disappear would falsify the claim that anatomical correctness is required.
Figures





read the original abstract
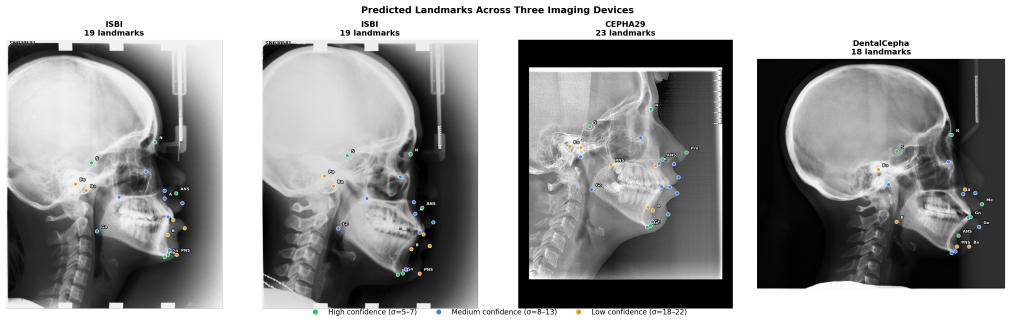
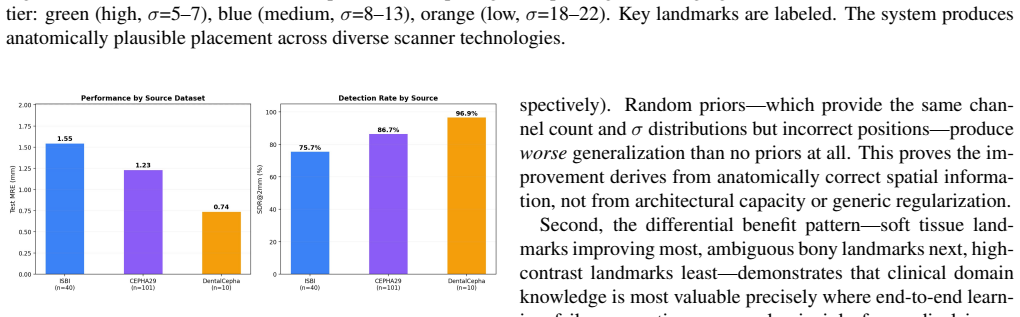
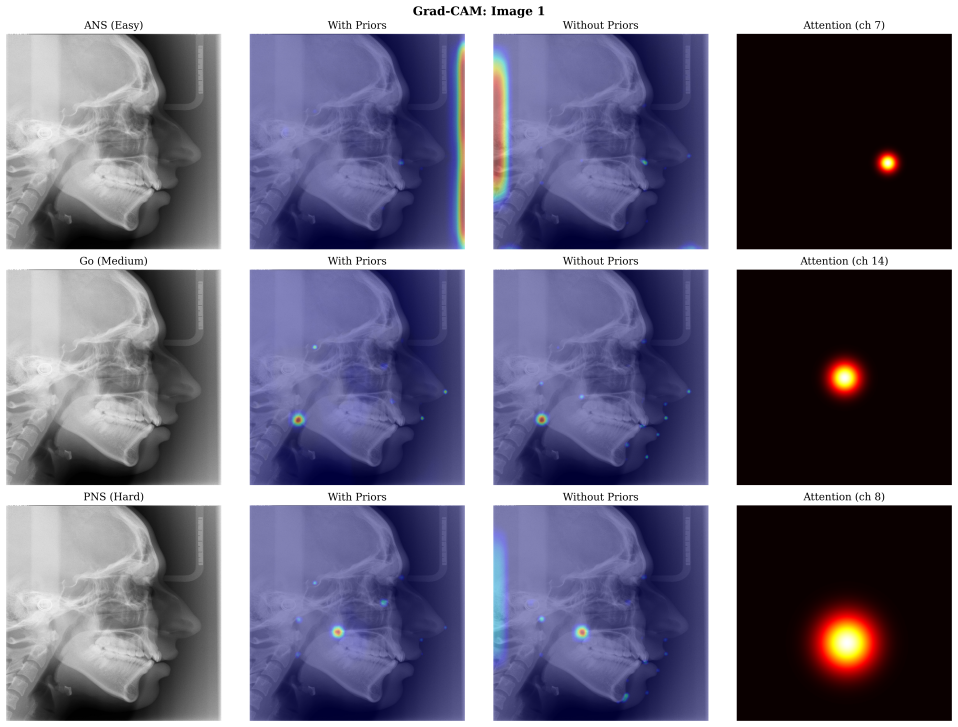
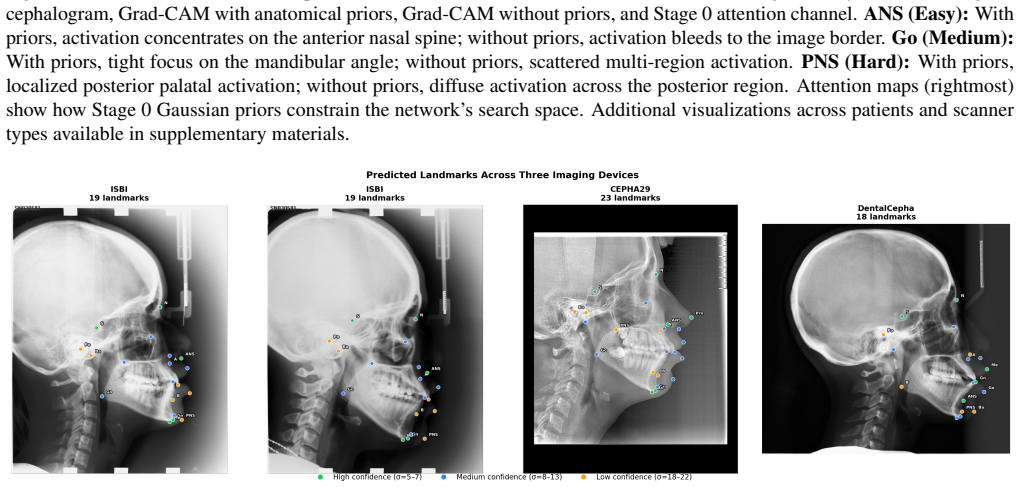
Clinicians trace cephalometric radiographs following a structured anatomical workflow, yet no prior system encodes this into computation. We present a five-phase anatomy-guided pipeline producing confidence-weighted spatial priors that shape HRNet-W32 training, achieving 1.04 mm mean radial error on 25 landmarks across 1,502 radiographs from 7+ imaging devices. A training x inference prior matrix isolates the mechanism: anatomical priors maintain a 1% validation-to-test gap versus 88% without priors (1.94 mm), despite identical validation convergence. The matrix establishes that all trained models are inference-independent, the expanded architecture alone provides no benefit, random priors yield partial but unstable improvement (1.72 mm), and only image-specific anatomically correct priors produce the 1.04 mm result -- functioning as a training-time regularizer requiring no automated prior generation at deployment. Five-fold cross-validation (p=0.0015), patient-level permutation testing (p<0.0001, n=151), quantified Grad-CAM analysis (88% vs. 74% in-zone activation, p<0.001), and clinical measurement validation (skeletal classification kappa=0.79-0.84, zero Class II<->III reversals, ICC>0.95) provide converging evidence. Cross-domain experiments on echocardiography, cervical spine, and hand radiography support the hypothesis that prior effectiveness scales with the spatial entropy of the landmark distribution.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript proposes a five-phase anatomy-guided pipeline to produce confidence-weighted spatial priors that encode clinical tracing workflows. These priors regularize HRNet-W32 training for 25 cephalometric landmarks, yielding 1.04 mm mean radial error on 1,502 radiographs from multiple devices. A training x inference prior matrix is used to isolate the contribution, showing that only image-specific anatomically correct priors (as opposed to random priors, no priors, or architecture changes) achieve the reported performance while maintaining a small 1% validation-to-test gap; the priors act solely as a training regularizer with no requirement at inference. Supporting analyses include five-fold CV (p=0.0015), patient-level permutation testing (p<0.0001), Grad-CAM activation differences (p<0.001), and clinical metrics (kappa 0.79-0.84, ICC>0.95). Cross-domain tests on echocardiography, cervical spine, and hand radiographs are presented to argue that prior utility scales with landmark spatial entropy.
Significance. If the priors can be shown to be independent of ground-truth labels, the work would offer a concrete mechanism for injecting anatomical domain knowledge into landmark detection training without inference overhead. The structured ablation matrix provides a useful template for disentangling prior effects from architecture or data leakage, and the clinical validation plus cross-domain results indicate potential applicability beyond cephalometry when landmark distributions exhibit high spatial entropy.
major comments (1)
- [five-phase anatomy-guided pipeline and training x inference prior matrix] The central claim—that only image-specific anatomically correct priors produce the 1.04 mm result as a training-time regularizer—rests on the five-phase pipeline generating priors that accurately reflect true anatomy without systematic bias or label leakage from the 25 GT landmarks. No quantitative check (e.g., prior-mode to GT-landmark distance, spatial overlap, or correlation metrics) is reported in the pipeline description or the training x inference prior matrix analysis to confirm independence from the annotation process used for supervision. This leaves open the possibility that the performance gap versus random priors (1.72 mm) and the small val-to-test gap reflect partial leakage rather than pure anatomical regularization.
Simulated Author's Rebuttal
We thank the referee for the constructive feedback, particularly the focus on confirming that the spatial priors are independent of ground-truth labels. We address the concern directly below.
read point-by-point responses
-
Referee: [five-phase anatomy-guided pipeline and training x inference prior matrix] The central claim—that only image-specific anatomically correct priors produce the 1.04 mm result as a training-time regularizer—rests on the five-phase pipeline generating priors that accurately reflect true anatomy without systematic bias or label leakage from the 25 GT landmarks. No quantitative check (e.g., prior-mode to GT-landmark distance, spatial overlap, or correlation metrics) is reported in the pipeline description or the training x inference prior matrix analysis to confirm independence from the annotation process used for supervision. This leaves open the possibility that the performance gap versus random priors (1.72 mm) and the small val-to-test gap reflect partial leakage rather than pure anatomical regularization.
Authors: We agree that a direct quantitative check for independence would strengthen the central claim. The five-phase pipeline derives priors from a structured clinical tracing workflow using general anatomical rules and image features, without reference to the specific 25 cephalometric ground-truth positions. The training × inference matrix already isolates the effect: only image-specific anatomically correct priors reach 1.04 mm with a 1% val-to-test gap, whereas random priors yield only 1.72 mm (unstable) and architecture-only or no-prior variants fail to close the gap. This differential performance is inconsistent with systematic leakage, which would be expected to advantage non-anatomical conditions similarly. Nevertheless, to address the referee's point explicitly, we will add the requested metrics (prior-mode to GT distance, spatial overlap, and correlation) in the revised manuscript. revision: yes
Circularity Check
Derivation chain self-contained with no reduction to inputs by construction
full rationale
The paper establishes its central claim via an empirical training x inference prior matrix that directly compares anatomical priors against random priors, no priors, and architecture-only baselines, with the 1.04 mm result isolated to image-specific anatomical correctness. Supporting evidence includes five-fold cross-validation, patient-level permutation testing, Grad-CAM quantification, and clinical measurement validation (kappa, ICC), none of which reduce to the input labels by definition or self-citation. No equations, fitted parameters renamed as predictions, or load-bearing self-citations appear in the provided text; the five-phase pipeline is described as an external anatomical workflow rather than a tautological encoding of the 25 GT landmarks. The result is therefore not forced by construction.
Axiom & Free-Parameter Ledger
axioms (1)
- domain assumption The five-phase anatomy-guided pipeline produces image-specific anatomically correct priors that reflect true landmark distributions
Reference graph
Works this paper leans on
-
[1]
H. W. Fields, B. E. Larson, D. M. Sarver, W. R. Proffit.Con- temporary Orthodontics, 7th ed. Elsevier, 2024
2024
-
[2]
Wang et al
C.-W. Wang et al. Evaluation and comparison of anatomical landmark detection methods for cephalometric x-ray images: A grand challenge.IEEE Trans. Med. Imaging, 34(9):1890–1900, 2015
1900
-
[3]
Lindner and T
C. Lindner and T. F. Cootes. Fully automatic cephalometric evaluation using random forest regression-voting. InProc. IEEE ISBI, 2015
2015
-
[4]
Zeng et al
M. Zeng et al. Cascaded convolutional networks for automatic cephalometric landmark detection.Medical Image Analysis, 68:101904, 2021
2021
-
[5]
Chen et al
R. Chen et al. Cephalometric landmark detection by attentive feature pyramid fusion and regression-voting. InProc. MICCAI, pp. 873–881, 2019
2019
-
[6]
A. Jaheen et al. CephRes-MHNet: A multi-head residual net- work for cephalometric landmark detection.arXiv:2511.10173, 2025
- [7]
-
[8]
H. J. Kwon et al. Automated cephalometric landmark detec- tion with confidence regions using Bayesian CNNs.BMC Oral Health, 20:270, 2020
2020
-
[9]
Son et al
I. Son et al. Ceph-Net: Automatic detection of cephalometric landmarks using an attention-based stacked regression network. BMC Oral Health, 2023
2023
-
[10]
Zhong et al
Z. Zhong et al. An attention-guided deep regression model for landmark detection in cephalograms. InProc. MICCAI, pp. 540–548, 2019
2019
-
[11]
Oh et al
K. Oh et al. Deep anatomical context feature learning for cephalometric landmark detection.IEEE J. Biomed. Health In- form., 2021
2021
-
[12]
M. A. Khalid et al. A two-stage regression framework for au- tomated cephalometric landmark detection.Expert Syst. Appl., 124840, 2024
2024
-
[13]
M. A. Khalid et al. A benchmark dataset for automatic cephalo- metric landmark detection.Scientific Data, 2025. 14
2025
-
[14]
R. R. Selvaraju et al. Grad-CAM: Visual explanations from deep networks via gradient-based localization. InProc. ICCV, pp. 618–626, 2017
2017
-
[15]
K. Sun, B. Xiao, D. Liu, and J. Wang. Deep high-resolution representation learning for visual recognition. InProc. CVPR, pp. 5693–5703, 2019
2019
-
[16]
Zhang, X
F. Zhang, X. Zhu, H. Dai, M. Ye, and C. Zhu. Distribution- aware coordinate representation for human pose estimation. In Proc. CVPR, pp. 7093–7102, 2020
2020
-
[17]
Payer, D
C. Payer, D. Štern, H. Bischof, and M. Urschler. Integrating spa- tial configuration into heatmap regression based CNNs for land- mark localization.Medical Image Analysis, 54:207–219, 2019
2019
-
[18]
Q. Ma, E. Kobayashi, and B. Fan. Automatic cephalometric landmark detection using modified Swin Transformer. InCL- Detection 2023 MICCAI Workshop, 2023
2023
-
[19]
Chen et al
L. Chen et al. CephalFormer: Multi-head attention in vision transformers for cephalometric landmark detection.Medical Image Analysis, 2023
2023
-
[20]
Wu et al
Y . Wu et al. Multi-scale feature fusion for cephalometric land- mark detection. InCL-Detection 2023 MICCAI Workshop, 2023
2023
-
[21]
Tian et al
Y . Tian et al. A comprehensive survey of cephalometric land- mark detection: Methods, datasets, and future directions.Artifi- cial Intelligence Review, 57:148, 2024
2024
-
[22]
Leclerc, E
S. Leclerc, E. Smistad, J. Pedrosa, A. Östvik, et al. Deep learning for segmentation using an open large-scale dataset in 2D echocardiography.IEEE Trans. Med. Imaging, 38(9):2198– 2210, 2019
2019
-
[23]
J. P. Howard et al. Automated left ventricular dimension assess- ment using artificial intelligence developed and validated by a UK-wide collaborative.Circulation: Cardiovascular Imaging, 14(5):e012135, 2021
2021
-
[24]
Ouyang et al
D. Ouyang et al. Video-based AI for beat-to-beat assessment of cardiac function.Nature, 580(7802):252–256, 2020
2020
-
[25]
K. He, X. Zhang, S. Ren, and J. Sun. Delving deep into recti- fiers: Surpassing human-level performance on ImageNet classi- fication. InProc. ICCV, pp. 1026–1034, 2015
2015
-
[26]
Y . Ran, W. Qin, C. Qin, X. Li, Y . Liu, L. Xu, X. Mu, L. Yan, B. Wang, Y . Dai, J. Chen, and D. Han. A high-quality dataset featuring classified and annotated cervical spine X-ray atlas. Scientific Data, 11(1):631, 2024
2024
-
[27]
Ronneberger, P
O. Ronneberger, P. Fischer, and T. Brox. U-Net: Convolutional networks for biomedical image segmentation. InProc. MICCAI, pp. 234–241, 2015
2015
-
[28]
Sandler, A
M. Sandler, A. Howard, M. Zhu, A. Zhmoginov, and L.- C. Chen. MobileNetV2: Inverted residuals and linear bottle- necks. InProc. CVPR, pp. 4510–4520, 2018
2018
-
[29]
K. He, X. Zhang, S. Ren, and J. Sun. Deep residual learning for image recognition. InProc. CVPR, pp. 770–778, 2016
2016
-
[30]
Distilling the Knowledge in a Neural Network
G. Hinton, O. Vinyals, and J. Dean. Distilling the knowledge in a neural network.arXiv:1503.02531, 2015
work page internal anchor Pith review Pith/arXiv arXiv 2015
-
[31]
Loshchilov and F
I. Loshchilov and F. Hutter. Decoupled weight decay regular- ization. InProc. ICLR, 2019
2019
-
[32]
Loshchilov and F
I. Loshchilov and F. Hutter. SGDR: Stochastic gradient descent with warm restarts. InProc. ICLR, 2017
2017
-
[33]
D. H. Douglas and T. K. Peucker. Algorithms for the reduction of the number of points required to represent a digitized line or its caricature.Cartographica, 10(2):112–122, 1973
1973
-
[34]
bright band
A. Gertych, A. Zhang, J. Sayre, S. Pospiech-Kurkowska, and H. K. Huang. Bone age assessment of children using a digi- tal hand atlas.Computerized Medical Imaging and Graphics, 31(4–5):322–331, 2007. 15 Supplementary Materials: Tracing Like a Clinician: Anatomy-Guided Spatial Priors for Cephalometric Landmark Detection Sidhartha Mohapatra1, Dr. Pallavi Moh...
2007
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.