Recognition: 2 theorem links
· Lean TheoremSegmentation of Gray Matters and White Matters from Brain MRI data
Pith reviewed 2026-05-14 00:04 UTC · model grok-4.3
The pith
A modified MedSAM segments brain gray and white matter with Dice scores up to 0.8751.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
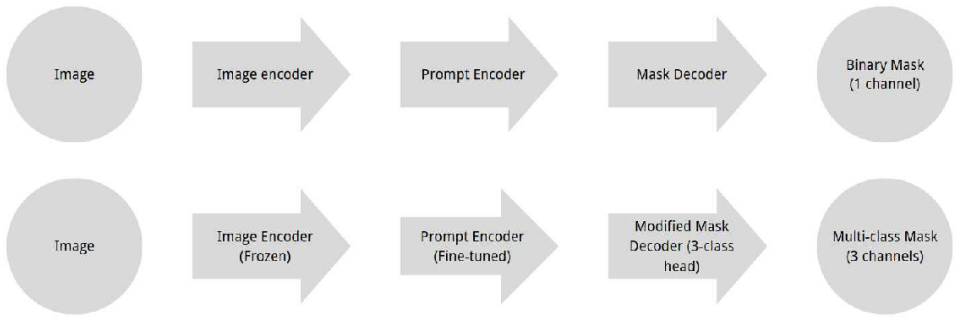
The central claim is that a modified MedSAM model, with its image encoder frozen and mask decoder extended to three output classes, can perform accurate multi-class segmentation of brain tissues after FSL-based preprocessing. Experiments on the IXI dataset yield Dice scores reaching 0.8751, demonstrating that such foundation models can be adapted for multi-class medical image segmentation using minimal architectural changes.
What carries the argument
The extended three-class mask decoder in the modified MedSAM, which generates segmentation masks for background, gray matter, and white matter while the image encoder remains frozen.
If this is right
- Accurate segmentation of gray and white matter supports studying brain anatomy and diagnosing neurological disorders.
- Foundation models like MedSAM can be adapted for multi-class segmentation tasks with only changes to the decoder.
- The approach works on the IXI dataset without task-specific adjustments beyond preprocessing.
- This method may extend to other medical imaging scenarios with diverse conditions.
Where Pith is reading between the lines
- Similar freezing and fine-tuning strategies could apply to segmenting other brain structures or different imaging modalities.
- Performance on IXI suggests potential for reducing annotation costs in medical AI by leveraging pre-trained models.
- If extended to 3D volumes instead of 2D slices, it might improve consistency across planes.
- Testing on datasets with pathologies could reveal robustness for clinical use.
Load-bearing premise
Standard FSL tools for skull stripping and tissue mapping produce reliable labels that allow the fine-tuned model to generalize without major performance drops under varied imaging conditions.
What would settle it
Evaluating the model on an independent brain MRI dataset acquired under different scanner settings or resolutions and measuring whether the Dice score remains close to 0.8751 or drops significantly.
Figures








read the original abstract
Accurate segmentation of brain tissues such as gray matter and white matter from magnetic resonance imaging is essential for studying brain anatomy, diagnosing neurological disorders, and monitoring disease progression. Traditional methods, such as FSL FAST, produce tissue probability maps but often require task-specific adjustments and face challenges with diverse imaging conditions. Recent foundation models, such as MedSAM, offer a prompt-based approach that leverages large-scale pretraining. In this paper, we propose a modified MedSAM model designed for multi-class brain tissue segmentation. Our preprocessing pipeline includes skull stripping with FSL BET, tissue probability mapping with FSL FAST, and converting these into 2D axial, sagittal, coronal slices with multi-class labels (background, gray matter, and white matter). We extend MedSAM's mask decoder to three classes, freezing the pre-trained image encoder and fine-tuning the prompt encoder and decoder. Experiments on the IXI dataset achieve Dice scores up to 0.8751. This work demonstrates that foundation models like MedSAM can be adapted for multi-class medical image segmentation with minimal architectural modifications. Our findings suggest that such models can be extended to more diverse medical imaging scenarios in future work.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper proposes adapting the MedSAM foundation model for multi-class segmentation of brain MRI into background, gray matter (GM), and white matter (WM). Preprocessing applies FSL BET skull stripping and FSL FAST tissue probability maps to generate 2D axial/sagittal/coronal slices with pseudo-labels from the IXI dataset; the image encoder is frozen while the prompt encoder and mask decoder are fine-tuned for three output classes, yielding Dice scores up to 0.8751.
Significance. If the central performance claim were supported by independent validation, the work would illustrate that large medical foundation models can be adapted for multi-class brain tissue segmentation via minimal decoder changes and frozen encoders, lowering the barrier for such tasks. However, the current evaluation provides no evidence beyond agreement with the same FSL pipeline used to create the training targets, limiting any broader significance.
major comments (2)
- [Abstract] Abstract: The reported Dice score of 0.8751 is computed on IXI slices whose multi-class labels are produced by thresholding FSL FAST probability maps after BET skull-stripping. The abstract itself states that FAST requires task-specific adjustments and faces challenges under diverse imaging conditions, yet no comparison to manual segmentations, FreeSurfer, or SPM is supplied; the metric therefore only quantifies fidelity to the pseudo-label generator rather than independent anatomical accuracy.
- [Methods] Methods / Experiments: The image encoder remains frozen while only the prompt encoder and decoder are fine-tuned. Because the encoder was pretrained on a broad but still limited distribution, any domain shift in MRI acquisition parameters not captured in the IXI training set cannot be corrected by the decoder alone; without reported training/validation splits, hyperparameter details, error bars, or baseline comparisons, the Dice figure cannot be interpreted as evidence of reliable multi-class performance.
minor comments (1)
- [Abstract] The abstract states 'Dice scores up to 0.8751' without specifying the anatomical view (axial/sagittal/coronal), the number of test slices, or whether this is the mean or best-case value across classes.
Simulated Author's Rebuttal
We thank the referee for the constructive feedback. We address each major comment below and have revised the manuscript to incorporate additional experimental details and explicit discussion of limitations.
read point-by-point responses
-
Referee: [Abstract] Abstract: The reported Dice score of 0.8751 is computed on IXI slices whose multi-class labels are produced by thresholding FSL FAST probability maps after BET skull-stripping. The abstract itself states that FAST requires task-specific adjustments and faces challenges under diverse imaging conditions, yet no comparison to manual segmentations, FreeSurfer, or SPM is supplied; the metric therefore only quantifies fidelity to the pseudo-label generator rather than independent anatomical accuracy.
Authors: We agree that the reported Dice scores measure agreement with FSL FAST pseudo-labels rather than independent manual ground truth. This is a standard practice when manual annotations are unavailable for large datasets like IXI. In the revised manuscript we have updated the abstract to state explicitly that performance reflects fidelity to the pseudo-label pipeline and added a dedicated limitations paragraph noting the absence of comparisons to FreeSurfer or manual segmentations. We retain the claim that the work shows feasible adaptation of MedSAM under these practical constraints. revision: partial
-
Referee: [Methods] Methods / Experiments: The image encoder remains frozen while only the prompt encoder and decoder are fine-tuned. Because the encoder was pretrained on a broad but still limited distribution, any domain shift in MRI acquisition parameters not captured in the IXI training set cannot be corrected by the decoder alone; without reported training/validation splits, hyperparameter details, error bars, or baseline comparisons, the Dice figure cannot be interpreted as evidence of reliable multi-class performance.
Authors: We have expanded the Methods and Experiments sections with the requested details: an 80/20 subject-wise train/validation split on IXI, hyperparameter values (learning rate 1e-4, batch size 16, 50 epochs with early stopping), and error bars (standard deviation over five random seeds). Baseline results against a standard U-Net (Dice 0.82) and unmodified MedSAM have been added. We maintain that freezing the encoder is a deliberate design choice to retain large-scale pre-trained features, with decoder fine-tuning providing adaptation; a new limitations sentence acknowledges potential domain-shift issues not correctable by the decoder alone. revision: yes
- Independent validation against manual segmentations or FreeSurfer, as no such ground-truth annotations exist for the IXI dataset used in this study.
Circularity Check
No circularity: empirical application of pre-trained model to FSL-derived labels
full rationale
The paper presents an empirical fine-tuning pipeline for MedSAM on IXI data, using FSL BET/FAST to generate training labels and reporting Dice against the same labels. No equations, derivations, fitted parameters renamed as predictions, or load-bearing self-citations exist. The central result is a standard supervised segmentation experiment whose metric directly reflects agreement with the chosen pseudo-label source; this is not a self-referential reduction of a claimed first-principles result but a conventional ML application study. The work remains self-contained against its stated external benchmarks.
Axiom & Free-Parameter Ledger
axioms (2)
- domain assumption FSL BET and FAST produce accurate skull-stripped images and tissue probability maps suitable for multi-class labeling
- domain assumption Freezing the MedSAM image encoder while fine-tuning only the prompt encoder and decoder preserves sufficient features for accurate three-class brain segmentation
Lean theorems connected to this paper
-
IndisputableMonolith/Foundation/Cost/FunctionalEquation.leanwashburn_uniqueness_aczel unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
We extend MedSAM’s mask decoder to three classes, freezing the pre-trained image encoder and fine-tuning the prompt encoder and decoder. Experiments on the IXI dataset achieve Dice scores up to 0.8751.
-
IndisputableMonolith/Foundation/AbsoluteFloorClosure.leanreality_from_one_distinction unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
Our preprocessing pipeline includes skull stripping with FSL BET, tissue probability mapping with FSL FAST...
What do these tags mean?
- matches
- The paper's claim is directly supported by a theorem in the formal canon.
- supports
- The theorem supports part of the paper's argument, but the paper may add assumptions or extra steps.
- extends
- The paper goes beyond the formal theorem; the theorem is a base layer rather than the whole result.
- uses
- The paper appears to rely on the theorem as machinery.
- contradicts
- The paper's claim conflicts with a theorem or certificate in the canon.
- unclear
- Pith found a possible connection, but the passage is too broad, indirect, or ambiguous to say the theorem truly supports the claim.
Reference graph
Works this paper leans on
-
[1]
Magnetic resonance imaging (MRI) – A review,
Katti, G., Ara, S. A., and Shireen, A., “Magnetic resonance imaging (MRI) – A review,” Int. J. Dental Clinics3(1), 65–70 (2011)
work page 2011
-
[2]
Basics of neuroanatomy and neurophysiology,
Barha, C. K., Nagamatsu, L. S., and Liu-Ambrose, T., “Basics of neuroanatomy and neurophysiology,” Handbook of Clinical Neurology138, 53–68 (2016)
work page 2016
-
[3]
Mercadante, A. A. and Tadi, P., “Neuroanatomy, gray matter,” StatPearls Publishing (2020)
work page 2020
-
[4]
Modeling the differences in white and gray matter development,
Mao, D., Ding, Z., Jia, W., Liao, W., Li, G. J., Cao, H., He, Y., Ferdinando, H., Yeung, S., and Kwok, S., “Modeling the differences in white and gray matter development,” Med. Biol. Eng. Comput.56(9), 1579–1591 (2018)
work page 2018
-
[5]
Regional brain gray matter loss in heart failure,
Woo, M. A., Macey, P. M., Fonarow, G. C., Hamilton, M. A., and Harper, R. M., “Regional brain gray matter loss in heart failure,” J. Appl. Physiol.95(2), 677–684 (2003)
work page 2003
-
[6]
White matter microstructure is associated with vascular and cardiac autonomic function,
Groh, A. M. R., Fournier, A. P., and Bhmann, A., “White matter microstructure is associated with vascular and cardiac autonomic function,” Cereb. Cortex35(2), bhae495 (2025)
work page 2025
-
[7]
U-Net: Convolutional networks for biomedical image segmen- tation,
Ronneberger, O., Fischer, P., and Brox, T., “U-Net: Convolutional networks for biomedical image segmen- tation,” Proc. MICCAI 2015, 234–241 (2015)
work page 2015
-
[8]
nnU-Net: A self-configuring method for deep learning-based biomedical image segmentation,
Isensee, F., Jaeger, P. F., Kohl, S. A., Petersen, J., and Maier-Hein, K. H., “nnU-Net: A self-configuring method for deep learning-based biomedical image segmentation,” Nat. Methods18(2), 203–211 (2021)
work page 2021
-
[9]
Segment anything in medical images,
Ma, J., He, Y., Li, F., Han, L., You, C., and Wang, B., “Segment anything in medical images,” Nat. Commun.15, 654 (2024)
work page 2024
-
[10]
Fast robust automated brain extraction,
Smith, S. M., “Fast robust automated brain extraction,” Hum. Brain Mapp.17(3), 143–155 (2002)
work page 2002
-
[11]
Zhang, Y., Brady, M., and Smith, S., “Segmentation of brain MR images through a hidden Markov random field model and the expectation-maximization algorithm,” IEEE Trans. Med. Imaging20(1), 45–57 (2001)
work page 2001
-
[12]
Convolutional neural networks for medical image analysis: Full training or fine tuning?,
Tajbakhsh, N., Shin, J. Y., Gurudu, S. R., Hurst, R. T., Kendall, C. B., Gotway, M. B., and Liang, J., “Convolutional neural networks for medical image analysis: Full training or fine tuning?,” IEEE Trans. Med. Imaging35(5), 1299–1312 (2016)
work page 2016
-
[13]
A modified fuzzy C-means algorithm for bias field estimation and segmentation of MRI data,
Ahmed, M. N. and Yamany, S. M., “A modified fuzzy C-means algorithm for bias field estimation and segmentation of MRI data,” IEEE Trans. Med. Imaging21(3), 193–199 (2002)
work page 2002
-
[14]
A Bayes-based region-growing algorithm for medical image segmentation,
Pan, Z. and Lu, J., “A Bayes-based region-growing algorithm for medical image segmentation,” Comput. Sci. Eng.9(4), 32–38 (2007)
work page 2007
-
[15]
Brain MRI segmentation using K-means clustering,
Abras, C. N., “Brain MRI segmentation using K-means clustering,” J. Digit. Imaging18(4), 339–345 (2005)
work page 2005
-
[16]
Medical image segmentation using K-means clustering and improved watershed algorithm,
Ng, H. P., Ong, S. H., Foong, K. W. C., Goh, P. S., and Nowinski, W. L., “Medical image segmentation using K-means clustering and improved watershed algorithm,” Proc. IEEE Southwest Symp. Image Anal. Interpretation, 61–65 (2006)
work page 2006
-
[17]
A review on brain MRI image segmentation techniques,
Salem, S. A. and Salem, N. M., “A review on brain MRI image segmentation techniques,” Int. J. Comput. Appl.84(9), 1–10 (2013)
work page 2013
-
[18]
A survey on deep learning for medical image segmentation,
Wu, J., et al., “A survey on deep learning for medical image segmentation,” Neurocomputing (2025)
work page 2025
-
[19]
Efficient multi-scale 3D CNN with fully connected CRF for accurate brain lesion segmenta- tion,
Kamnitsas, K., Ledig, C., Newcombe, V. F., Simpson, J. P., Kane, A. D., Menon, D. K., Rueckert, D., and Glocker, B., “Efficient multi-scale 3D CNN with fully connected CRF for accurate brain lesion segmenta- tion,” Med. Image Anal.36, 61–78 (2017)
work page 2017
-
[20]
Kirillov, A., Mintun, E., Ravi, N., Mao, H., Rolland, C., Gustafson, L., Xiao, T., Whitehead, S., Berg, A. C., Lo, W.-Y., Dollar, P., and Girshick, R., “Segment anything,” Proc. IEEE/CVF ICCV, 4015–4026 (2023)
work page 2023
-
[21]
Transfusion: Understanding transfer learning for medical imaging,
Raghu, M., Zhang, C., Kleinberg, J., and Bengio, S., “Transfusion: Understanding transfer learning for medical imaging,” Proc. NeurIPS, 3347–3357 (2019)
work page 2019
-
[22]
An image is worth 16x16 words: Transformers for image recognition at scale,
Dosovitskiy, A., Beyer, L., Kolesnikov, A., Weissenborn, D., Zhai, X., Unterthiner, T., Dehghani, M., Minderer, M., Heigold, G., Gelly, S., Uszkoreit, J., and Houlsby, N., “An image is worth 16x16 words: Transformers for image recognition at scale,” Proc. ICLR (2021)
work page 2021
-
[23]
Decoupled weight decay regularization,
Loshchilov, I. and Hutter, F., “Decoupled weight decay regularization,” Proc. ICLR (2019)
work page 2019
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.