Recognition: unknown
Combined photon-proton modeling of radiation-induced brain imaging changes supports variability in proton relative biological effectiveness and increased periventricular radiosensitivity
Pith reviewed 2026-05-10 16:15 UTC · model grok-4.3
The pith
Voxel modeling across photon and proton brain patients shows variable proton RBE and higher periventricular radiosensitivity.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
Spatially resolved predictive modeling of RICE in a combined photon-proton cohort identifies absorbed dose, LETd for protons, and periventricular region as predictors. The model implies a variable proton RBE described by RBE=1+m⋅LETd with m=0.10 μm/keV. At the patient level, the equivalent uniform dose (EUDa=8) in the brain based on this RBE achieved the highest predictive performance. The cross-modality framework enables clinical assessment of proton RBE without reliance on predefined reference dose-response relationships.
What carries the argument
Voxel-level logistic regression applied to combined photon-proton irradiation data, from which a clinical RBE model is derived by comparing estimated risk between the two modalities.
If this is right
- Proton RBE increases linearly with dose-averaged linear energy transfer in brain tissue.
- The periventricular region exhibits elevated radiosensitivity and should be considered a more sensitive organ at risk.
- Variable RBE improves prediction of radiation-induced contrast enhancements over constant RBE assumptions.
- Incorporating LET dependence and periventricular protection into planning may reduce side effects in proton therapy.
Where Pith is reading between the lines
- Treatment planning systems could prioritize low-LET proton paths near the ventricles to lower risk.
- The mixed-cohort regression method could be tested on other radiation toxicities where both modalities are used.
- This supports clinical trials that adapt proton plans based on LET maps rather than fixed RBE=1.1.
Load-bearing premise
Voxel-level logistic regression on observational data from mixed photon-proton patients can isolate causal effects of LET and periventricular location without residual confounding from patient selection, imaging timing, or unmeasured spatial correlations.
What would settle it
A matched comparison showing identical RICE rates for photons and protons at the same physical dose and location, or direct experimental measurements of proton RBE in brain tissue that show no linear dependence on LETd.
Figures


read the original abstract
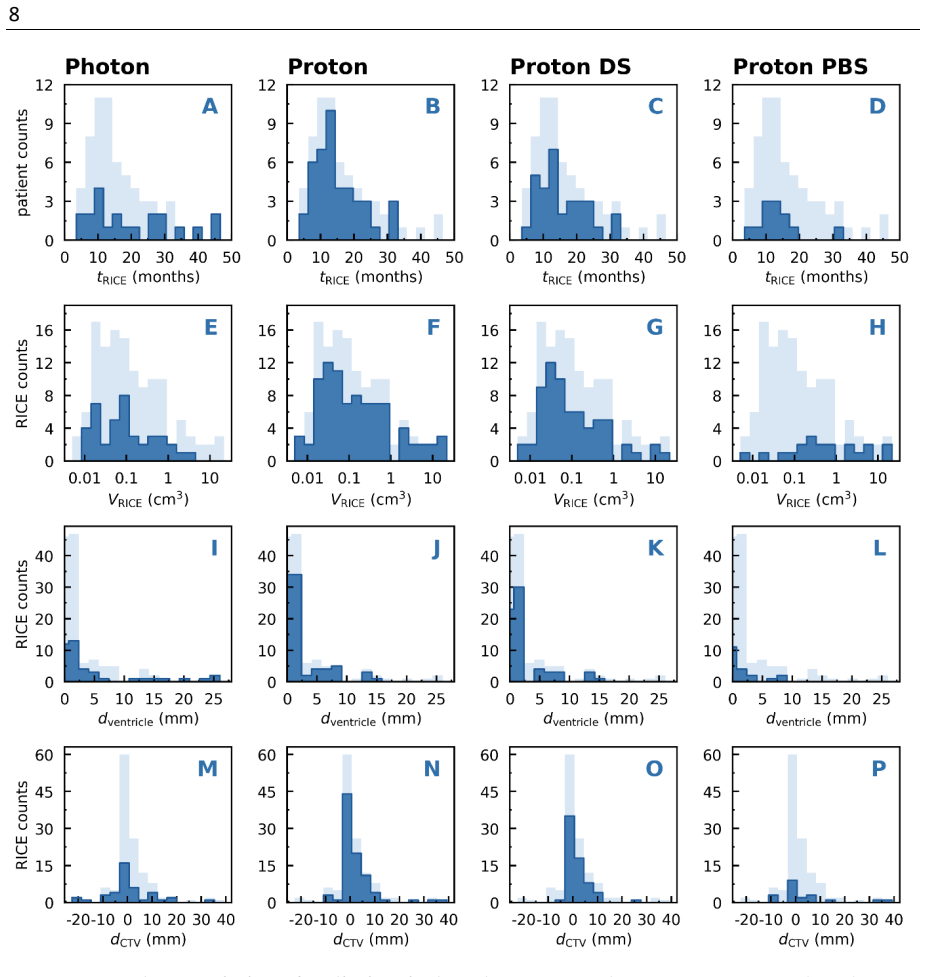
Purpose: Recent investigations of radiation-induced contrast enhancements (RICE) in brain tumor patients after proton therapy indicated variability in proton relative biological effectiveness (RBE) and increased radiosensitivity of the periventricular region (PVR). Prior studies, however, were restricted to proton cohorts requiring assumptions on reference radiation. This study assessed proton RBE variability and PVR radiosensitivity using spatially resolved predictive modeling of RICE in a combined photon-proton cohort. Methods and Materials: Predictive models for RICE detected on follow-up magnetic resonance imaging were developed in 152 brain tumor patients treated with photons or protons. Logistic regression was applied at the voxel level to model spatial occurrence and at the patient level to model incidence. A clinical RBE model was derived from voxel-wise comparisons of estimated risk between photon and proton irradiation. Results: In total, 128 RICE of various grades occurred in 64 patients. Voxel-level modeling identified absorbed dose (D), D multiplied by dose-averaged linear energy transfer (LETd) for proton therapy, and PVR as independent predictors of RICE. The model implied a variable proton RBE described by RBE=1+m$\cdot$LETd, with m=0.10 $\mu$m/keV. At the patient level, the equivalent uniform dose (EUDa=8) in the brain based on this RBE achieved the highest predictive performance. Conclusions: RICE was spatially associated with increased LET-dependent proton RBE and elevated PVR radiosensitivity across photon and proton radiotherapy. The cross-modality framework enables clinical assessment of proton RBE without reliance on predefined reference dose-response relationships. Incorporating variable proton RBE and the PVR as an organ at risk may improve risk assessment and mitigation of radiation-induced side effects.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript develops voxel-level logistic regression models for radiation-induced contrast enhancements (RICE) in a cohort of 152 brain tumor patients treated with photons or protons. It identifies absorbed dose D, the D × LETd interaction term for proton voxels, and periventricular region (PVR) status as independent predictors. From the fitted coefficients the authors derive a variable proton RBE model of the form RBE = 1 + m · LETd with m = 0.10 μm/keV, and report that an equivalent uniform dose (EUDa = 8) computed with this RBE yields the highest patient-level predictive performance for RICE incidence. The work concludes that the cross-modality framework supports LET-dependent RBE variability and elevated PVR radiosensitivity without requiring pre-defined photon reference curves.
Significance. If the central claims survive independent validation and confounding checks, the study supplies a data-driven route to estimate proton RBE variability directly from clinical imaging endpoints in mixed cohorts. This could refine treatment planning by incorporating LET effects and designating the periventricular region as a radiosensitive organ at risk. The approach avoids some assumptions of prior proton-only analyses, but its observational design and lack of reported external validation limit immediate clinical translation.
major comments (3)
- [Results] Results (voxel-level modeling and RBE derivation): The coefficient m = 0.10 μm/keV is obtained by fitting the logistic model to the same observational data later used to compute and rank patient-level EUDa performance. No cross-validation, hold-out test set, or bootstrap procedure is described for the interaction term or for the subsequent EUD comparison, so the reported superiority of EUDa = 8 is evaluated on the training data by construction.
- [Methods] Methods and Results (model assumptions): The logistic regression treats photon- and proton-treated voxels as exchangeable conditional on D and PVR status. In an observational cohort, modality assignment correlates with tumor location, histology, and follow-up MRI timing; these factors also affect periventricular exposure and RICE detection. Residual confounding or spatial autocorrelation among voxels can therefore bias the D × LETd coefficient and the inferred RBE variability.
- [Results] Results (patient-level analysis): The value a = 8 for the EUD is selected because it produces the highest predictive performance; the manuscript does not state whether this parameter was pre-specified or whether multiple a values were tested with appropriate multiplicity correction.
minor comments (2)
- [Methods] The translation from logistic coefficients to the explicit RBE formula RBE = 1 + m · LETd should be derived step-by-step in the Methods section with the relevant equations shown.
- [Methods] No details are provided on how spatial autocorrelation among voxels within patients was handled (e.g., mixed-effects models, cluster-robust standard errors, or permutation tests).
Simulated Author's Rebuttal
We thank the referee for the detailed and constructive review. The comments highlight important methodological considerations for our observational analysis. We address each major comment below and have revised the manuscript to strengthen the presentation of limitations and statistical procedures.
read point-by-point responses
-
Referee: [Results] Results (voxel-level modeling and RBE derivation): The coefficient m = 0.10 μm/keV is obtained by fitting the logistic model to the same observational data later used to compute and rank patient-level EUDa performance. No cross-validation, hold-out test set, or bootstrap procedure is described for the interaction term or for the subsequent EUD comparison, so the reported superiority of EUDa = 8 is evaluated on the training data by construction.
Authors: We agree that the RBE parameter and EUD ranking were derived from the full dataset without an independent validation set or cross-validation, which limits the strength of claims about superiority. This is an inherent feature of the exploratory analysis in this cohort. In the revision we will add bootstrap resampling (1000 iterations) to quantify uncertainty in the interaction coefficient and to evaluate the stability of the EUDa performance ordering. We will also explicitly state that the reported EUD comparison is internal to the training data and should be interpreted as hypothesis-generating pending external validation. revision: partial
-
Referee: [Methods] Methods and Results (model assumptions): The logistic regression treats photon- and proton-treated voxels as exchangeable conditional on D and PVR status. In an observational cohort, modality assignment correlates with tumor location, histology, and follow-up MRI timing; these factors also affect periventricular exposure and RICE detection. Residual confounding or spatial autocorrelation among voxels can therefore bias the D × LETd coefficient and the inferred RBE variability.
Authors: We acknowledge the risk of residual confounding and spatial dependence in this observational setting. Although the combined photon-proton design avoids the need for an external photon reference curve, unmeasured factors such as histology, tumor location, and imaging timing remain potential sources of bias. The revised manuscript includes an expanded limitations paragraph that discusses these issues and notes that the D × LETd interaction should be interpreted cautiously. We also added a sensitivity analysis that clusters standard errors at the patient level to partially account for within-patient voxel correlation. revision: yes
-
Referee: [Results] Results (patient-level analysis): The value a = 8 for the EUD is selected because it produces the highest predictive performance; the manuscript does not state whether this parameter was pre-specified or whether multiple a values were tested with appropriate multiplicity correction.
Authors: The exponent a was varied over a discrete grid (a = 1, 2, 4, 8, 16) to identify the value maximizing patient-level AUC. This selection was data-driven rather than pre-specified. In the revision we now report AUC values for the full grid, note that a = 8 was chosen post hoc, and apply a simple Bonferroni adjustment when highlighting the peak performance. We have also clarified the exploratory nature of the EUD parameter search in the methods and discussion. revision: yes
Circularity Check
No significant circularity; empirical model fit and interpretation are self-contained
full rationale
The paper fits a voxel-level logistic regression including absorbed dose D, a D × LETd interaction for protons, and a PVR indicator. It then interprets the ratio of the interaction coefficient to the D coefficient as the slope m in RBE = 1 + m · LETd. This is a direct reparameterization of the fitted model rather than a separate prediction. The subsequent patient-level EUD evaluation applies the same fitted coefficients to aggregate incidence prediction and compares performance across model variants. No step reduces by construction to its own inputs, no self-citation chain is load-bearing, and no uniqueness theorem or ansatz is smuggled in. The analysis remains an in-sample empirical estimation on observational data; any concerns about confounding or generalizability fall under validity rather than circularity.
Axiom & Free-Parameter Ledger
free parameters (2)
- m =
0.10 μm/keV
- EUDa =
8
axioms (2)
- domain assumption Voxel-level observations are independent after accounting for dose, LETd, and PVR status in the logistic model.
- domain assumption Photon and proton cohorts are comparable after adjustment for absorbed dose and other covariates.
Reference graph
Works this paper leans on
-
[1]
Relative biological effectiveness (RBE) values for proton beam therapy
Paganetti H, Niemierko A, Ancukiewicz M, Gerweck LE, Goitein M, Loeffler JS, et al. Relative biological effectiveness (RBE) values for proton beam therapy. Int J Radiat Oncol Biol Phys 2002;53:407–21. https://doi.org/10.1016/S0360-3016(02)02754-2
-
[2]
Relative Biological Effectiveness—Clinical Practice at US Proton Therapy Centers
Lühr A, Mohan R, Mahajan A, Shih HA, Paganetti H. Relative Biological Effectiveness—Clinical Practice at US Proton Therapy Centers. Int J Part Ther 2025;18:101212. https://doi.org/10.1016/j.ijpt.2025.101212
-
[3]
Heuchel L, Hahn C, Pawelke J, Sørensen BS, Dosanjh M, Lühr A. Clinical use and future requirements of relative biological effectiveness: Survey among all European proton therapy centres. Radiotherapy and Oncology 2022;172:134–9. https://doi.org/10.1016/j.radonc.2022.05.015
-
[4]
Journal of the ICRU 2007
Seltzer SM, Dawson P, Doi K, Gahbauer RA, Inokuti M, Jones DTL, et al. Journal of the ICRU 2007
2007
-
[5]
Relative biological effectiveness (RBE) values for proton beam therapy
Paganetti H. Relative biological effectiveness (RBE) values for proton beam therapy. Variations as a function of biological endpoint, dose, and linear energy transfer. Phys Med Biol 2014;59:R419–72. https://doi.org/10.1088/0031-9155/59/22/R419
-
[6]
Relative biological effectiveness in proton beam therapy – Current knowledge and future challenges
Lühr A, von Neubeck C, Krause M, Troost EGC. Relative biological effectiveness in proton beam therapy – Current knowledge and future challenges. Clin Transl Radiat Oncol 2018;9:35–41. https://doi.org/10.1016/j.ctro.2018.01.006
-
[7]
Paganetti H, Goitein M. Radiobiological significance of beamline dependent proton energy distributions in a spread-out Bragg peak. Med Phys 2000;27:1119–26. https://doi.org/10.1118/1.598977
-
[8]
Range uncertainty in proton therapy due to variable biological effectiveness
Carabe A, Moteabbed M, Depauw N, Schuemann J, Paganetti H. Range uncertainty in proton therapy due to variable biological effectiveness. Phys Med Biol 2012;57:1159–
2012
-
[9]
https://doi.org/10.1088/0031-9155/57/5/1159
-
[10]
Physical and biological factors determining the effective proton range
Grün R, Friedrich T, Krämer M, Zink K, Durante M, Engenhart-Cabillic R, et al. Physical and biological factors determining the effective proton range. Med Phys 2013;40. https://doi.org/10.1118/1.4824321
-
[11]
Lühr A, Wagenaar D, Eekers DBP, Glimelius L, Habraken SJM, Harrabi S, et al. Recommendations for reporting and evaluating proton therapy beyond dose and Photon-proton modeling of brain imaging changes 17 Last edited on April 11, 2026 constant relative biological effectiveness. Phys Imaging Radiat Oncol 2025;33. https://doi.org/10.1016/j.phro.2024.100692
-
[12]
Palkowitsch M, Kaufmann LM, Hennings F, Menkel S, Hahn C, Bensberg J, et al. Variable-RBE-induced NTCP predictions for various side-effects following proton therapy for brain tumors – Identification of high-risk patients and risk mitigation. Radiotherapy and Oncology 2025;202. https://doi.org/10.1016/j.radonc.2024.110590
-
[13]
Hahn C, Heuchel L, Ödén J, Traneus E, Wulff J, Plaude S, et al. Comparing biological effectiveness guided plan optimization strategies for cranial proton therapy: potential and challenges. Radiation Oncology 2022;17. https://doi.org/10.1186/s13014-022-02143- x
-
[14]
McIntyre M, Wilson P, Gorayski P, Bezak E. A Systematic Review of LET-Guided Treatment Plan Optimisation in Proton Therapy: Identifying the Current State and Future Needs. Cancers (Basel) 2023;15. https://doi.org/10.3390/cancers15174268
-
[15]
Giantsoudi D, Grassberger C, Craft D, Niemierko A, Trofimov A, Paganetti H. Linear energy transfer-guided optimization in intensity modulated proton therapy: Feasibility study and clinical potential. Int J Radiat Oncol Biol Phys 2013;87:216–22. https://doi.org/10.1016/j.ijrobp.2013.05.013
-
[16]
Traneus E, Ödén J. Introducing Proton Track-End Objectives in Intensity Modulated Proton Therapy Optimization to Reduce Linear Energy Transfer and Relative Biological Effectiveness in Critical Structures. Int J Radiat Oncol Biol Phys 2019;103:747–57. https://doi.org/10.1016/j.ijrobp.2018.10.031
-
[17]
Reoptimization of Intensity Modulated Proton Therapy Plans Based on Linear Energy Transfer
Unkelbach J, Botas P, Giantsoudi D, Gorissen BL, Paganetti H. Reoptimization of Intensity Modulated Proton Therapy Plans Based on Linear Energy Transfer. Int J Radiat Oncol Biol Phys 2016;96:1097–106. https://doi.org/10.1016/j.ijrobp.2016.08.038
-
[18]
Grassberger C, Trofimov A, Lomax A, Paganetti H. Variations in linear energy transfer within clinical proton therapy fields and the potential for biological treatment planning. Int J Radiat Oncol Biol Phys 2011;80:1559–66. https://doi.org/10.1016/j.ijrobp.2010.10.027
-
[19]
Optimization of radiobiological effects in intensity modulated proton therapy
Wilkens JJ, Oelfke U. Optimization of radiobiological effects in intensity modulated proton therapy. Med Phys 2005;32:455–65. https://doi.org/10.1118/1.1851925
-
[20]
Heuchel L, Hahn C, Ödén J, Traneus E, Wulff J, Timmermann B, et al. The dirty and clean dose concept: Towards creating proton therapy treatment plans with a photon- like dose response. Med Phys 2024;51:622–36. https://doi.org/10.1002/mp.16809
-
[21]
NRG Oncology White Paper on the Relative Biological Effectiveness in Proton Therapy
Paganetti H, Simone CB, Bosch WR, Haas-Kogan D, Kirsch DG, Li H, et al. NRG Oncology White Paper on the Relative Biological Effectiveness in Proton Therapy. Int J Radiat Oncol Biol Phys 2025;121:202–17. https://doi.org/10.1016/j.ijrobp.2024.07.2152
-
[22]
A systematic review of clinical studies on variable proton Relative Biological Effectiveness (RBE)
Underwood TSA, McNamara AL, Appelt A, Haviland JS, Sørensen BS, Troost EGC. A systematic review of clinical studies on variable proton Relative Biological Effectiveness (RBE). Radiotherapy and Oncology 2022;175:79–92. https://doi.org/10.1016/j.radonc.2022.08.014. 18 Last edited on April 11, 2026
-
[23]
Mechanisms and Review of Clinical Evidence of Variations in Relative Biological Effectiveness in Proton Therapy
Paganetti H. Mechanisms and Review of Clinical Evidence of Variations in Relative Biological Effectiveness in Proton Therapy. Int J Radiat Oncol Biol Phys 2022;112:222–
2022
-
[24]
https://doi.org/10.1016/j.ijrobp.2021.08.015
-
[25]
Wagenaar D, Schuit E, van der Schaaf A, Langendijk JA, Both S. Can the mean linear energy transfer of organs be directly related to patient toxicities for current head and neck cancer intensity-modulated proton therapy practice? Radiotherapy and Oncology 2021;165:159–65. https://doi.org/10.1016/j.radonc.2021.09.003
-
[26]
Lauwens L, Ribeiro MF, Zegers CML, Høyer M, Alapetite C, Blomstrand M, et al. Systematic review of MRI alterations in the brain following proton and photon radiation therapy: Towards a uniform European Particle Therapy Network (EPTN) definition. Radiotherapy and Oncology 2025;208. https://doi.org/10.1016/j.radonc.2025.110936
-
[27]
Radiation necrosis in pediatric patients with brain tumors treated with proton radiotherapy
Kralik SF, Ho CY, Finke W, Buchsbaum JC, Haskins CP, Shih CS. Radiation necrosis in pediatric patients with brain tumors treated with proton radiotherapy. American Journal of Neuroradiology 2015;36:1572–8. https://doi.org/10.3174/ajnr.A4333
-
[28]
Walker AJ, Ruzevick J, Malayeri AA, Rigamonti D, Lim M, Redmond KJ, et al. Postradiation imaging changes in the CNS: How can we differentiate between treatment effect and disease progression? Future Oncology 2014;10:1277–97. https://doi.org/10.2217/fon.13.271
-
[29]
Peeler, CR; Mirkovic, D; Titt, U; Blanchard, P; Gunther, JR; Mahajan, A; Mohan, R; and Grosshans D. Clinical evidence of variable proton biological effectiveness in pediatric patients treated for ependymoma. Physiol Behav 2017;176:139–48. https://doi.org/10.1016/j.radonc.2016.11.001
-
[30]
Niemierko A, Schuemann J, Niyazi M, Giantsoudi D, Maquilan G, Shih HA, et al. Brain Necrosis in Adult Patients After Proton Therapy: Is There Evidence for Dependency on Linear Energy Transfer? Int J Radiat Oncol Biol Phys 2021;109:109–19. https://doi.org/10.1016/j.ijrobp.2020.08.058
-
[31]
Roberts KW, Wan Chan Tseung HS, Eckel LJ, Harmsen WS, Beltran C, Laack NN. Biologic Dose and Imaging Changes in Pediatric Brain Tumor Patients Receiving Spot Scanning Proton Therapy. Int J Radiat Oncol Biol Phys 2019;105:664–73. https://doi.org/10.1016/j.ijrobp.2019.06.2534
-
[32]
Radiation induced contrast enhancement after proton beam therapy in patients with low grade glioma – How safe are protons? Radiotherapy and Oncology 2022;167:211–
Harrabi SB, von Nettelbladt B, Gudden C, Adeberg S, Seidensaal K, Bauer J, et al. Radiation induced contrast enhancement after proton beam therapy in patients with low grade glioma – How safe are protons? Radiotherapy and Oncology 2022;167:211–
2022
-
[33]
https://doi.org/10.1016/j.radonc.2021.12.035
-
[34]
Giantsoudi D, Sethi R V., Yeap BY, Eaton BR, Ebb DH, Caruso PA, et al. Incidence of CNS Injury for a Cohort of 111 Patients Treated with Proton Therapy for Medulloblastoma: LET and RBE Associations for Areas of Injury. Int J Radiat Oncol Biol Phys 2016;95:287–96. https://doi.org/10.1016/j.ijrobp.2015.09.015. Photon-proton modeling of brain imaging changes...
-
[35]
Risk modeling of imaging changes after proton beam therapy for childhood brain tumors
Heinzelmann F, Peters S, Quenzer A, Lühr A, Löck S, Schleithoff SS, et al. Risk modeling of imaging changes after proton beam therapy for childhood brain tumors. Radiotherapy and Oncology 2025:111261. https://doi.org/10.1016/j.radonc.2025.111261
-
[36]
Bregman A, Rutgers JJ, Andersen T, van der Schaaf A, Brouwer CL, Janssens GO, et al. Development of the first prediction model for radiation-induced contrast enhancement after proton therapy for posterior fossa tumours in paediatric patients. Radiotherapy and Oncology 2026;216:111360. https://doi.org/10.1016/j.radonc.2025.111360
-
[37]
Vestergaard A, Kallehauge JF, Muhic A, Carlsen JF, Dahlrot RH, Lukacova S, et al. Mixed effect model confirms increased risk of image changes with increasing linear energy transfer in proton therapy of gliomas. Radiotherapy and Oncology 2025;204. https://doi.org/10.1016/j.radonc.2025.110716
-
[38]
Lütgendorf-Caucig C, Pelak M, Hug E, Flechl B, Surböck B, Marosi C, et al. Prospective Analysis of Radiation-Induced Contrast Enhancement and Health-Related Quality of Life After Proton Therapy for Central Nervous System and Skull Base Tumors. Int J Radiat Oncol Biol Phys 2024;118:1206–16. https://doi.org/10.1016/j.ijrobp.2024.01.007
-
[39]
Bahn E, Bauer J, Harrabi S, Herfarth K, Debus J, Alber M. Late Contrast Enhancing Brain Lesions in Proton-Treated Patients With Low-Grade Glioma: Clinical Evidence for Increased Periventricular Sensitivity and Variable RBE. International Journal of Radiation Oncology*Biology*Physics 2020;107:571–8. https://doi.org/10.1016/j.ijrobp.2020.03.013
-
[40]
Eulitz J, G. C. Troost E, Klünder L, Raschke F, Hahn C, Schulz E, et al. Increased relative biological effectiveness and periventricular radiosensitivity in proton therapy of glioma patients. Radiotherapy and Oncology 2023;178:109422. https://doi.org/10.1016/j.radonc.2022.11.011
-
[41]
Engeseth GM, He R, Mirkovic D, Yepes P, Mohamed ASR, Stieb S, et al. Mixed Effect Modeling of Dose and Linear Energy Transfer Correlations With Brain Image Changes After Intensity Modulated Proton Therapy for Skull Base Head and Neck Cancer. Int J Radiat Oncol Biol Phys 2021;111:684–92. https://doi.org/10.1016/j.ijrobp.2021.06.016
-
[42]
Bertolet A, Abolfath R, Carlson DJ, Lustig RA, Hill-Kayser C, Alonso-Basanta M, et al. Correlation of LET With MRI Changes in Brain and Potential Implications for Normal Tissue Complication Probability for Patients With Meningioma Treated With Pencil Beam Scanning Proton Therapy. Int J Radiat Oncol Biol Phys 2022;112:237–46. https://doi.org/10.1016/j.ijro...
-
[43]
Grey A, Justus T, Wahl H, Engellandt K, Seidlitz A, Bütof R, et al. Incidence and time course of new contrast-enhancing lesions on MRI after proton versus photon radiotherapy in glioma patients. Neuroradiology 2025. https://doi.org/10.1007/s00234- 025-03829-1
-
[44]
Palkowitsch M, Kilian LS, Hennings F, Lühr A, Thiem J, Grey A, et al. Model validation confirms variable relative biological effectiveness and elevated 20 Last edited on April 11, 2026 periventricular sensitivity after proton therapy of brain tumors. Radiotherapy and Oncology 2026;214. https://doi.org/10.1016/j.radonc.2025.111271
-
[45]
Eulitz J, Lutz B, Wohlfahrt P, Dutz A, Enghardt W, Karpowitz C, et al. A Monte Carlo based radiation response modelling framework to assess variability of clinical RBE in proton therapy. Phys Med Biol 2019;64. https://doi.org/10.1088/1361-6560/ab3841
-
[46]
Lutz B, Eulitz J, Haneke-Swanson R, Enghardt W, Lühr A. Precision modeling of the IBA Universal Nozzle double scattering mode at the University Proton Therapy Dresden for Monte Carlo simulation. Journal of Instrumentation 2021;16. https://doi.org/10.1088/1748-0221/16/03/T03007
-
[47]
TOPAS: An innovative proton Monte Carlo platform for research and clinical applications
Perl J, Shin J, Schümann J, Faddegon B, Paganetti H. TOPAS: An innovative proton Monte Carlo platform for research and clinical applications. Med Phys 2012;39:6818–
2012
-
[48]
https://doi.org/10.1118/1.4758060
-
[49]
Hahn C, Ödén J, Dasu A, Vestergaard A, Fuglsang Jensen M, Sokol O, et al. Towards harmonizing clinical linear energy transfer (LET) reporting in proton radiotherapy: a European multi-centric study. Acta Oncol (Madr) 2022;61:206–14. https://doi.org/10.1080/0284186X.2021.1992007
-
[50]
Wang CC, McNamara AL, Shin J, Schuemann J, Grassberger C, Taghian AG, et al. End-of-Range Radiobiological Effect on Rib Fractures in Patients Receiving Proton Therapy for Breast Cancer. Int J Radiat Oncol Biol Phys 2020;107:449–54. https://doi.org/10.1016/j.ijrobp.2020.03.012
-
[51]
Glowa C, Saager M, Hintz L, Euler-Lange R, Peschke P, Brons S, et al. Variable Relative Biological Effectiveness of Protons in the Rat Spinal Cord: Measurements and Comparison With Model Calculations. Adv Radiat Oncol 2025;10. https://doi.org/10.1016/j.adro.2025.101809
-
[52]
Hahn C, Eulitz J, Peters N, Wohlfahrt P, Enghardt W, Richter C, et al. Impact of range uncertainty on clinical distributions of linear energy transfer and biological effectiveness in proton therapy. Med Phys 2020;47:6151–62. https://doi.org/10.1002/mp.14560
-
[53]
Sørensen BS, Pawelke J, Bauer J, Burnet NG, Dasu A, Høyer M, et al. Does the uncertainty in relative biological effectiveness affect patient treatment in proton therapy? Radiotherapy and Oncology 2021;163:177–84. https://doi.org/10.1016/j.radonc.2021.08.016
-
[54]
Sallem H, Harrabi S, Traneus E, Herfarth K, Debus J, Bauer J. A model-based risk- minimizing proton treatment planning concept for brain injury prevention in low- grade glioma patients. Radiotherapy and Oncology 2024;201. https://doi.org/10.1016/j.radonc.2024.110579
-
[55]
Ortkamp T, Sallem H, Harrabi S, Frank M, Jäkel O, Bauer J, et al. Direct optimization of the probability of lesion origin in proton treatment planning for low-grade glioma patients. Med Phys 2026;53. https://doi.org/10.1002/mp.70395. Last edited on April 11, 2026 Supplement Combined photon–proton modeling of radiation-induced brain imaging changes support...
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.