Quantitative Evaluation of the Severity of Posttraumatic Stress Disorder through Transfer Learning from Specific Phobia Data
Pith reviewed 2026-06-29 22:25 UTC · model grok-4.3
The pith
Machine learning transfers arachnophobia fear responses to classify PTSD severity at 86 percent accuracy
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
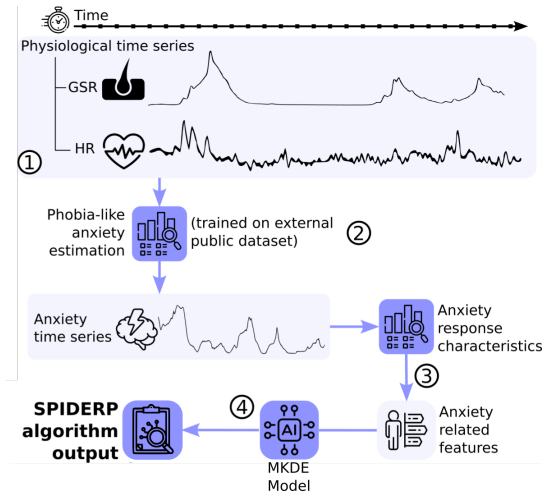
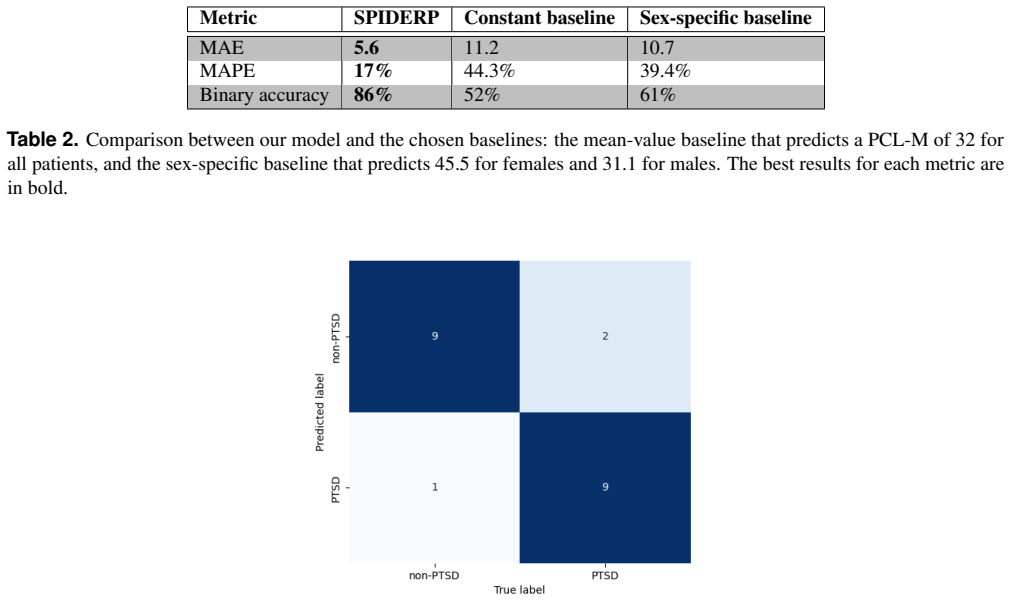
Training a fear-response model on arachnophobia data allows extraction of PTSD predictive features from fear-response curves in military simulation data, yielding 86 percent accuracy for PTSD classification and a mean absolute error of 5.6 for severity estimation on the PCL-M scale.
What carries the argument
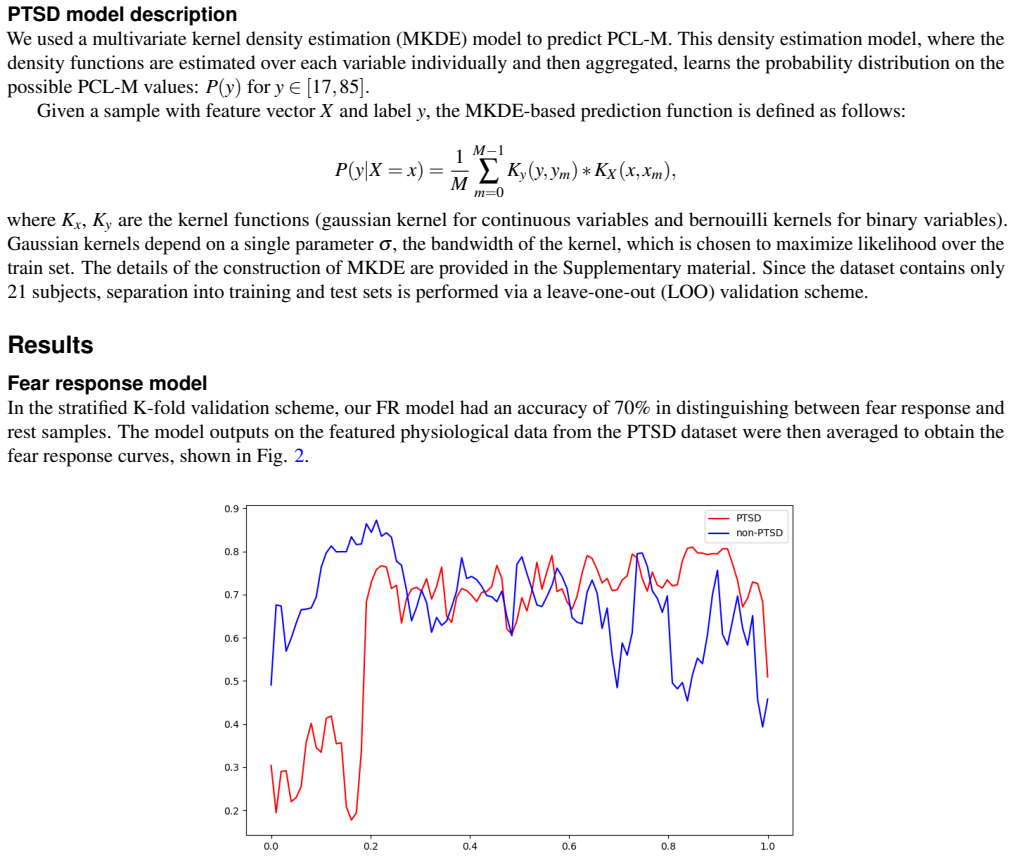
multivariate kernel density estimation (MKDE) fear-response model
Load-bearing premise
Fear responses measured in arachnophobia are structured similarly to those triggered by PTSD-related stimuli in the military simulation.
What would settle it
If applying the model to the military dataset resulted in classification accuracy close to 50 percent, this would show that the transfer did not capture relevant predictive features.
Figures
read the original abstract
Posttraumatic stress disorder (PTSD) is a prevalent and debilitating mental health condition with significant personal and societal impacts. Current clinical assessments of PTSD often rely on subjective evaluations, which can be time-consuming, costly, and prone to human bias. This study proposes a machine learning (ML) approach based on multivariate kernel density estimation (MKDE) technique for the objective evaluation of PTSD severity. We collected heart rate (HR) and galvanic skin response (GSR) signals as well as PTSD Checklist - Military Version (PCL-M) labels from 21 participants during an immersive simulation. A fear-response model was trained on a public arachnophobia dataset, and predictive features of PTSD were extracted from the fear-response curves estimated on the military dataset. The model achieved an accuracy of 86\% in classifying PTSD status, effectively distinguishing participants with and without PTSD (PCL-M threshold of 36). The average mean absolute error (MAE) of the models is 5.6, and it estimated a clinical PTSD severity scale with a mean absolute percentage error of 17\%. Our algorithm demonstrates promising potential for enhancing estimation of PTSD severity and followup by offering an objective and low-effort evaluation approach using physiology. These findings suggest clinical utility in both screening and follow-up settings.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper claims that a multivariate kernel density estimation (MKDE) fear-response model trained on a public arachnophobia dataset can be transferred to extract predictive features from heart rate (HR) and galvanic skin response (GSR) signals collected during an immersive military simulation with 21 participants. Using these features, the approach classifies PTSD status (PCL-M threshold of 36) at 86% accuracy, estimates severity with mean absolute error (MAE) of 5.6, and achieves mean absolute percentage error (MAPE) of 17%, offering an objective physiological alternative to subjective clinical assessments.
Significance. If the transfer learning result holds after proper validation, the work would demonstrate a low-effort, physiology-based method for PTSD screening and follow-up that leverages an independent public dataset, which is a strength for reproducibility. The reported performance numbers on a small clinical sample would suggest clinical utility if shown to be robust, but the current evidence does not yet establish this.
major comments (3)
- [Abstract] Abstract and methods description: the headline results (86% accuracy, MAE 5.6, MAPE 17% on n=21) are presented without any description of cross-validation procedure, statistical testing, or handling of the small sample size, so it is impossible to determine whether the numbers reflect genuine predictive power or overfitting.
- [Abstract] Abstract: the central transfer-learning claim requires that MKDE fear-response curves fitted to arachnophobia HR/GSR traces remain predictive when applied to military-simulation data, yet no comparison of response-shape statistics, timing, or amplitude distributions across the two domains is supplied; without this, the 86% accuracy cannot be attributed to transferable fear encoding rather than dataset-specific artifacts.
- [Methods description] Methods description: feature extraction from the MKDE model and final evaluation both occur on the identical 21-participant PTSD dataset with no reported train/test separation or independent hold-out, creating a data-dependent fitting risk that directly undermines the reported classification and regression performance.
Simulated Author's Rebuttal
We thank the referee for the constructive comments, which highlight important gaps in the reporting of validation and transfer-learning evidence. We will revise the manuscript to address each point.
read point-by-point responses
-
Referee: [Abstract] Abstract and methods description: the headline results (86% accuracy, MAE 5.6, MAPE 17% on n=21) are presented without any description of cross-validation procedure, statistical testing, or handling of the small sample size, so it is impossible to determine whether the numbers reflect genuine predictive power or overfitting.
Authors: We agree that the abstract and methods lack these details. In the revised manuscript we will expand both sections to describe the cross-validation procedure employed, any statistical tests performed on the performance metrics, and an explicit discussion of limitations arising from the n=21 cohort size. revision: yes
-
Referee: [Abstract] Abstract: the central transfer-learning claim requires that MKDE fear-response curves fitted to arachnophobia HR/GSR traces remain predictive when applied to military-simulation data, yet no comparison of response-shape statistics, timing, or amplitude distributions across the two domains is supplied; without this, the 86% accuracy cannot be attributed to transferable fear encoding rather than dataset-specific artifacts.
Authors: The referee is correct that no such domain-comparison statistics are currently provided. We will add quantitative comparisons (e.g., Kolmogorov-Smirnov tests or summary statistics on peak amplitude, latency, and curve shape) between the arachnophobia and military-simulation fear-response curves to support the transferability claim. revision: yes
-
Referee: [Methods description] Methods description: feature extraction from the MKDE model and final evaluation both occur on the identical 21-participant PTSD dataset with no reported train/test separation or independent hold-out, creating a data-dependent fitting risk that directly undermines the reported classification and regression performance.
Authors: We acknowledge the risk of data-dependent fitting. The MKDE model was trained only on the arachnophobia data, yet the downstream classifiers/regressors were evaluated on features from all 21 participants without an independent hold-out. In the revision we will implement and report a proper cross-validation scheme (e.g., leave-one-subject-out) with clear separation between feature extraction and model evaluation. revision: yes
Circularity Check
No significant circularity detected
full rationale
The derivation trains an MKDE fear-response model exclusively on an independent public arachnophobia dataset, then applies the fixed model to estimate curves and extract features from the separate 21-participant military dataset. No equation or step defines a target quantity in terms of itself, renames a fitted parameter as a prediction, or relies on a self-citation chain for a uniqueness claim. The reported classification accuracy and error metrics are downstream applications of the transferred model rather than reductions to the input data by construction. The central claim therefore remains self-contained with external training data providing independent support.
Axiom & Free-Parameter Ledger
free parameters (1)
- PCL-M threshold =
36
axioms (2)
- domain assumption Fear-response curves derived from arachnophobia data share transferable structure with PTSD physiological responses
- domain assumption HR and GSR signals during simulation are sufficient to capture PTSD severity variation
Reference graph
Works this paper leans on
-
[1]
Diagnostic and statistical manual of mental disorders: DSM-5
American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-5. 5th ed. Washington, DC: American Psychiatric Publishing, a division of American Psychiatric Association; 2013
2013
-
[2]
Posttraumatic stress disorder in the World Mental Health Surveys
Koenen KC, Ratanatharathorn A, Ng L, McLaughlin KA, Bromet EJ, Stein DJ, et al. Posttraumatic stress disorder in the World Mental Health Surveys. Psychological Medicine. 2017;47(13):2260–2274. doi:10.1017/S0033291717000708
-
[3]
Benjet C, Bromet E, Karam EG, Kessler RC, McLaughlin KA, Ruscio AM, et al. The epidemiology of traumatic event expo- sure worldwide: results from the World Mental Health Survey Consortium. Psychological Medicine. 2016;46(2):327–343. doi:10.1017/S0033291715001981
-
[4]
Charlson F, Ommeren M, Flaxman A, Cornett J, Whiteford H, Saxena S. New WHO prevalence estimates of mental disorders in conflict settings: a systematic review and meta-analysis. The Lancet. 2019;394. doi:10.1016/S0140- 6736(19)30934-1. 8/14
-
[5]
Lifetime Events and Posttraumatic Stress Disorder in 4 Postconflict Settings
de Jong JTVM, Komproe IH, Van Ommeren M, El Masri M, Araya M, Khaled N, et al. Lifetime Events and Posttraumatic Stress Disorder in 4 Postconflict Settings. JAMA. 2001;286(5):555–562. doi:10.1001/jama.286.5.555
-
[6]
Rzeszutek M, Dragan M, Lis-Turlejska M, Schier K, Holas P, Drabarek K, et al. Exposure to self-reported traumatic events and probable PTSD in a national sample of Poles: Why does Poland’s PTSD prevalence differ from other national estimates? PLOS ONE. 2023;18. doi:10.1371/journal.pone.0287854
-
[7]
How Common Is PTSD in Adults? https://www
National Center for PTSD, US Department of Veterans Affairs. How Common Is PTSD in Adults? https://www. ptsd.va.gov/understand/common/common_adults.asp
-
[8]
Roberts N, Kitchiner N, Lewis C, Downes A, Bisson J. Psychometric properties of the PTSD Checklist for DSM-5 in a sam- ple of trauma exposed mental health service users. Eur J Psychotraumatol. 2022;12. doi:10.1080/20008198.2020.1863578
-
[9]
Bovin M, Marx B, Weathers F, Gallagher M, Rodriguez P, Schnurr P, et al. Psychometric Properties of the PTSD Checklist for Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition (PCL-5) in Veterans. Psychological assessment. 2015;28. doi:10.1037/pas0000254
-
[10]
Resick, al PA. A comparison of the CAPS-5 and PCL-5 to assess PTSD in military and veteran treatment-seeking samples. European journal of psychotraumatology. 2023;14. doi:10.1080/20008066.2023.2222608
-
[11]
Prevalence of post-traumatic stress disorder in the United States: a systematic literature review
Schein J, Houle C, Urganus A, Cloutier M, Patterson-Lomba O, Wang Y , et al. Prevalence of post-traumatic stress disorder in the United States: a systematic literature review. Current Medical Research and Opinion. 2021;37:1–1. doi:10.1080/03007995.2021.1978417
-
[12]
Prevalence, Detection and Correlates of PTSD in the Primary Care Setting: A Systematic Review
Greene T, Neria Y , Gross R. Prevalence, Detection and Correlates of PTSD in the Primary Care Setting: A Systematic Review. Journal of clinical psychology in medical settings. 2016;23. doi:10.1007/s10880-016-9449-8
-
[13]
Systematic review of machine learning in PTSD studies for automated diagnosis evaluation
Wu Y , Mao K, Dennett L, Chen J. Systematic review of machine learning in PTSD studies for automated diagnosis evaluation. npj Mental Health Research. 2023;2. doi:10.1038/s44184-023-00035-w
-
[14]
Psychophysiology of the posttraumatic stress disorder: from sulfur fumes to behavioral genetics
Shalev AY , Rogel-Fuchs Y . Psychophysiology of the posttraumatic stress disorder: from sulfur fumes to behavioral genetics. Psychosomatic medicine. 1993;55:413–423. doi:10.1097/00006842-199309000-00003
-
[15]
Neurobiological aspects of PTSD: Review of clinical and preclinical studies
Krystal JH, Kosten TR, Southwick S, Mason JW, Perry BD, Giller EL. Neurobiological aspects of PTSD: Review of clinical and preclinical studies. Behavior Therapy. 1989;20(2):177–198. doi:https://doi.org/10.1016/S0005-7894(89)80068-1
-
[16]
Posttraumatic Stress Disorder and Motor Vehicle Accidents: A Multidisciplinary Overview
Kuch K, Cox B, Evans R. Posttraumatic Stress Disorder and Motor Vehicle Accidents: A Multidisciplinary Overview. Canadian journal of psychiatry Revue canadienne de psychiatrie. 1996;41:429–34. doi:10.1177/070674379604100707
-
[17]
Pole N, Neylan T, Otte C, Metzler T, Best S, Henn-Haase C, et al. Associations Between Childhood Trauma and Emotion- Modulated Psychophysiological Responses to Startling Sounds: A Study of Police Cadets. Journal of abnormal psychology. 2007;116:352–61. doi:10.1037/0021-843X.116.2.352
-
[18]
De Novo Conditioning in Trauma-Exposed Individuals With and Without Posttraumatic Stress Disorder
Orr S, Metzger L, Lasko N, Macklin M, Peri T, Roger P. De Novo Conditioning in Trauma-Exposed Individuals With and Without Posttraumatic Stress Disorder. Journal of abnormal psychology. 2000;109:290–8. doi:10.1037/0021- 843X.109.2.290
-
[19]
Pellegrin G, Ricka N, Fompeyrine DA, Rohaly T, Enders L, Roy H. Assessment of PTSD in military personnel via machine learning based on physiological habituation in a virtual immersive environment. Scientific Reports. 2025;15:7562. doi:10.1038/s41598-025-91916-x
-
[20]
In: Posttraumatic stress disorder: from neurobiology to clinical presentation: Bremner/Posttraumatic Stress Disorder
Shalev A, Bremner J. In: Posttraumatic stress disorder: from neurobiology to clinical presentation: Bremner/Posttraumatic Stress Disorder. John Wiley & Sons; 2016. p. 1–26
2016
-
[21]
Assessing the current utilization status of wearable devices in clinical research
Miyakoshi T, Ito Y . Assessing the current utilization status of wearable devices in clinical research. Clinical trials (London, England). 2024; p. 17407745241230287. doi:10.1177/17407745241230287
-
[22]
Henriksen A, Mikalsen M, Woldaregay A, Muzny M, Hartvigsen G, Hopstock L, et al. Using Fitness Trackers and Smartwatches to Measure Physical Activity in Research: Analysis of Consumer Wrist-Worn Wearables. Journal of Medical Internet Research. 2018;20:e110. doi:10.2196/jmir.9157
-
[23]
Etkin A, Wager T. Functional Neuroimaging of Anxiety: A Meta-Analysis of Emotional Processing in PTSD, Social Anxiety Disorder, and Specific Phobia. The American journal of psychiatry. 2007;164:1476–88. doi:10.1176/appi.ajp.2007.07030504
-
[24]
Kleim B, Ehlers A. Reduced Autobiographical Memory Specificity Predicts Depression and Posttraumatic Stress Disorder After Recent Trauma. Journal of consulting and clinical psychology. 2008;76:231–42. doi:10.1037/0022-006X.76.2.231
-
[25]
Pfaltz M, Michael T, Meyer A, Wilhelm F. Reexperiencing Symptoms, Dissociation, and Avoidance Behaviors in Daily Life of Patients With PTSD and Patients With Panic Disorder With Agoraphobia. Journal of traumatic stress. 2013;26. doi:10.1002/jts.21822
-
[26]
Emerging Wearable Medical Devices towards Personalized Healthcare
Zheng J, Shen Y , Zhang Z, Wu T, Zhang G, Lu H. Emerging Wearable Medical Devices towards Personalized Healthcare. In: Conference on Body Area Networks; 2013. p. 427–431
2013
-
[27]
Wang J, Ouyang H, Jiao R, Cheng S, Zhang H, Shang Z, et al. The application of machine learning techniques in posttraumatic stress disorder: a systematic review and meta-analysis. npj Digital Medicine. 2024;7. doi:10.1038/s41746- 9/14 024-01117-5
-
[28]
Tahmasian M, Jamalabadi H, Abedini M, Ghadami M, Sepehry A, Knight D, et al. Differentiation chronic post traumatic stress disorder patients from healthy subjects using objective and subjective sleep-related parameters. Neuroscience Letters. 2017;650. doi:10.1016/j.neulet.2017.04.042
-
[30]
Post-Traumatic Stress Disorder: The Relationship Between the Fear Response and Chronic Stress
Maeng L, Milad M. Post-Traumatic Stress Disorder: The Relationship Between the Fear Response and Chronic Stress. Chronic Stress. 2017;1:247054701771329. doi:10.1177/2470547017713297
-
[31]
Prefrontal cortex, amygdala, and threat processing: implications for PTSD
Kredlow M, Fenster R, Laurent E, Ressler K, Phelps E. Prefrontal cortex, amygdala, and threat processing: implications for PTSD. Neuropsychopharmacology. 2021;47:1–13. doi:10.1038/s41386-021-01155-7
-
[32]
Using the PTSD Checklist for DSM-IV (PCL) https://www.ptsd.va.gov/professional/assessment/documents/PCL_handoutDSM4.pdf (accessed May 2026)
National Center for PTSD. Using the PTSD Checklist for DSM-IV (PCL) https://www.ptsd.va.gov/professional/assessment/documents/PCL_handoutDSM4.pdf (accessed May 2026)
2026
-
[33]
Soldier Performance in Sociotechnical Environments (Summary Technical Report)
Roy H, Enders L, Cohen-Hoffing R, Touryan J, Rohaly T, Dalangin B, et al. Soldier Performance in Sociotechnical Environments (Summary Technical Report). ARL-TR-9997 APG, MD. 2024; p. 315–336
2024
-
[34]
The PTSD Checklist (PCL): Reliability, validity, and diagnostic utility
Weathers F, Litz B, Herman D, Huska JA, Keane T. The PTSD Checklist (PCL): Reliability, validity, and diagnostic utility. Paper Presented at the Annual Convention of the International Society for Traumatic Stress Studies. 1993
1993
-
[35]
Ihmig FR, Gogeascoechea A, Schäfer S, Lass-Hennemann J, Michael T. Electrocardiogram, skin conductance and respiration from spider-fearful individuals watching spider video clips (version 1.0.0). PhysioNet. 2020. doi: 10.13026/sq6q- zg04
-
[36]
Ihmig F, Gogeascoechea A, Neurohr-Parakenings F, Schäfer S, Lass-Hennemann J, Michael T. On-line anxiety level detection from biosignals: Machine learning based on a randomized controlled trial with spider-fearful individuals. PLOS ONE. 2020;15:e0231517. doi:10.1371/journal.pone.0231517
-
[37]
Respiratory Markers Significantly Enhance Anxiety Detection Using Multimodal Physiological Sensing
Gazi A, Lis P, Mohseni A, Ompi C, Giuste F, Shi W, et al. Respiratory Markers Significantly Enhance Anxiety Detection Using Multimodal Physiological Sensing. In: IEEE EMBS International Conference on Biomedical and Health Informatics
-
[38]
p. 1–4. doi: 10.1109/BHI50953.2021.9508589
-
[39]
Spontaneous Breathing Rate Variations Linked to Social Exclusion and Emotion Self-assessment
Hidalgo-Muñoz A, Cuadrado E, Castillo-Mayén R, Luque B, Tabernero C. Spontaneous Breathing Rate Variations Linked to Social Exclusion and Emotion Self-assessment. Applied Psychophysiology and Biofeedback. 2022;47:1–7. doi:10.1007/s10484-022-09551-5
-
[40]
Toward machine emotional intelligence: analysis of affective physiological state
Picard RW, Vyzas E, Healey J. Toward machine emotional intelligence: analysis of affective physiological state. IEEE Transactions on Pattern Analysis and Machine Intelligence. 2001;23(10):1175–1191. doi:10.1109/34.954607
-
[41]
Bardeen J, Tull M, Stevens E, Gratz K. Further Investigation of the Association between Anxiety Sensitivity and Posttraumatic Stress Disorder: Examining the Influence of Emotional Avoidance. Journal of Contextual Behavioral Science. 2015;4. doi:10.1016/j.jcbs.2015.05.002
-
[42]
Psychometric properties of the PTSD Checklist with older primary care patients
Cook J, Elhai J, Areán P. Psychometric properties of the PTSD Checklist with older primary care patients. Journal of traumatic stress. 2005;18:371–6. doi:10.1002/jts.20038
-
[43]
Screening for Posttraumatic Stress Disorder in V A Primary Care Patients with Depression Symptoms
Gerrity M, Corson K, Dobscha S. Screening for Posttraumatic Stress Disorder in V A Primary Care Patients with Depression Symptoms. Journal of general internal medicine. 2007;22:1321–4. doi:10.1007/s11606-007-0290-5
-
[44]
Bauer E. P. Sex differences in fear responses: Neural circuits. Neuropharmacology. 2023;222:109298. doi:10.1016/j.neuropharm.2022.109298
-
[45]
Hyndman, R., Bashtannyk, D. & Grunwald, G. Estimating and visualizing conditional densities.J. Comput. Graph. Stat.5, 315–336 (1996). doi: 10.1080/10618600.1996.10474715. 45.Nadaraya, E. A. On estimating regression.Theory Probab. & Its Appl.9, 141–142, 1964. doi:10.1137/1109020. 46.Watson, G. Smooth regression analysis.Sankhya: The Indian J. Stat.A, 359–3...
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.