Female-RHINO: A Real-Time Scanner-Integrated Framework for Automated Quantitative Uterine MRI Analysis and Structured Reporting
Pith reviewed 2026-06-25 22:22 UTC · model grok-4.3
The pith
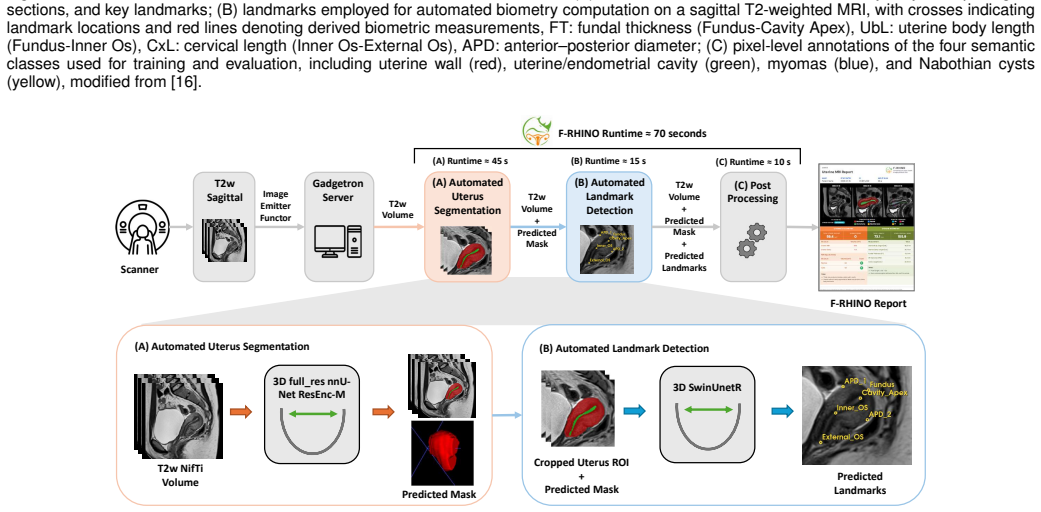
Female-RHINO connects deep learning models directly to MRI scanners to automate uterine segmentation, landmark detection, and structured reporting in under 70 seconds.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
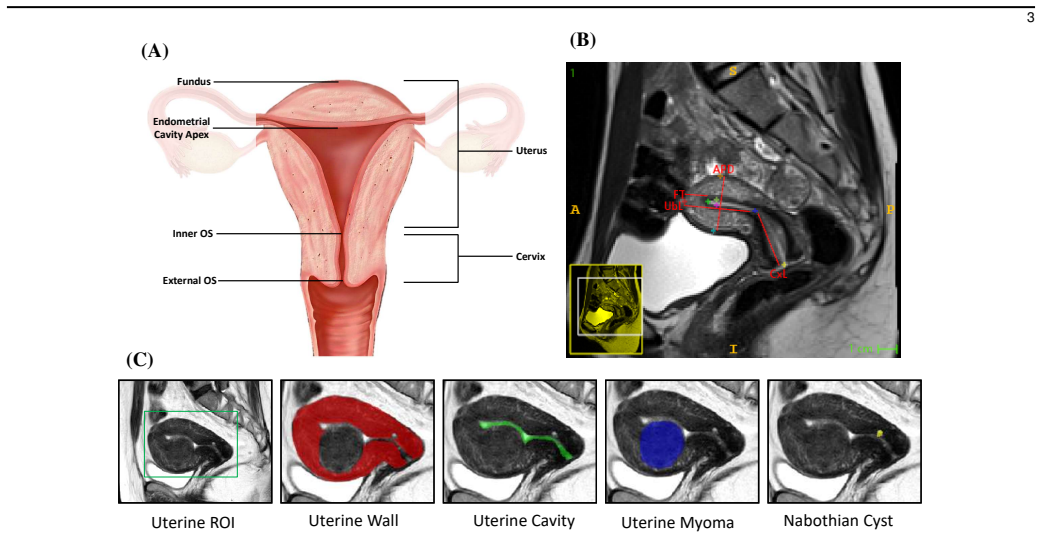
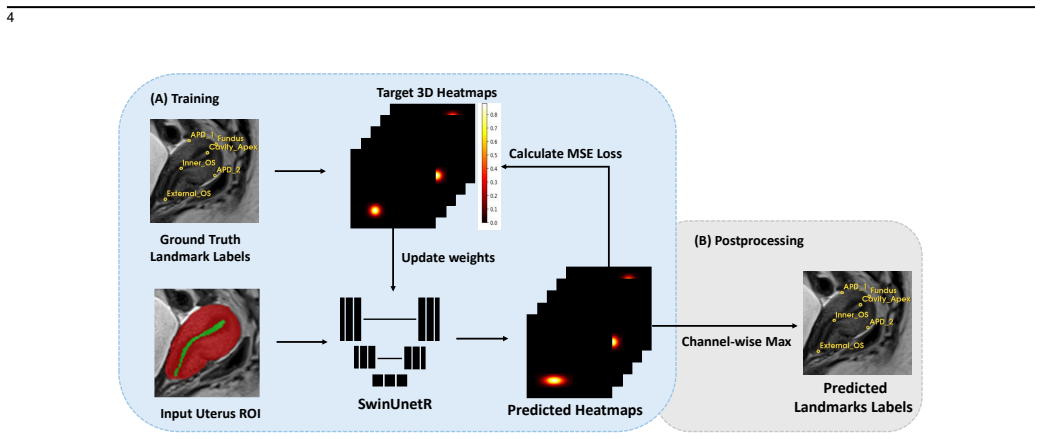
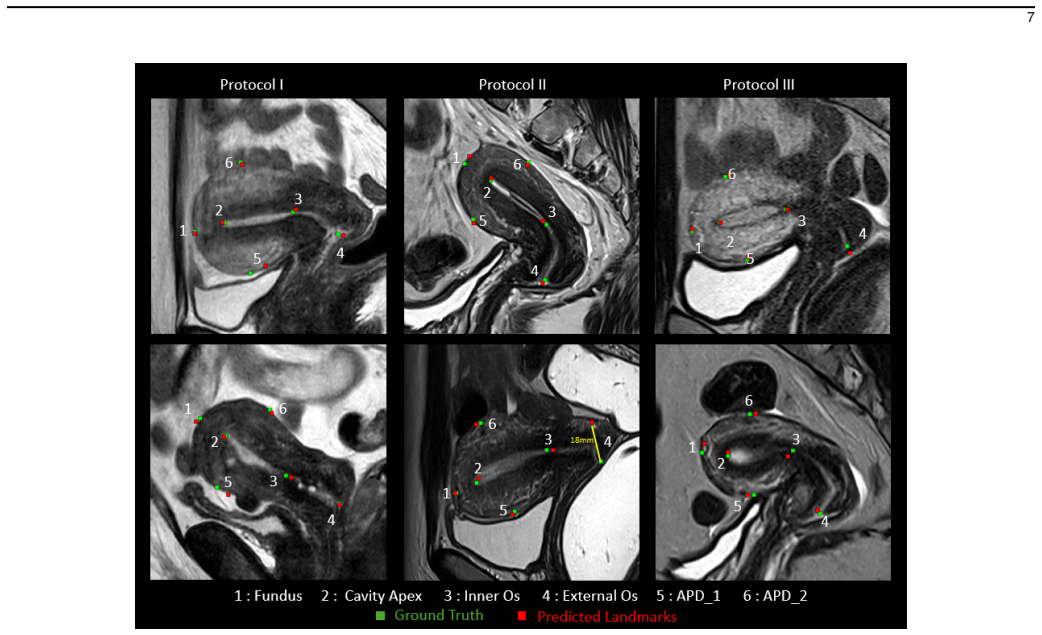
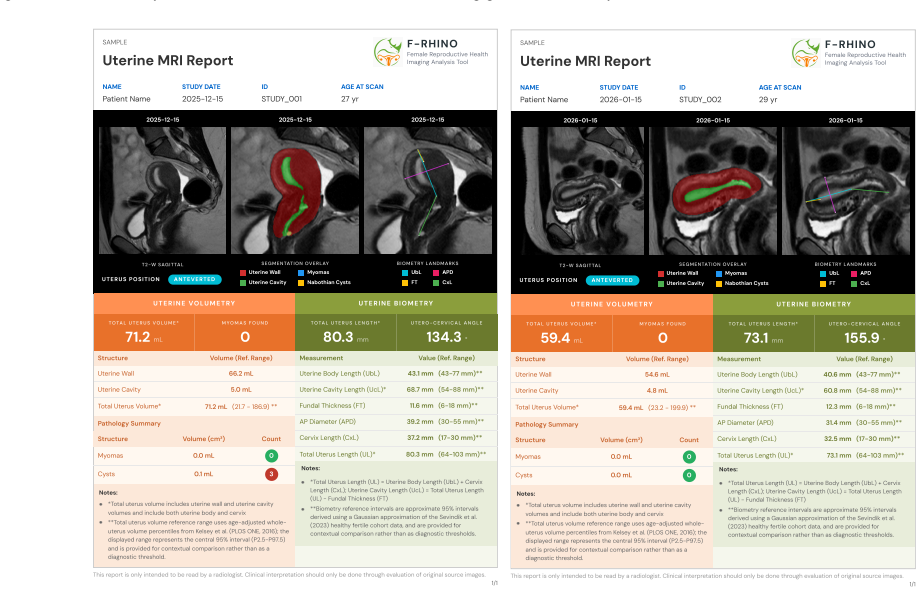
The framework combines segmentation and anatomical landmark detection models trained on more than 500 multi-center datasets to derive quantitative uterine biomarkers from sagittal T2-weighted pelvic MRI, detect and quantify fibroids and Nabothian cysts, extract six anatomical landmarks, and compile results into structured reports with visualizations, all completed in under 70 seconds during ongoing acquisition on independent retrospective and prospective cohorts.
What carries the argument
The inline scanner communication pipeline paired with deep learning models for uterus and fibroid segmentation, six-landmark detection, volumetry, and automated structured report generation.
If this is right
- Quantitative biomarkers and structured reports become available while the patient is still in the scanner.
- Analysis produces consistent results across diverse protocols, vendors, and patient populations.
- Incidental findings such as fibroids and Nabothian cysts are automatically detected and quantified.
- Structured reports with visualizations reduce manual interaction and observer dependence.
- Prospective deployment yields immediate, standardized, and reproducible analyses supported by inter-observer agreement.
Where Pith is reading between the lines
- The same scanner-integration pattern could be tested on MRI of other pelvic or abdominal structures to reduce total exam time.
- Longitudinal tracking of uterine volume or fibroid burden might become more feasible if the same pipeline is applied to follow-up scans.
- Sites with limited access to specialized readers could gain standardized biometric data that would otherwise require expert contouring.
- The six-landmark set might serve as a starting point for automated biometric indices that correlate with clinical outcomes in future studies.
Load-bearing premise
The deep learning models trained on more than 500 multi-center datasets will maintain the reported performance levels on new prospective deployments without substantial degradation due to protocol, vendor, or population differences.
What would settle it
A new prospective cohort on scanners from unseen vendors showing mean Dice scores below 0.70 for uterus segmentation or landmark radial error above 6 mm would falsify the robustness across acquisition settings.
Figures
read the original abstract
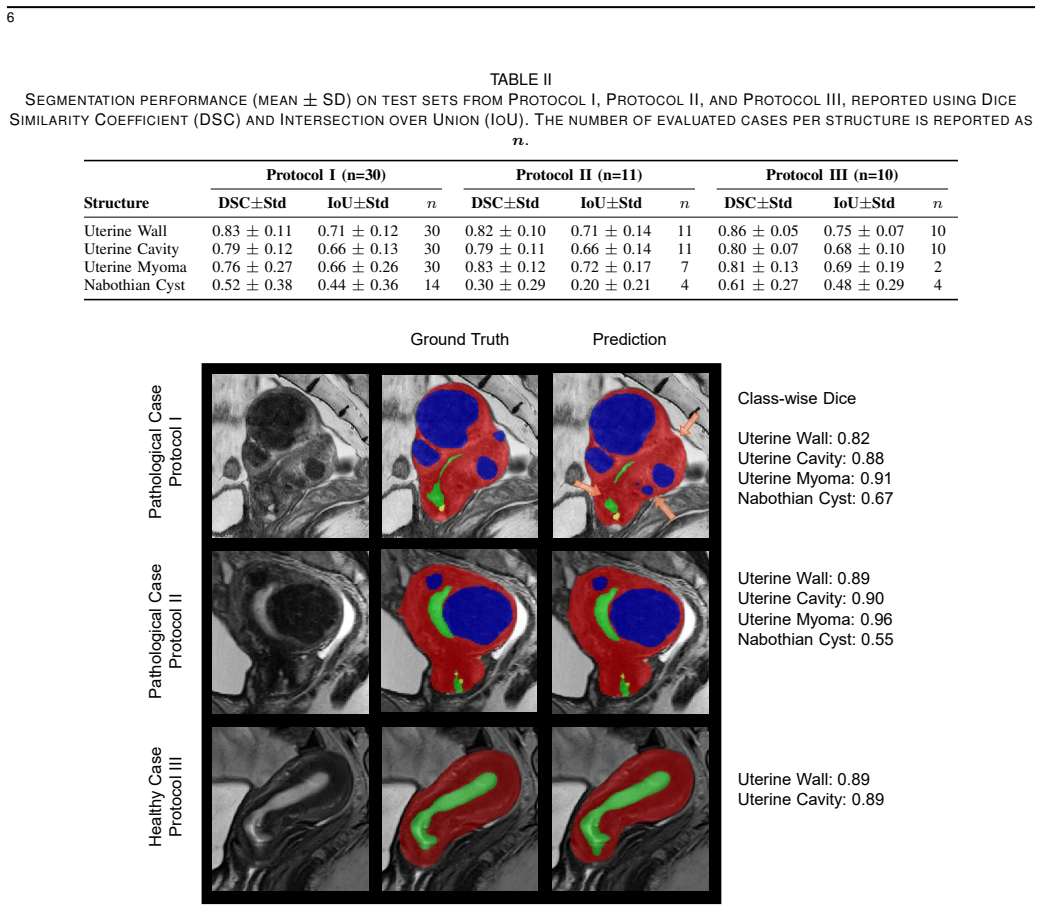
Standardized assessment of uterine MRI remains challenging due to anatomical variability, observer dependence, and the lack of workflow-integrated automated analysis tools. This work presents Female-RHINO: (R)eproductive (H)ealth (I)maging A(N)alysis T(O)ol, a real-time AI-assisted framework for automated quantitative uterine MRI analysis and structured reporting during image acquisition. We present an end-to-end system that integrates inline communication with the MRI scanner and deep learning-based analysis to derive quantitative uterine biomarkers from sagittal T2-weighted pelvic MRI. The framework combines segmentation and anatomical landmark detection models trained and evaluated on more than 500 multi-center datasets spanning diverse protocols, vendors, and patient populations. It performs volumetry, detects and quantifies common incidental findings such as fibroids and Nabothian cysts, and extracts six anatomical landmarks for biometric assessment. Results are compiled into a structured clinician-oriented report with integrated visualizations, without manual interaction. Evaluation on independent retrospective and prospective cohorts demonstrated robust performance across varying acquisition settings. Mean Dice similarity coefficients were 0.82 for the uterus and 0.80 for fibroids, with lower but consistent agreement for Nabothian cysts. Landmark detection achieved a mean radial error of 3.7 mm. End-to-end processing was completed in under 70 seconds, enabling availability of results during the ongoing scan. Prospective deployment yielded immediate, standardized, and reproducible analyses supported by inter-observer agreement. The proposed system enables real-time scanner-integrated AI for automated uterine MRI analysis and reporting, with potential to improve standardization, efficiency, and clinical workflow in pelvic imaging.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript presents Female-RHINO, a scanner-integrated real-time framework for automated quantitative analysis of sagittal T2-weighted uterine MRI. It combines deep-learning segmentation of the uterus and fibroids, landmark detection, quantification of incidental findings (fibroids, Nabothian cysts), and generation of structured reports. Models were trained on >500 multi-center datasets; evaluation on independent retrospective and prospective cohorts is reported to yield mean DSC 0.82 (uterus), 0.80 (fibroids), 3.7 mm mean radial landmark error, and end-to-end runtime <70 s, with prospective deployment producing immediate standardized outputs.
Significance. If the reported metrics and generalization hold, the work would represent a meaningful engineering contribution by delivering the first scanner-inline, fully automated, real-time quantitative uterine MRI pipeline with structured reporting. The combination of multi-center training, prospective evaluation, and sub-70-second latency directly addresses workflow integration, a recognized barrier in pelvic MRI standardization. Credit is due for the explicit prospective cohort testing and the end-to-end system description.
major comments (1)
- [Abstract / Results] Abstract and Results: the central robustness claim (performance maintained on independent prospective cohorts across acquisition settings) is load-bearing yet unsupported by any quantitative description of the distribution of field strength, vendor, sequence parameters, or patient demographics between training and test sets, nor by domain-shift metrics or subgroup performance tables. Without these, it is not possible to verify that the reported DSC and radial-error values demonstrate generalization rather than in-distribution performance.
Simulated Author's Rebuttal
We thank the referee for the constructive feedback and for recognizing the engineering contribution of the Female-RHINO framework. We address the single major comment below.
read point-by-point responses
-
Referee: [Abstract / Results] Abstract and Results: the central robustness claim (performance maintained on independent prospective cohorts across acquisition settings) is load-bearing yet unsupported by any quantitative description of the distribution of field strength, vendor, sequence parameters, or patient demographics between training and test sets, nor by domain-shift metrics or subgroup performance tables. Without these, it is not possible to verify that the reported DSC and radial-error values demonstrate generalization rather than in-distribution performance.
Authors: We acknowledge that the current manuscript provides only qualitative statements regarding multi-center diversity and reports performance on independent retrospective and prospective cohorts without quantitative breakdowns of field strength, vendor, sequence parameters, demographics, domain-shift metrics, or subgroup tables. While the training set of >500 cases spans multiple centers and the prospective evaluation occurred under real-world acquisition conditions, these details do not substitute for explicit distributions or analyses. In the revised manuscript we will add (i) a table of acquisition-parameter and demographic distributions across training, retrospective-test, and prospective cohorts, and (ii) subgroup performance metrics where sample sizes allow. This will enable readers to better evaluate the generalization claim. revision: yes
Circularity Check
No circularity; applied ML system description with empirical evaluation only
full rationale
The manuscript describes an end-to-end scanner-integrated DL framework for uterine segmentation, fibroid detection, landmark localization and structured reporting. Performance numbers (DSC 0.82/0.80, radial error 3.7 mm, <70 s runtime) are presented as direct empirical outcomes of training and testing on >500 multi-center cases plus independent retrospective/prospective cohorts. No equations, parameter-fitting steps, uniqueness theorems, or ansatzes are introduced; therefore none of the six enumerated circularity patterns can be instantiated. The central claim is an engineering performance assertion on held-out data, which remains externally falsifiable and does not reduce to its own inputs by construction.
Axiom & Free-Parameter Ledger
Reference graph
Works this paper leans on
-
[1]
MRI for adenomyosis: a pictorial review,
L. Agostinho, R. Cruz, F. Os ´orio, J. Alves, A. Set ´ubal, and A. Guerra, “MRI for adenomyosis: a pictorial review,”Insights Imaging, vol. 8, no. 6, pp. 549–556, Dec. 2017
2017
-
[2]
Preoperative diagnosis of cervical cystic lesions using magnetic resonance imaging: a retrospective study,
M. Omi, Y . O. Tanaka, N. Kurihara, Y . Sugiyama, A. Tonooka, M. Kanno, A. Fusegi, Y . Aoki, S. Netsu, A. Abe, T. Tanigawa, S. Okamoto, H. Nomura, and H. Kanao, “Preoperative diagnosis of cervical cystic lesions using magnetic resonance imaging: a retrospective study,”BMC Womens. Health, vol. 24, no. 1, p. 460, Aug. 2024
2024
-
[3]
Imaging of endometrial and cervical cancer,
S. Patel, S. H. Liyanage, A. Sahdev, A. G. Rockall, and R. H. Reznek, “Imaging of endometrial and cervical cancer,”Insights into imaging, vol. 1, pp. 309–328, 2010
2010
-
[4]
Magnetic resonance imaging evaluation of gynecological mass lesions: A comprehensive analysis with histopathological correlation,
S. Salman, N. Shireen, R. Riyaz, S. A. Khan, J. P. Singh, and A. Uttam, “Magnetic resonance imaging evaluation of gynecological mass lesions: A comprehensive analysis with histopathological correlation,”Medicine, vol. 103, no. 32, p. e39312, 2024
2024
-
[5]
Diagnostic accuracy of mri in the differential diagnosis between uterine leiomyomas and sarcomas: A systematic review and meta-analysis,
A. Raffone, D. Raimondo, D. Neola, A. Travaglino, M. Giorgi, L. Lazzeri, F. De Laurentiis, C. Carravetta, E. Zupi, R. Seracchioli, P. Casadio, and M. Guida, “Diagnostic accuracy of mri in the differential diagnosis between uterine leiomyomas and sarcomas: A systematic review and meta-analysis,”International Journal of Gynecology & Obstetrics, vol. 165, pp...
2024
-
[6]
Deep learning enables automated mri-based estimation of uterine volume also in patients with uterine fibroids undergoing high-intensity focused ultrasound therapy,
M. Theis, T. Tonguc, O. Savchenko, S. Nowak, W. Block, F. Recker, M. Essler, A. Mustea, U. Attenberger, M. Marinovaet al., “Deep learning enables automated mri-based estimation of uterine volume also in patients with uterine fibroids undergoing high-intensity focused ultrasound therapy,”Insights into Imaging, vol. 14, no. 1, p. 1, 2023. 10
2023
-
[7]
Outlier data in volume calculations of uterine fibroids comparing ellipsoid formula and voxel- based segmentation,
V . B´erczi, K. G. Turt ´oczki, S. Fazekas, A. Dolla-Tak ´acs, R. Stollmayer, P. N. Kaposi, I. Kalina, and B. K. Budai, “Outlier data in volume calculations of uterine fibroids comparing ellipsoid formula and voxel- based segmentation,”BMC Medical Imaging, vol. 25, pp. 1–8, 2025
2025
-
[8]
Uterine artery embolization of uterine leiomyomas: predictive mri features of volumetric response,
L. A. S. Kurban, H. Metwally, M. Abdullah, A. Kerban, A. Oulhaj, and J. A. Alkoteesh, “Uterine artery embolization of uterine leiomyomas: predictive mri features of volumetric response,”American Journal of Roentgenology, vol. 216, no. 4, pp. 967–974, 2021
2021
-
[9]
Differences in the anatomical structure of the uterus between fertile and infertile individuals,
B. Sevindik, N. Unver Dogan, O. Secilmis, E. Uysal, Z. Fazliogullari, and A. K. Karabulut, “Differences in the anatomical structure of the uterus between fertile and infertile individuals,”Clinical Anatomy, vol. 36, no. 5, p. 764, 2023
2023
-
[10]
Artifacts and pitfalls in MR imaging of the pelvis,
K. R. Zand, C. Reinhold, M. A. Haider, A. Nakai, L. Rohoman, and S. Maheshwari, “Artifacts and pitfalls in MR imaging of the pelvis,”J. Magn. Reson. Imaging, vol. 26, no. 3, pp. 480–497, Sep. 2007
2007
-
[11]
Uterine fibroids: current perspectives,
A. T. Khan, M. Shehmar, and J. K. Gupta, “Uterine fibroids: current perspectives,”International journal of women’s health, p. 95, 2014
2014
-
[12]
Epidemiology of uterine fibroids: a systematic review,
E. A. Stewart, C. Cookson, R. A. Gandolfo, and R. Schulze-Rath, “Epidemiology of uterine fibroids: a systematic review,”BJOG: An International Journal of Obstetrics & Gynaecology, vol. 124, no. 10, pp. 1501–1512, 2017
2017
-
[13]
Angle of uterine flexion and adenomyosis,
A. Xholli, U. Scovazzi, A. P. Londero, G. Evangelisti, E. Cavalli, M. G. Schiaffino, I. Vacca, F. Oppedisano, M. F. Ferraro, G. Sirito et al., “Angle of uterine flexion and adenomyosis,”Journal of clinical medicine, vol. 11, no. 11, p. 3214, 2022
2022
-
[14]
Structured vs narrative reporting of pelvic mri for fibroids: clarity and impact on treatment planning,
A. Franconeri, J. Fang, B. Carney, A. Justaniah, L. Miller, H.-C. Hur, L. P. King, R. Alammari, S. Faintuch, K. J. Morteleet al., “Structured vs narrative reporting of pelvic mri for fibroids: clarity and impact on treatment planning,”European radiology, vol. 28, no. 7, pp. 3009–3017, 2018
2018
-
[15]
Value of vaginal cervical position in estimating uterine anatomy,
U. Fidan, U. Keskin, M. Ulubay, M. ¨Ozt¨urk, and S. Bodur, “Value of vaginal cervical position in estimating uterine anatomy,”Clinical Anatomy, vol. 30, no. 3, pp. 404–408, 2017
2017
-
[16]
Large-scale uterine myoma mri dataset covering all figo types with pixel-level annotations,
H. Pan, M. Chen, W. Bai, B. Li, X. Zhao, M. Zhang, D. Zhang, Y . Li, H. Wang, H. Genget al., “Large-scale uterine myoma mri dataset covering all figo types with pixel-level annotations,”Scientific Data, vol. 11, no. 1, p. 410, 2024
2024
-
[17]
Intrauterine devices and uterine peristalsis: evaluation with MRI,
A. Kido, K. Togashi, M. L. Kataoka, A. Nakai, T. Koyama, and S. Fujii, “Intrauterine devices and uterine peristalsis: evaluation with MRI,”Magn. Reson. Imaging, vol. 26, no. 1, pp. 54–58, Jan. 2008
2008
-
[18]
Recommendations for mri technique in the evaluation of pelvic en- dometriosis: consensus statement from the society of abdominal ra- diology endometriosis disease-focused panel,
A. Tong, W. M. VanBuren, L. Chami ´e, M. Feldman, N. Hindman, C. Huang, P. Jha, A. Kilcoyne, S. Laifer-Narin, R. Nicolaet al., “Recommendations for mri technique in the evaluation of pelvic en- dometriosis: consensus statement from the society of abdominal ra- diology endometriosis disease-focused panel,”Abdominal Radiology, vol. 45, pp. 1569–1586, 2020
2020
-
[19]
Robust 3D landmark detection framework for one-stop automated pelvic MRI prescription,
T. Koike, A. Kudo, T. Fuchigami, A. Tachibana, A. Ikegawa, W. Yoko- hama, K. Sakuragi, Y . Kitamura, M. Hori, and N. Tomiyama, “Robust 3D landmark detection framework for one-stop automated pelvic MRI prescription,” inISMRM Annual Meeting, no. 1395. Concord, CA: ISMRM, 2025
2025
-
[20]
Automatic segmentation of the uterus on mri using a convolutional neural network,
Y . Kurata, M. Nishio, A. Kido, K. Fujimoto, M. Yakami, H. Isoda, and K. Togashi, “Automatic segmentation of the uterus on mri using a convolutional neural network,”Computers in biology and medicine, vol. 114, p. 103438, 2019
2019
-
[21]
A deep learning-based tool for analyzing the female reproductive system in MR images,
J. Khaghani, S. Basar, Y . Chodakiewitz, S. London, R. Attariwal, and S. Hashemi, “A deep learning-based tool for analyzing the female reproductive system in MR images,” inISMRM, 2024
2024
-
[22]
An AI-based solution for MR image analysis of the female reproductive system,
J. Khaghani, S. Khallaghi, S. Basar, Y . Chodakiewitz, R. Attariwala, and S. Hashemi, “An AI-based solution for MR image analysis of the female reproductive system,” inISMRM, Concord, CA, 2024
2024
-
[23]
Deep learning assisted detection and segmentation of uterine fibroids using multi-orientation magnetic resonance imaging,
X.-Y . Liu, Z.-L. Yuan, F.-Z. Cong, L. Mao, X.-L. Li, Z. Zhou, J. Ren, Y . Li, Y . Zhang, Y .-L. Heet al., “Deep learning assisted detection and segmentation of uterine fibroids using multi-orientation magnetic resonance imaging,”Abdominal Radiology, pp. 1–12, 2025
2025
-
[24]
Three-dimensional measurement of the uterus on magnetic resonance images: Development and performance analysis of an automated deep-learning tool,
D. Mulliez, E. Poncelet, L. Ferret, C. Hoeffel, B. Hamet, L. A. Dang, N. Laurent, and G. Ramette, “Three-dimensional measurement of the uterus on magnetic resonance images: Development and performance analysis of an automated deep-learning tool,”Diagnostics, vol. 13, no. 16, p. 2662, 2023
2023
-
[25]
Prototyping image reconstruction and analysis with fire,
K. Chow, P. Kellman, and H. Xue, “Prototyping image reconstruction and analysis with fire,” inSCMR, 2021
2021
-
[26]
Automatic flow planning for fetal cardiovascular magnetic resonance imaging,
S. N. Silva, T. Woodgate, S. McElroy, M. Cleri, K. St Clair, J. A. Verdera, K. Payette, A. Uus, L. Story, D. Lloydet al., “Automatic flow planning for fetal cardiovascular magnetic resonance imaging,”Journal of Cardiovascular Magnetic Resonance, vol. 27, no. 1, p. 101888, 2025
2025
-
[27]
Heron: High-efficiency real-time motion quantification and re-acquisition for fetal diffusion mri,
J. A. Verdera, A. Bortolazzi, S. N. Silva, K. Payette, K. S. Clair, S. McEl- roy, S. Malik, J. Hajnal, R. Tomi-Tricot, M. Rutherfordet al., “Heron: High-efficiency real-time motion quantification and re-acquisition for fetal diffusion mri,”IEEE Transactions on Medical Imaging, 2025
2025
-
[28]
Gadgetron inline ai: Effective model inference on mr scanner,
H. Xue, R. Davies, D. Hansen, E. Tseng, M. Fontana, J. C. Moon, and P. Kellman, “Gadgetron inline ai: Effective model inference on mr scanner,” inProceedings of the 27th Annual ISMRM Meeting and Exhibition, 2019, p. 4837
2019
-
[29]
Lessons learned during implementation of mr-guided high- intensity focused ultrasound treatment of uterine fibroids,
K. Anneveldt, I. Verpalen, I. Nijholt, J. Dijkstra, R. van den Hoed, M. van’t Veer-ten Kate, E. de Boer, J. van Osch, E. Heijman, H. Naber et al., “Lessons learned during implementation of mr-guided high- intensity focused ultrasound treatment of uterine fibroids,”Insights into Imaging, vol. 12, pp. 1–13, 2021
2021
-
[30]
Artificial intelligence for instance segmentation of mri: advancing efficiency and safety in laparoscopic myomectomy of broad ligament fibroids,
F. Liu, M. Chen, H. Pan, B. Li, and W. Bai, “Artificial intelligence for instance segmentation of mri: advancing efficiency and safety in laparoscopic myomectomy of broad ligament fibroids,”Frontiers in Oncology, vol. 15, p. 1549803, 2025
2025
-
[31]
Real-time automated analysis and reporting of uterine mri,
D. Bhatia, J. Aviles Verdera, M. Kitzberger, S. Tripathy, M. C. Bus- tos Vivas, L. Kratzsch, A. Knupfer, and J. Hutter, “Real-time automated analysis and reporting of uterine mri,” inSkin Image Analysis, and Computer-Aided Pelvic Imaging for Female Health. Springer Nature Switzerland, 2026, pp. 137–147
2026
-
[32]
The figo recommendations on terminologies and definitions for normal and abnormal uterine bleeding,
I. S. Fraser, H. O. Critchley, M. Broder, and M. G. Munro, “The figo recommendations on terminologies and definitions for normal and abnormal uterine bleeding,” inSeminars in reproductive medicine, vol. 29, no. 05. © Thieme Medical Publishers, 2011, pp. 383–390
2011
-
[33]
User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability,
P. A. Yushkevich, J. Piven, H. Cody Hazlett, R. Gimpel Smith, S. Ho, J. C. Gee, and G. Gerig, “User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability,” Neuroimage, vol. 31, no. 3, pp. 1116–1128, 2006
2006
-
[34]
nnu-net revisited: A call for rigorous validation in 3d medical image segmentation,
F. Isensee, T. Wald, C. Ulrich, M. Baumgartner, S. Roy, K. Maier-Hein, and P. F. Jaeger, “nnu-net revisited: A call for rigorous validation in 3d medical image segmentation,” inInternational Conference on Medical Image Computing and Computer-Assisted Intervention. Springer, 2024, pp. 488–498
2024
-
[35]
Swin unetr: Swin transformers for semantic segmentation of brain tumors in mri images,
A. Hatamizadeh, V . Nath, Y . Tang, D. Yang, H. R. Roth, and D. Xu, “Swin unetr: Swin transformers for semantic segmentation of brain tumors in mri images,” inBrainlesion, MICCAI. Springer, 2021, p. 272
2021
-
[36]
Pytorch: An imperative style, high-performance deep learning library,
A. Paszke, S. Gross, F. Massa, A. Lerer, J. Bradbury, G. Chanan, T. Killeen, Z. Lin, N. Gimelshein, L. Antigaet al., “Pytorch: An imperative style, high-performance deep learning library,”Advances in neural information processing systems, vol. 32, 2019
2019
-
[37]
A validated normative model for human uterine volume from birth to age 40 years,
T. W. Kelsey, E. Ginbey, M. M. Chowdhury, L. E. Bath, R. A. Anderson, and W. H. B. Wallace, “A validated normative model for human uterine volume from birth to age 40 years,”PloS one, vol. 11, no. 6, p. e0157375, 2016
2016
-
[38]
Study on the value of mri in locating the internal os of the cervix and influencing factors,
M. Liu, Y . Liang, X. Zheng, N. Mo, and E. Jin, “Study on the value of mri in locating the internal os of the cervix and influencing factors,” Scientific Reports, vol. 14, no. 1, p. 17784, 2024
2024
-
[39]
Wa-resunet: A focused tail class mri medical image segmentation algorithm,
H. Pan, B. Gao, W. Bai, B. Li, Y . Li, M. Zhang, H. Wang, X. Zhao, M. Chen, C. Yin, and W. Kong, “Wa-resunet: A focused tail class mri medical image segmentation algorithm,”Bioengineering, vol. 10, no. 8, p. 945, 2023
2023
-
[40]
An instance segmentation model based on deep learning for intelligent diagnosis of uterine myomas in mri,
H. Pan, M. Zhang, W. Bai, B. Li, H. Wang, H. Geng, X. Zhao, D. Zhang, Y . Li, and M. Chen, “An instance segmentation model based on deep learning for intelligent diagnosis of uterine myomas in mri,”Diagnostics, vol. 13, no. 9, p. 1525, 2023
2023
-
[41]
Metrics reloaded: recommendations for image analysis validation,
L. Maier-Hein, A. Reinke, P. Godau, M. D. Tizabi, F. Buettner, E. Christodoulou, B. Glocker, F. Isensee, J. Kleesiek, M. Kozubeket al., “Metrics reloaded: recommendations for image analysis validation,” Nature methods, vol. 21, no. 2, pp. 195–212, 2024
2024
-
[42]
Deep learning-based automated segmen- tation of uterine myomas,
T. J. Saleem and M. Yaqub, “Deep learning-based automated segmen- tation of uterine myomas,”arXiv, vol. abs/2508.11010, 2025
arXiv 2025
-
[43]
Integrating spatial configuration into heatmap regression based cnns for landmark localiza- tion,
C. Payer, D. ˇStern, H. Bischof, and M. Urschler, “Integrating spatial configuration into heatmap regression based cnns for landmark localiza- tion,”Medical image analysis, vol. 54, pp. 207–219, 2019
2019
-
[44]
Prior guided 3d medical image landmark localization,
Y . Pang, P. Cheng, J. Lyu, F. Lin, and X. Tang, “Prior guided 3d medical image landmark localization,” inMedical Imaging with Deep Learning. PMLR, 2024, pp. 1163–1175
2024
-
[45]
Differential diagnosis of cervical cystic lesions: Naboth- ian cyst, tunnel cluster, legh, mda,
J. Takahama, “Differential diagnosis of cervical cystic lesions: Naboth- ian cyst, tunnel cluster, legh, mda,” inMRI and CT for Decision-Making in Obstetrics and Gynecology Practice, N. Matsumura, M. Matsuki, and A. Kido, Eds. Springer, Singapore, 2025, pp. 223–230
2025
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.