Beyond WER: A Paired Acoustic Stress Test for Ambient Clinical Scribes
Pith reviewed 2026-06-27 23:49 UTC · model grok-4.3
The pith
Ambient noise nearly doubles unsafe clinical outputs while barely affecting Word Error Rate.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
The paper claims that when stationary ambient noise is added to clinical dialogues, the Word Error Rate rises by only 0.71 percentage points, but the rate of unsafe outputs nearly doubles. This occurs because minor acoustic changes can reverse clinical meaning in ways that standard error counts miss. The paired test design keeps the language model fixed to show the effect comes from the noise on the input. A lightweight mitigation approach reduces the safety loss under these conditions.
What carries the argument
The paired acoustic stress test, which applies controlled noise to identical input dialogues while holding the downstream language model constant to measure effects on clinical safety.
Load-bearing premise
The way unsafe outputs are defined and automatically detected matches the actual risks that matter in clinical practice, and the noise added in tests represents what happens in real clinics.
What would settle it
Direct comparison of the automated unsafe labels with reviews by medical professionals on the same set of noisy transcripts to check agreement.
Figures
read the original abstract
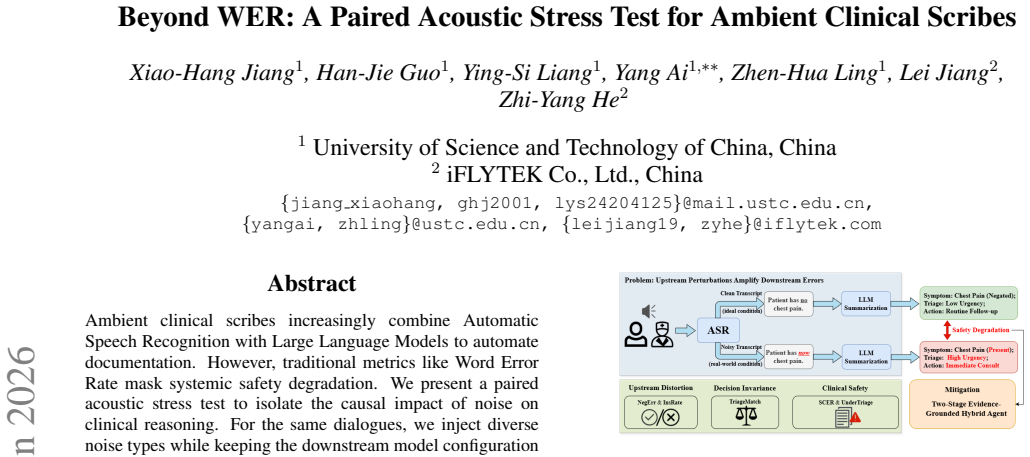
Ambient clinical scribes increasingly combine Automatic Speech Recognition with Large Language Models to automate documentation. However, traditional metrics like Word Error Rate mask systemic safety degradation. We present a paired acoustic stress test to isolate the causal impact of noise on clinical reasoning. For the same dialogues, we inject diverse noise types while keeping the downstream model configuration frozen. Crucially, we uncover a dangerous disconnect between signal fidelity and clinical safety. Stationary ambient noise increased the Word Error Rate by a negligible 0.71 percentage points yet nearly doubled the rate of unsafe outputs. Our analysis reveals that minor acoustic perturbations can invert clinical meaning without substantially inflating error rates. Furthermore, we demonstrate a lightweight mitigation strategy that mitigates safety degradation under noisy conditions without requiring model fine tuning.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript introduces a paired acoustic stress test for ambient clinical scribes that combine ASR with LLMs. By injecting controlled noise types into the same dialogues while freezing the downstream model, the authors report that stationary ambient noise raises Word Error Rate by only 0.71 percentage points yet nearly doubles the rate of unsafe clinical outputs. They conclude that minor acoustic perturbations can invert clinical meaning without substantially inflating conventional error rates and propose a lightweight mitigation that does not require model fine-tuning.
Significance. If the safety metric proves reliable, the work usefully demonstrates that WER is an incomplete proxy for clinical risk in noisy environments and supplies a concrete experimental design for isolating acoustic effects on downstream reasoning. The paired, frozen-model protocol is a clear methodological strength that could be adopted more broadly.
major comments (2)
- [Abstract and §3] Abstract and §3 (safety evaluation): the headline result (0.71 pp WER increase yet ~2× unsafe rate) rests on an automated unsafe-output detector whose definition, training data, inter-rater agreement with clinicians, and correlation with actual clinical harm are not reported. Without external validation, the observed doubling could arise from instability in the detector’s own decision boundary rather than genuine meaning inversion.
- [§4] §4 (experimental setup): no sample size, confidence intervals, or statistical test is supplied for the unsafe-output rate comparison, nor is it stated how many dialogues or noise realizations were used. This omission prevents assessment of whether the reported effect is robust or could be explained by sampling variability.
minor comments (2)
- [Figure 2] Figure 2 caption: the y-axis label for unsafe rate should explicitly state the unit (e.g., fraction of outputs) and whether error bars represent standard error or bootstrap intervals.
- [§2.2] §2.2: the precise prompt or classifier architecture used for the unsafe-output detector should be moved from supplementary material into the main text or an appendix table for reproducibility.
Simulated Author's Rebuttal
We thank the referee for the detailed and constructive report. The two major comments identify important omissions in the reporting of the safety metric and experimental statistics. We address each point below and will incorporate the requested information into the revised manuscript.
read point-by-point responses
-
Referee: [Abstract and §3] Abstract and §3 (safety evaluation): the headline result (0.71 pp WER increase yet ~2× unsafe rate) rests on an automated unsafe-output detector whose definition, training data, inter-rater agreement with clinicians, and correlation with actual clinical harm are not reported. Without external validation, the observed doubling could arise from instability in the detector’s own decision boundary rather than genuine meaning inversion.
Authors: We agree that additional detail on the automated detector is required. In the revised §3 we will supply the exact definition of unsafe outputs, the procedure and data used to train or configure the detector, and any internal agreement statistics that were computed. We will also add an explicit limitations paragraph addressing the absence of external clinician validation and the lack of direct correlation data with downstream clinical harm. At the same time, the paired design—identical dialogues processed under frozen model conditions—limits the scope for detector instability to explain the result, because any systematic bias would have to act differentially on the noisy versus clean versions of the same input. We view the requested additions as strengthening rather than undermining the central claim. revision: yes
-
Referee: [§4] §4 (experimental setup): no sample size, confidence intervals, or statistical test is supplied for the unsafe-output rate comparison, nor is it stated how many dialogues or noise realizations were used. This omission prevents assessment of whether the reported effect is robust or could be explained by sampling variability.
Authors: We acknowledge the omission. The revised §4 will report the exact number of dialogues, the number of independent noise realizations per dialogue, 95 % confidence intervals on the unsafe-output rates, and the results of a paired statistical test (McNemar’s test for the binary unsafe label). These quantities were computed during the original experiments but were inadvertently left out of the submitted text. revision: yes
Circularity Check
No significant circularity; empirical test is self-contained
full rationale
The paper reports an experimental paired acoustic stress test that injects external noise types into dialogues while freezing the downstream model, then measures WER and unsafe output rates. No equations, parameter fitting, predictions derived from fits, or load-bearing self-citations are present in the described chain. The unsafe-output detector is treated as an external automated component without evidence that its definition reduces to the paper's own inputs or results. This matches the default case of a self-contained empirical evaluation against external benchmarks.
Axiom & Free-Parameter Ledger
axioms (1)
- domain assumption Injected noise types represent real clinical ambient conditions and unsafe outputs are correctly identified by the evaluation protocol.
Reference graph
Works this paper leans on
-
[1]
Introduction Ambient clinical scribes, which cascade Automatic Speech Recognition (ASR) with Large Language Models (LLMs), are rapidly transforming healthcare documentation [1, 2, 3, 4]. By unobtrusively recording clinician–patient dialogues and au- tomating the generation of structured notes and decision sup- port, these pipelines promise to alleviate se...
-
[2]
P:I’ve had this dull ache in my right ankle
Proposed Method 2.1. Overview As shown in Fig. 1, we design acontrolled, paired acoustic stress testto systematically attribute downstream clinical errors arXiv:2606.05909v1 [cs.SD] 4 Jun 2026 Table 1:Paired cause→effect examples of ASR-induced safety degradation. ASR Error Type (Cause) Paired Transcript Example (Clean vs. Noisy) Downstream LLM Impact (Ef...
Pith/arXiv arXiv 2026
-
[3]
Dataset Setup Clinical Corpus.We instantiate our OSCE framework using the open-source dataset by Fareez et al
Experiment 3.1. Dataset Setup Clinical Corpus.We instantiate our OSCE framework using the open-source dataset by Fareez et al. [22]. This corpus com- prises272English encounters (approximately 52 hours), cov- ering a diverse case mix of five specialties: respiratory, car- diovascular, gastrointestinal, musculoskeletal, and dermatolog- ical. All recordings...
-
[4]
never-event
(via an official API service) to decompose the clean hu- man transcripts into a set of atomic clinical facts (e.g., specific symptoms, medication status, timeframes). Crucially, these candidate claims underwent a physician audit, where clinical experts corrected hallucinations and supplemented omitted de- tails to ensure high clinical validity. This proce...
-
[5]
Conclusion We presented a paired counterfactual noise stress test for ASR→LLM clinical scribe pipelines, isolating how controlled acoustic perturbations propagate into downstream clinical- claim drift. Across realistic noise families, we find that safety- relevant errors can increase even when transcript-level fidelity changes appear modest, highlighting ...
-
[6]
After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the final version of the manuscript
Generative AI Use Disclosure During the preparation of this manuscript, the authors used ChatGPT 5.2 to polish the language and improve the flow of the text. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the final version of the manuscript
-
[7]
The last mile: where artificial intelligence meets re- ality,
E. Coiera, “The last mile: where artificial intelligence meets re- ality,”Journal of medical Internet research, vol. 21, no. 11, p. e16323, 2019
2019
-
[8]
Radiology reporting, past, present, and future: the radiologist’s perspective,
B. I. Reiner, N. Knight, and E. L. Siegel, “Radiology reporting, past, present, and future: the radiologist’s perspective,”Journal of the American College of Radiology, vol. 4, no. 5, pp. 313–319, 2007
2007
-
[9]
V oice recognition for radiology reporting: is it good enough?
D. Rana, G. Hurst, L. Shepstone, J. Pilling, J. Cockburn, and M. Crawford, “V oice recognition for radiology reporting: is it good enough?”Clinical radiology, vol. 60, no. 11, pp. 1205– 1212, 2005
2005
-
[10]
V oice recognition technology for radiology re- porting: transforming the radiologist’s value proposition,
G. W. Boland, “V oice recognition technology for radiology re- porting: transforming the radiologist’s value proposition,”Journal of the American College of Radiology, vol. 4, no. 12, pp. 865–867, 2007
2007
-
[11]
Tethered to the ehr: pri- mary care physician workload assessment using ehr event log data and time-motion observations,
B. G. Arndt, J. W. Beasley, M. D. Watkinson, J. L. Temte, W.-J. Tuan, C. A. Sinsky, and V . J. Gilchrist, “Tethered to the ehr: pri- mary care physician workload assessment using ehr event log data and time-motion observations,”The Annals of Family Medicine, vol. 15, no. 5, pp. 419–426, 2017
2017
-
[12]
Physicians’ well-being linked to in-basket messages generated by algorithms in electronic health records,
M. Tai-Seale, E. C. Dillon, Y . Yang, R. Nordgren, R. L. Steinberg, T. Nauenberg, T. C. Lee, A. Meehan, J. Li, A. S. Chanet al., “Physicians’ well-being linked to in-basket messages generated by algorithms in electronic health records,”Health affairs, vol. 38, no. 7, pp. 1073–1078, 2019
2019
-
[13]
ASR error management for improving spoken language under- standing,
E. Simonnet, S. Ghannay, N. Camelin, Y . Est`eve, and R. de Mori, “ASR error management for improving spoken language under- standing,” inInterspeech 2017, 2017
2017
-
[14]
Improving the robustness of summarization systems with dual augmentation,
X. Chen, G. Long, C. Tao, M. Li, X. Gao, C. Zhang, and X. Zhang, “Improving the robustness of summarization systems with dual augmentation,” inProceedings of the 61st Annual Meeting of the Association for Computational Linguistics (Volume 1: Long Pa- pers), 2023, pp. 6846–6857
2023
-
[15]
Adversarial attacks on medical machine learn- ing,
S. G. Finlayson, J. D. Bowers, J. Ito, J. L. Zittrain, A. L. Beam, and I. S. Kohane, “Adversarial attacks on medical machine learn- ing,”Science, vol. 363, no. 6433, pp. 1287–1289, 2019
2019
-
[16]
WER is unaware: Assessing how asr errors distort clinical understanding in patient facing dialogue,
Z. Ellis, J. Joselowitz, Y . Deo, Y . He, A. Kalygina, A. Higham, M. Rahimzadeh, Y . Jia, I. Habli, and E. Lim, “WER is unaware: Assessing how asr errors distort clinical understanding in patient facing dialogue,” inProceedings of the 13th International Work- shop on Spoken Dialogue Systems Technology (IWSDS), 2026
2026
-
[17]
Speech model pre-Training for end-to-End spoken language understanding,
L. Lugosch, M. Ravanelli, P. Ignoto, V . S. Tomar, and Y . Ben- gio, “Speech model pre-Training for end-to-End spoken language understanding,” inInterspeech. ISCA, 2019
2019
-
[18]
Instruction-tuning LLaMA for synthetic medical note generation in swedish and english,
L. Kiefer, J. Alabi, T. Vakili, H. Dalianis, and D. Klakow, “Instruction-tuning LLaMA for synthetic medical note generation in swedish and english,” inProceedings of the 15th International Conference on Recent Advances in Natural Language Processing- Natural Language Processing in the Generative AI Era, 2025, pp. 557–566
2025
-
[19]
MEDSAGE: enhancing robustness of medical dialogue summarization to asr errors with llm-generated synthetic dialogues,
K. Binici, A. R. Kashyap, V . Schlegel, A. T. Liu, V . P. Dwivedi, T.-T. Nguyen, X. Gao, N. F. Chen, and S. Winkler, “MEDSAGE: enhancing robustness of medical dialogue summarization to asr errors with llm-generated synthetic dialogues,” inProceedings of the AAAI Conference on Artificial Intelligence, vol. 39, no. 22, 2025, pp. 23 496–23 504
2025
-
[20]
Is word error rate a good indicator for spoken language understanding accuracy,
Y .-Y . Wang, A. Acero, and C. Chelba, “Is word error rate a good indicator for spoken language understanding accuracy,” in2003 IEEE workshop on automatic speech recognition and understand- ing (IEEE Cat. No. 03EX721). IEEE, 2003, pp. 577–582
2003
-
[21]
Musan: A music, speech, and noise corpus,
D. Snyder, G. Chen, and D. Povey, “Musan: A music, speech, and noise corpus,”arXiv preprint arXiv:1510.08484, 2015
Pith/arXiv arXiv 2015
-
[22]
The diverse environments multi-channel acoustic noise database (demand): A database of multichannel environmental noise recordings,
J. Thiemann, N. Ito, and E. Vincent, “The diverse environments multi-channel acoustic noise database (demand): A database of multichannel environmental noise recordings,” inProceedings of Meetings on Acoustics, vol. 19, no. 1. Acoustical Society of America, 2013, p. 035081
2013
-
[23]
Beyond accu- racy: Behavioral testing of nlp models with checklist,
M. T. Ribeiro, T. Wu, C. Guestrin, and S. Singh, “Beyond accu- racy: Behavioral testing of nlp models with checklist,” inPro- ceedings of the 58th annual meeting of the association for compu- tational linguistics, 2020, pp. 4902–4912
2020
-
[24]
As- sessment of clinical competence using objective structured exam- ination
R. M. Harden, M. Stevenson, W. W. Downie, and G. Wilson, “As- sessment of clinical competence using objective structured exam- ination.”Br Med J, vol. 1, no. 5955, pp. 447–451, 1975
1975
-
[25]
An overview of the uses of standardized pa- tients for teaching and evaluating clinical skills. aamc,
H. S. Barrows, “An overview of the uses of standardized pa- tients for teaching and evaluating clinical skills. aamc,”Academic medicine, vol. 68, no. 6, pp. 443–51, 1993
1993
-
[26]
Informational and energetic masking effects in the perception of two simultaneous talkers,
D. S. Brungart, “Informational and energetic masking effects in the perception of two simultaneous talkers,”The Journal of the Acoustical Society of America, vol. 109, no. 3, pp. 1101–1109, 2001
2001
-
[27]
A study on data augmentation of reverberant speech for robust speech recognition,
T. Ko, V . Peddinti, D. Povey, M. L. Seltzer, and S. Khudanpur, “A study on data augmentation of reverberant speech for robust speech recognition,” in2017 IEEE international conference on acoustics, speech and signal processing (ICASSP). IEEE, 2017, pp. 5220–5224
2017
-
[28]
A dataset of simulated patient-physician medical interviews with a focus on respiratory cases,
F. Fareez, T. Parikh, C. Wavell, S. Shahab, M. Chevalier, S. Good, I. De Blasi, R. Rhouma, C. McMahon, J.-P. Lamet al., “A dataset of simulated patient-physician medical interviews with a focus on respiratory cases,”Scientific Data, vol. 9, no. 1, p. 313, 2022
2022
-
[29]
Robust speech recognition via large-scale weak supervision,
A. Radford, J. W. Kim, T. Xu, G. Brockman, C. McLeavey, and I. Sutskever, “Robust speech recognition via large-scale weak supervision,” inInternational conference on machine learning. PMLR, 2023, pp. 28 492–28 518
2023
-
[30]
A. Yang, A. Li, B. Yang, B. Zhang, B. Hui, B. Zheng, B. Yu, C. Gao, C. Huang, C. Lvet al., “Qwen3 technical report,”arXiv preprint arXiv:2505.09388, 2025
Pith/arXiv arXiv 2025
-
[31]
Towards conversational diagnostic artificial intelligence,
T. Tu, M. Schaekermann, A. Palepu, K. Saab, J. Freyberg, R. Tanno, A. Wang, B. Li, M. Amin, Y . Chenget al., “Towards conversational diagnostic artificial intelligence,”Nature, vol. 642, no. 8067, pp. 442–450, 2025
2025
-
[32]
A. Singh, A. Fry, A. Perelman, A. Tart, A. Ganesh, A. El-Kishky, A. McLaughlin, A. Low, A. Ostrow, A. Ananthramet al., “Openai gpt-5 system card,”arXiv preprint arXiv:2601.03267, 2025
Pith/arXiv arXiv 2025
-
[33]
G-eval: Nlg evaluation using gpt-4 with better human alignment,
Y . Liu, D. Iter, Y . Xu, S. Wang, R. Xu, and C. Zhu, “G-eval: Nlg evaluation using gpt-4 with better human alignment,” inProceed- ings of the 2023 conference on empirical methods in natural lan- guage processing, 2023, pp. 2511–2522
2023
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.