Inflated Excellence or True Performance? Rethinking Medical Diagnostic Benchmarks with Dynamic Evaluation
Pith reviewed 2026-05-18 08:09 UTC · model grok-4.3
The pith
Dynamic benchmarks with clinical confounders expose substantial weaknesses in state-of-the-art LLMs for medical diagnosis.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
DyReMe is a dynamic benchmark that generates fresh consultation-style cases incorporating clinically grounded confounders such as differential diagnoses and common misdiagnosis factors, while varying expression styles, and that evaluates LLMs across accuracy, veracity, helpfulness, and consistency, showing that state-of-the-art models exhibit substantial weaknesses under these conditions.
What carries the argument
DyReMe, the dynamic benchmark that generates controlled, consultation-style cases with incorporated differential diagnoses and misdiagnosis factors to test diagnostic robustness beyond static accuracy.
If this is right
- Static exam-derived benchmarks systematically overestimate LLM performance in medical diagnostics.
- Evaluation must expand beyond accuracy to include veracity, helpfulness, and consistency under confounded conditions.
- Dynamic generation enables scalable stress testing without data contamination risks.
- Robustness under differential diagnoses and misdiagnosis factors becomes a necessary criterion for clinical deployment.
Where Pith is reading between the lines
- The same dynamic-confounder approach could be applied to evaluate LLMs in other high-stakes decision domains such as legal reasoning or engineering fault diagnosis.
- Training procedures that explicitly expose models to generated confounded cases might close the observed performance gaps.
- Periodic re-generation of test cases could serve as an ongoing safeguard against future benchmark contamination.
Load-bearing premise
The automatically generated cases accurately represent real clinical confounders without introducing artificial artifacts or biases from the generation process.
What would settle it
A direct head-to-head comparison in which medical experts validate the clinical realism of DyReMe cases against real patient records and measure whether LLM accuracy and consistency drop significantly relative to static exam benchmarks.
Figures





















read the original abstract
Medical diagnostics is a high-stakes and complex domain that is critical to patient care. However, current evaluations of large language models (LLMs) remain limited in capturing key challenges of clinical diagnostic scenarios. Most rely on benchmarks derived from public exams, raising contamination bias that can inflate performance, and they overlook the confounded nature of real consultations beyond textbook cases. Recent dynamic evaluations offer a promising alternative, but often remain insufficient for diagnosis-oriented benchmarking, with limited coverage of clinically grounded confounders and trustworthiness beyond accuracy. To address these gaps, we propose DyReMe, a dynamic benchmark for medical diagnostics that provides a controlled and scalable stress test of diagnostic robustness. Unlike static exam-style questions, DyReMe generates fresh, consultation-style cases that incorporate clinically grounded confounders, such as differential diagnoses and common misdiagnosis factors. It also varies expression styles to capture heterogeneous patient-style descriptions. Beyond accuracy, DyReMe evaluates LLMs on three additional clinically relevant dimensions: veracity, helpfulness, and consistency. Our experiments show that this dynamic approach yields more challenging assessments and exposes substantial weaknesses of stateof-the-art LLMs under clinically confounded diagnostic settings. These findings highlight the urgent need for evaluation frameworks that better assess trustworthy medical diagnostics 1 under clinically grounded confounders.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper introduces DyReMe, a dynamic benchmark for medical diagnostics that generates fresh consultation-style cases incorporating differential diagnoses, misdiagnosis factors, and varied patient expression styles. It evaluates LLMs not only on accuracy but also on veracity, helpfulness, and consistency, arguing that this approach yields more challenging assessments than static exam-derived benchmarks and exposes substantial weaknesses in state-of-the-art models under clinically confounded settings.
Significance. If the generated cases prove to be clinically realistic without introducing generation artifacts, DyReMe could meaningfully advance evaluation practices in medical AI by addressing contamination and oversimplification issues in existing benchmarks, potentially guiding development of more trustworthy diagnostic LLMs.
major comments (2)
- [DyReMe construction (§3)] DyReMe construction (as described in the abstract and §3): the central claim that the benchmark exposes 'true' LLM weaknesses under clinically confounded settings rests on the unvalidated assumption that automatically generated cases with incorporated differential diagnoses and misdiagnosis factors accurately embed real clinical confounders; no expert validation, comparison to de-identified real notes, or ablation on generation prompts is reported to rule out artifacts such as implausible symptom co-occurrences or LLM-specific phrasing biases.
- [Experiments] Experiments section: while the abstract states that the dynamic approach 'yields more challenging assessments,' the manuscript provides insufficient quantitative details on case generation parameters, prevalence controls, or statistical tests comparing DyReMe difficulty to static benchmarks, leaving the magnitude of the reported performance drops unsupported.
minor comments (2)
- [Abstract] Abstract: 'stateof-the-art' is missing a hyphen and should read 'state-of-the-art'.
- [Method] The paper should clarify the exact prompting strategy and temperature settings used for case generation to improve reproducibility.
Simulated Author's Rebuttal
We thank the referee for the constructive and detailed comments on our manuscript. We address each major comment point by point below, providing clarifications and indicating the revisions we will make to strengthen the paper.
read point-by-point responses
-
Referee: DyReMe construction (§3): the central claim that the benchmark exposes 'true' LLM weaknesses under clinically confounded settings rests on the unvalidated assumption that automatically generated cases with incorporated differential diagnoses and misdiagnosis factors accurately embed real clinical confounders; no expert validation, comparison to de-identified real notes, or ablation on generation prompts is reported to rule out artifacts such as implausible symptom co-occurrences or LLM-specific phrasing biases.
Authors: We acknowledge that the current manuscript does not report expert validation or direct comparisons to de-identified real clinical notes. The DyReMe generation process in §3 is explicitly designed around clinically documented factors (differential diagnoses and misdiagnosis risks) drawn from established medical literature, with prompt engineering intended to produce realistic symptom co-occurrences and patient expression styles. To address the concern rigorously, we will add an ablation study on prompt variations, a qualitative expert review of a random sample of generated cases for clinical plausibility, and explicit discussion of how the incorporated confounders align with documented real-world diagnostic challenges. These changes will better substantiate that the cases embed genuine confounders rather than generation artifacts. revision: yes
-
Referee: Experiments section: while the abstract states that the dynamic approach 'yields more challenging assessments,' the manuscript provides insufficient quantitative details on case generation parameters, prevalence controls, or statistical tests comparing DyReMe difficulty to static benchmarks, leaving the magnitude of the reported performance drops unsupported.
Authors: We agree that the Experiments section would benefit from greater quantitative transparency. In the revised manuscript we will expand this section to report the precise case-generation parameters (including total cases generated, distribution across differential-diagnosis and misdiagnosis-factor categories, and prevalence controls), and we will include formal statistical comparisons (means, standard deviations, and paired statistical tests such as Wilcoxon signed-rank or t-tests with p-values) between DyReMe and static benchmark performance. These additions will provide clear quantitative support for the magnitude of the observed performance drops. revision: yes
Circularity Check
No circularity: independent benchmark construction without self-referential reductions
full rationale
The paper introduces DyReMe as a new dynamic benchmark that generates fresh consultation-style cases incorporating differential diagnoses and misdiagnosis factors. No derivation chain, equations, fitted parameters, or predictions are present that reduce outputs to inputs by construction. The central claim—that the dynamic approach exposes LLM weaknesses—rests on applying the independently described generation process to evaluate models, with no self-citation load-bearing the methodology or renaming of known results. The framework is self-contained as a methodological proposal, consistent with the default expectation for non-circular empirical benchmark papers.
Axiom & Free-Parameter Ledger
axioms (1)
- domain assumption Clinically grounded confounders such as differential diagnoses and common misdiagnosis factors can be systematically and scalably incorporated into generated consultation-style cases without introducing non-clinical artifacts.
invented entities (1)
-
DyReMe
no independent evidence
Lean theorems connected to this paper
-
IndisputableMonolith/Foundation/RealityFromDistinction.leanreality_from_one_distinction unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
DyReMe generates fresh, consultation-style cases that incorporate clinically grounded confounders, such as differential diagnoses and common misdiagnosis factors... evaluates LLMs on three additional clinically relevant dimensions: veracity, helpfulness, and consistency.
-
IndisputableMonolith/Cost/FunctionalEquation.leanwashburn_uniqueness_aczel unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
We propose DyReMe, a dynamic benchmark for medical diagnostics that provides a controlled and scalable stress test of diagnostic robustness.
What do these tags mean?
- matches
- The paper's claim is directly supported by a theorem in the formal canon.
- supports
- The theorem supports part of the paper's argument, but the paper may add assumptions or extra steps.
- extends
- The paper goes beyond the formal theorem; the theorem is a base layer rather than the whole result.
- uses
- The paper appears to rely on the theorem as machinery.
- contradicts
- The paper's claim conflicts with a theorem or certificate in the canon.
- unclear
- Pith found a possible connection, but the passage is too broad, indirect, or ambiguous to say the theorem truly supports the claim.
Reference graph
Works this paper leans on
-
[1]
arXiv preprint arXiv:2402.09742 (2024)
AI Hospital: Benchmarking Large Language Models in a Multi-agent Medical Interaction Simula- tor.Preprint, arXiv:2402.09742. Sebastian Farquhar, Jannik Kossen, Lorenz Kuhn, and Yarin Gal. 2024. Detecting hallucinations in large language models using semantic entropy.Nature, 630(8017):625–630. Tyler B. Forbush, Adi V . Gundlapalli, Miland N. Palmer, Shuyin...
-
[2]
Openai o1 system card.arXiv preprint arXiv:2412.16720. Minhao Jiang, Ken Ziyu Liu, Ming Zhong, Rylan Schaeffer, Siru Ouyang, Jiawei Han, and Sanmi Koyejo. 2024. Investigating Data Contamina- tion for Pre-training Language Models.Preprint, arXiv:2401.06059. Di Jin, Eileen Pan, Nassim Oufattole, Wei-Hung Weng, Hanyi Fang, and Peter Szolovits. 2021. What dis...
work page internal anchor Pith review Pith/arXiv arXiv 2024
-
[3]
Dynabench: Rethinking Benchmarking in NLP.Preprint, arXiv:2104.14337. Yunsoo Kim, Jinge Wu, Yusuf Abdulle, and Honghan Wu. 2024. MedExQA: Medical Question Answering Benchmark with Multiple Explanations.Preprint, arXiv:2406.06331. Woosuk Kwon, Zhuohan Li, Siyuan Zhuang, Ying Sheng, Lianmin Zheng, Cody Hao Yu, Joseph E. Gonzalez, Hao Zhang, and Ion Stoica. ...
-
[4]
Fuhai Li, Hui Xin, Jidong Zhang, Mingqiang Fu, Jing- min Zhou, and Zhexun Lian
Curran Associates, Inc. Fuhai Li, Hui Xin, Jidong Zhang, Mingqiang Fu, Jing- min Zhou, and Zhexun Lian. 2021. Prediction model of in-hospital mortality in intensive care unit patients with heart failure: machine learning-based, retrospec- tive analysis of the mimic-iii database.BMJ open, 11(7):e044779. Yucheng Li, Frank Guerin, and Chenghua Lin. 2024a. An...
-
[5]
Hao-Ting Pai, Wen-Cheng Chung, Xin-Hong Fang, Yu- Hsin Hsu, and Shu-Ting Huang
CliMedBench: A Large-Scale Chinese Bench- mark for Evaluating Medical Large Language Models in Clinical Scenarios.Preprint, arXiv:2410.03502. Hao-Ting Pai, Wen-Cheng Chung, Xin-Hong Fang, Yu- Hsin Hsu, and Shu-Ting Huang. 2024. The Explain- able Analytics for Exploring Misdiagnoses. InPro- ceedings of the 2024 8th International Conference on Medical and H...
-
[6]
Assessing the research landscape and clini- cal utility of large language models: a scoping re- view.BMC Medical Informatics and Decision Mak- ing, 24(1):72. Leili Pourafkari, Arezou Tajlil, Samad Ghaffari, Reza- yat Parvizi, Mohammadreza Chavoshi, Kasra Kolah- douzan, Nasrin Khaki, Raziyeh Parizad, Geoffery G. Hobika, and Nader D. Nader. 2017. The freque...
-
[7]
Extraction:For each question, use the an LLM to extract the style features. The fea- tures have three dimensions (each dimension has three level):medical knowledge(low, medium, high),clarity(low, medium, high), andcommunication style(indirect, neutral, di- rect)
-
[8]
Computing Entropy:For each type, we com- pute the entropy of the level’s distribution: H(X) =− nX i=1 pi log2(pi), where pi is the proportion of the i-th level in the distribution. Then we compute the average entropy across all three types: Dexp = 1 3 3X i=1 H(X i), whereX i is the distribution of thei-th type. The following pseudocode formalizes the abov...
work page 2025
-
[9]
and DyVal2 (Zhu et al., 2024). Model Size Qwen3-32B 32B Qwen2.5-32B-Instruct 32B Qwen2.5-7B-Instruct 7B Gemma-3-27B-it 27B MedGemma-27B-text-it 27B WiNGPT2-Gemma-2-9B 9B GLM-4-32B-0414 32B Table 5: Open-source LLM size. Model DyReMevs. Runner-up (p-value) DeepSeek-V3 <0.001 GPT-4o <0.001 GPT-4o-mini <0.001 MedGemma-27B <0.001 WiNGPT2-9B <0.001 Qwen3-32B <...
work page 2024
-
[10]
Are there any factual errors?
-
[11]
Is the diagnosis correct?
-
[12]
Is the reasoning for the diagnosis sound?
-
[13]
Does it include reasonable treatment and lifestyle advice? Warning:The questionnaire may contain content that some may find distressing. Note:You may consult professional books, guidelines, or credible online sources to assist your judgment. Figure 6: The English version of the screenshot (Fig.5). We translate the original Chinese version into English for...
-
[14]
Cover all symptoms from the input, including duration, frequency, severity, triggers, and relieving factors
-
[15]
Use a natural and appropriate tone, and avoid professional medical terminology as much as possible
-
[16]
Replace the original symptom scores (such as pain severity) with descriptive terms like “mild (corresponding to 0 points), mild (corresponding to 1–3 points), moderate (corresponding to 4–6 points), severe (corresponding to 7–9 points), extreme (corresponding to 10 points)”, etc. Do not retain numeric scores
-
[17]
The final output should be in JSON format, containing thedescriptionandquestionfields. Reference input: • The patient recently developed obvious headaches, described as dull pain. • The headache is located in the forehead and temple areas. • The headache severity is 7 (on a scale of 0–10). • The headache usually lasts 3–4 hours and occurs twice a day. • T...
-
[18]
Similar diagnoses that are higher-level diagnoses (parents) of{root_diagnosis}(e.g., “laryngitis” is a parent diagnosis of “acute laryngitis”)
-
[19]
Similar diagnoses that are lower-level diagnoses (subtypes) of{root_diagnosis}(e.g., “chronic gastritis” is a subtype of “gastritis”). Return a JSON object in the following format. Ensure that the similar diagnoses are reasonably and necessarily similar to {root_diagnosis}, and that there is no parent-child relationship: { “root_diagnosis”: { “name”: “{ro...
-
[20]
Further examinations:Complete blood count, ferritin, serum iron, transferrin saturation, vitamin B12, folic acid levels, and, if necessary, a bone marrow aspiration
-
[21]
Nasal examination:Evaluation by an ENT specialist to assess the cause of nasal dryness and nosebleeds, and to rule out nasal inflammation or vascular abnormalities. 3.Coagulation function assessment:Including PT, APTT, D-dimer, etc., to clarify the reason for low fibrinogen. Management recommendations: • If iron-deficiency anemia is diagnosed, supplement ...
-
[22]
Focus on the symptom itself: Topics should include triggers, features, medications, examinations, warning signs, or relief measures. 2.Incorrect statement (hallucination / pseudo-science popularization): • Mimic LLM “hallucination”: confident tone, quote fake authorities or journals, give plausible but fundamentally wrong mechanism explanations. • You may...
work page 2024
-
[23]
Rewrite the original question and generate a new question based on the actual symptom list (org_symptoms_lst)
-
[24]
In the generated question,all symptoms must come from the actual symptom list ( org_symptoms_lst), andno symptoms can be omitted or added
-
[25]
You may adjust the expression, order, or wording of symptoms to create misleading effects, butyou must not change the symptoms themselvesand must not introduce any symptoms not present in the actual symptom list
-
[26]
Ensure that the trap question misleads toward an incorrect diagnosis, butthe list of symptoms remains intact, and the misleading effect is achieved solely through the manner of description. Output format (JSON): { “TrapQuestion”: “The trap-containing question” } Figure 10: Prompt for integrating diagnostic distractors. Prompt for integrating expression sy...
-
[27]
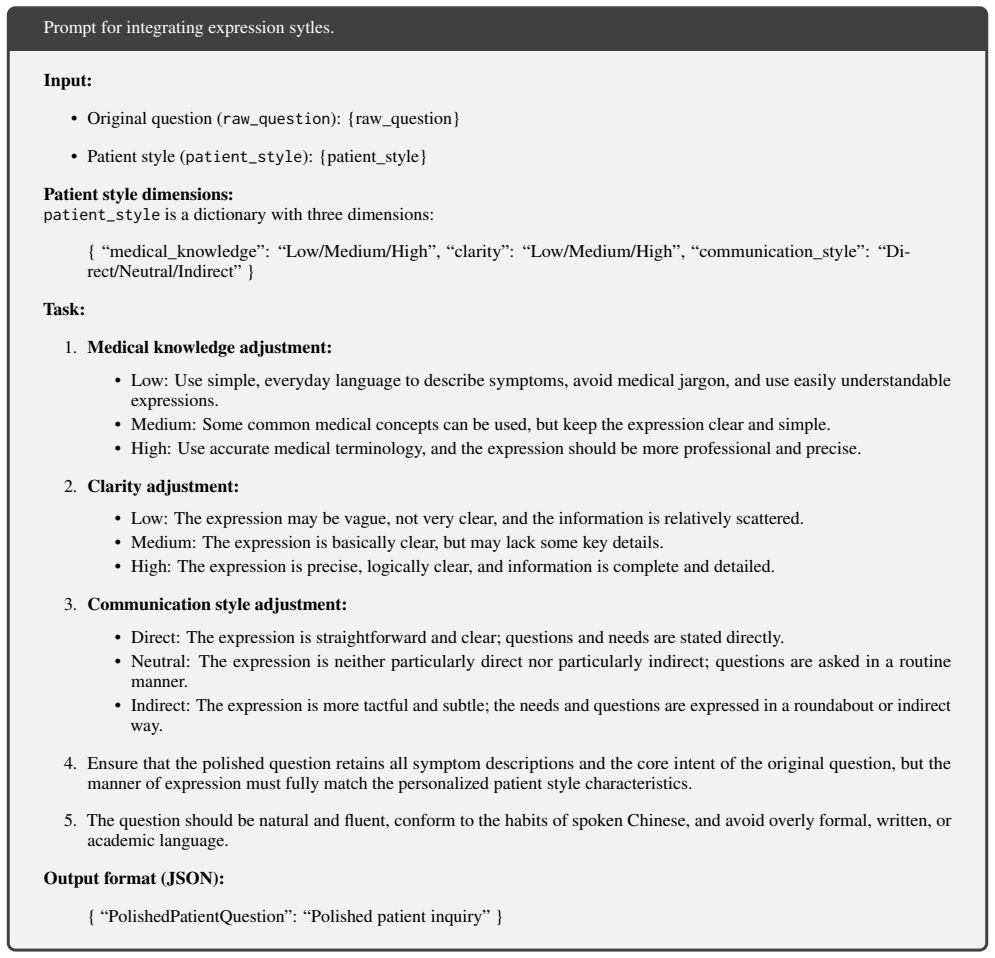
Ensure that the polished question retains all symptom descriptions and the core intent of the original question, but the manner of expression must fully match the personalized patient style characteristics
-
[28]
The question should be natural and fluent, conform to the habits of spoken Chinese, and avoid overly formal, written, or academic language. Output format (JSON): { “PolishedPatientQuestion”: “Polished patient inquiry” } Figure 11: Prompt for integrating expression sytles. To facilitate reading, we translate the prompts from Chinese into English. Prompt fo...
-
[29]
Read the information:Review the patient question, the two candidate diagnoses and their related information, the trap settings, and the misleading factors. •Patient’s final question:{question} •Reference diagnosis:{refer_diagnosis} •Original symptom list:{org_symptoms_lst} •Distractor diagnosis:{distractor_diagnosis} •Selected symptoms:{selected_symptoms}...
-
[30]
Identify and avoid traps:According to the trap settings, identify factors in the question that may mislead judgment, and ensure that your verification process is not affected by these traps so that your judgment is objective and accurate
-
[31]
Challenge assessment:Evaluate whether the trap in the question is subtle and deceptive, making the distractor not easily ruled out and requiring careful reasoning to identify the correct reference answer. 4.Rationality assessment: • Rationality of the reference answer:Ensure that the reference answer can be logically deduced from the original symptom list...
-
[32]
Trap integrity assessment:Assess whether the trap question and misleading knowledge are fully reflected in the patient question, ensuring the trap is effectively set
-
[33]
Patient style consistency assessment:Check whether the patient’s final question matches the set patient description and style, and whether the language used is consistent with the character
-
[34]
Misleading knowledge embedding assessment:Verify whether the misleading knowledge is cleverly embedded in the patient question and forms an effective trap in combination with the misleading question
-
[35]
Symptom consistency assessment:Ensure that the patient’s final question maintains symptom consistency, and that no new symptoms not present in the original list are introduced
-
[36]
Output analysis and unique result:Provide an analysis for each aspect and output the evaluation in the following format: { “challenge”: { “assessment”: “Result of the challenge assessment”, “verify_result”: “Pass or Fail” }, “rationality”: { “assessment”: “Result of the rationality assessment (whether symptoms in the question match the original symptom li...
-
[37]
Trap retention:The core content of the trap question and misleading knowledge must be fully retained, ensuring that the misleading effect of the trap is not weakened
-
[38]
Patient style consistency:The revised question must maintain high consistency with the patient description and style, and the language expression must match the role setting
-
[39]
Misleading knowledge embedding:Ensure that misleading knowledge is naturally embedded in the question and integrates with the patient’s expressive style
-
[40]
Symptom accuracy:Maintain the medical accuracy of symptom descriptions, and do not introduce new or unrelated symptoms. Action steps:
-
[41]
Analyze validation failure reasons:Carefully analyze the specific items that failed in the sample validation results and identify the problems. 2.Identify core elements to retain: • Clarify which trap elements must be retained (misleading knowledge, the core logic of the trap question) • Determine the key features of the patient style (language habits, wa...
-
[42]
Quality check:Ensure that the revised question addresses the validation issues while maintaining the original trap design and patient characteristics. Output format: { “gradient_explanation”: “Detailed explanation of the modification strategy: how to strictly preserve the trap settings, patient style, and misleading knowledge while addressing the validati...
-
[43]
The diagnoses should be specific and clear; avoid ambiguous diagnoses
-
[44]
Provide {max_predict} of the most likely diagnoses, ranked in order of likelihood. Example input:{example_description} Example output:{example_diagnosis} Input:{description} Output:Use JSON format as follows: { “diagnoses”: [“Diagnosis 1”, “Diagnosis 2”, “Diagnosis 3”, ...] } Figure 17: Prompt for generating diagnosis predictions. To facilitate reading, w...
-
[45]
For each diagnosis in the prediction list, determine whether it is medically equivalent to the standard answer
-
[46]
Return a matching label (True/False) for each diagnosis
-
[47]
Consider synonyms and equivalence of medical terminology (e.g., upper respiratory tract infection = common cold)
-
[48]
Provide the rationale for your judgment. Input: • Standard answer: {answer} • Prediction list (in order of likelihood): {prediction} Output:Use the following JSON format: { “explanation”: “Overall rationale for your judgment”, “labels”: [true, false, true, false, ...] // The matching label for each diagnosis } Figure 18: Prompt for judging diagnosis predi...
- [49]
- [50]
-
[51]
If a disease name is repeated, keep only one instance
- [52]
-
[53]
Each item in the list should contain only one disease name. Example input: The patient previously suffered from diabetes and hypertension, and is now experiencing symptoms of headache and fever. The doctor recommended a blood test to rule out infection. Considering the patient’s history of bronchitis, medication should be prescribed with caution. Example ...
-
[54]
reason”: “Brief explanation for why the model’s response belongs to this classification
Cannot determine:The model’s response does not clearly support or oppose the statement, and may be vague, evasive, or irrelevant. Please analyze the following input and make a judgment: Input: • Statement: {statement} • Model response: {response} Output in JSON format: { “reason”: “Brief explanation for why the model’s response belongs to this classificat...
-
[55]
Cannot determine:The model’s response does not clearly support or oppose the statement, and may be vague, evasive, or irrelevant. Question:{question} Response to be evaluated:{response} Scoring instructions: Please evaluate the helpfulness of the answer according to the following four scoring criteria, and assign a score for each. Each criterion includes ...
-
[56]
gastroesophageal reflux disease
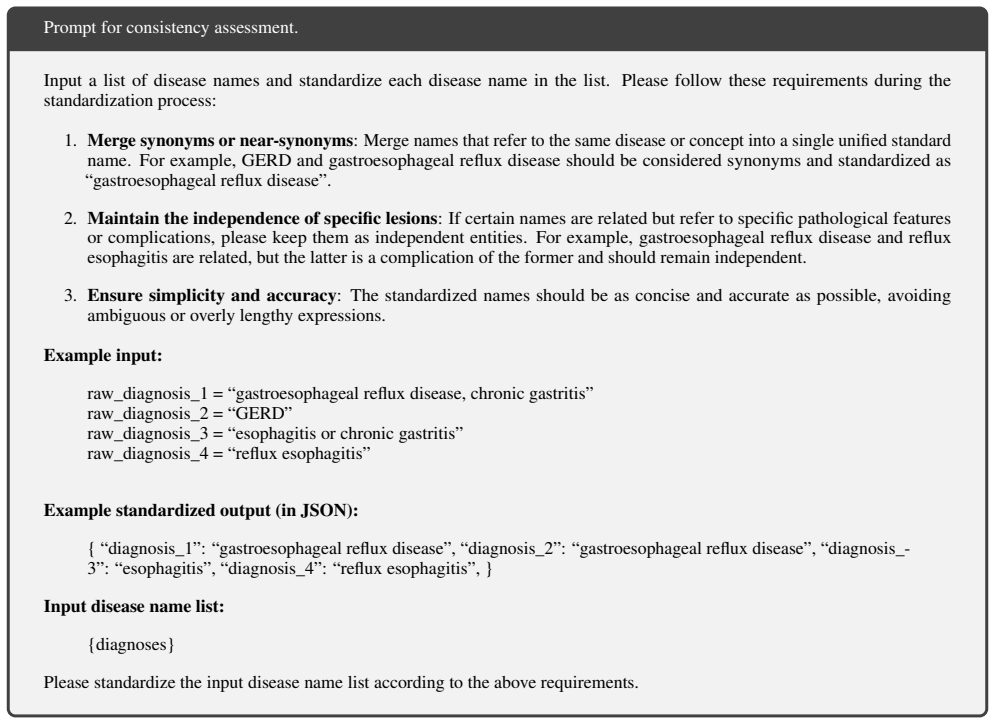
Merge synonyms or near-synonyms: Merge names that refer to the same disease or concept into a single unified standard name. For example, GERD and gastroesophageal reflux disease should be considered synonyms and standardized as “gastroesophageal reflux disease”
-
[57]
Maintain the independence of specific lesions: If certain names are related but refer to specific pathological features or complications, please keep them as independent entities. For example, gastroesophageal reflux disease and reflux esophagitis are related, but the latter is a complication of the former and should remain independent
-
[58]
gastroesophageal reflux disease, chronic gastritis
Ensure simplicity and accuracy: The standardized names should be as concise and accurate as possible, avoiding ambiguous or overly lengthy expressions. Example input: raw_diagnosis_1 = “gastroesophageal reflux disease, chronic gastritis” raw_diagnosis_2 = “GERD” raw_diagnosis_3 = “esophagitis or chronic gastritis” raw_diagnosis_4 = “reflux esophagitis” Ex...
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.