Simultaneous hyperkinetic movement disorders phenotyping: a cross-cohort pediatric transfer study using routine videos, markerless pose estimation and a tabular foundation model
Pith reviewed 2026-06-28 02:09 UTC · model grok-4.3
The pith
A video framework detects eight hyperkinetic movement disorders at once and transfers from adults to children after calibrating only the final decision layer.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
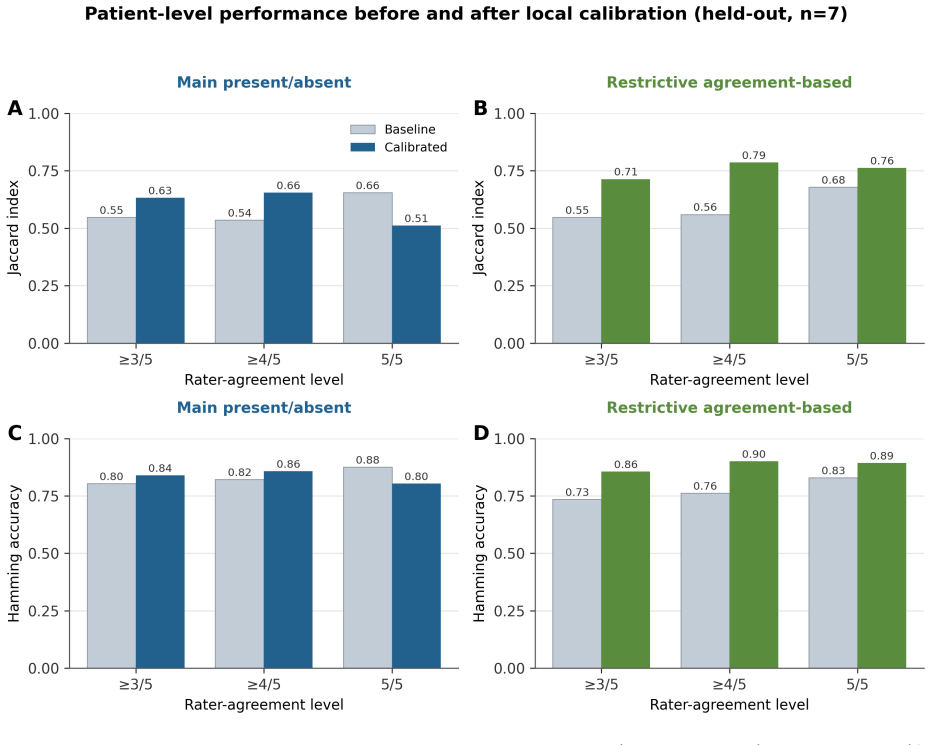
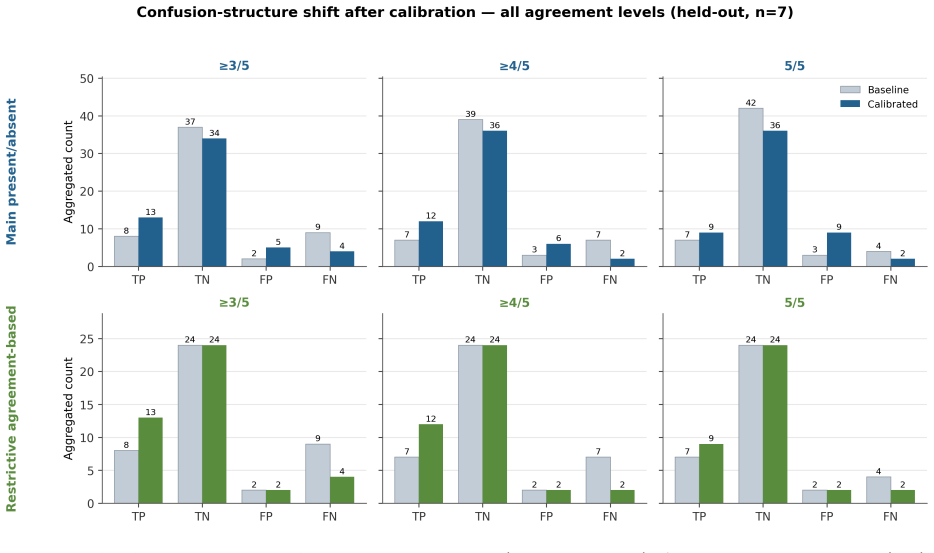
After training a shared predictive backbone on 21 adults and 4 controls, the system is deployed unchanged on 12 pediatric patients with monogenic combined movement disorders; lightweight calibration of only the final decision layer on a clinician-selected subset raises Hamming accuracy from 0.804 to 0.839 and Jaccard index from 0.548 to 0.633 on the seven held-out pediatric cases, with further gains when restricted to phenomenologies showing higher clinician agreement.
What carries the argument
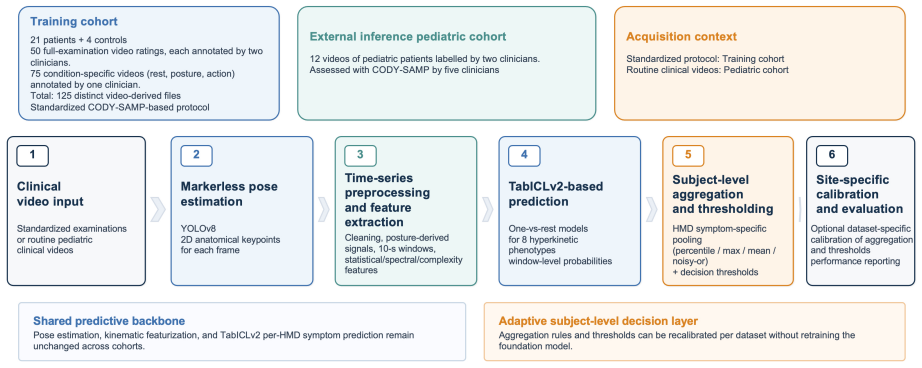
Markerless pose estimation producing kinematic descriptors that feed a pretrained tabular foundation model, followed by lightweight calibration restricted to the final subject-level decision layer.
If this is right
- The same backbone supports simultaneous detection of all eight listed phenomenologies from a single routine video.
- Transfer to a new age group succeeds without retraining the pose estimation or foundation-model layers.
- Performance remains stable when evaluation is limited to the subset of labels with stronger clinician consensus.
- The approach works on real-world rather than protocol-controlled recordings in the external cohort.
Where Pith is reading between the lines
- Clinics could begin using the system on existing video archives with only a few local labels for calibration instead of collecting new large datasets.
- The same transfer pattern might apply to other video-based neurological assessments if the kinematic descriptors prove stable across conditions.
- Larger studies could test whether random or stratified calibration subsets produce comparable gains, clarifying how much clinician selection matters.
Load-bearing premise
The small clinician-selected subset used for calibration represents the full phenotypic range of the pediatric cohort without selection bias that would inflate measured transfer performance.
What would settle it
Run the same pipeline on a new pediatric cohort where the calibration subset is selected randomly rather than by clinician judgment and measure whether the accuracy gains disappear or reverse.
Figures
read the original abstract
Objective: To develop and externally test a video-based framework for simultaneous detection of hyperkinetic MDs phenomenologies: dystonia, tremor, myoclonus, chorea, athetosis, ballismus, stereotypies, and tics using routine clinical recordings, with explicit testing of external, cross-cohort transfer from adult to pediatric populations. Methods: In this proof-of-concept study, the framework combines markerless pose estimation, kinematic descriptors, and a pretrained fondation model. A shared predictive backbone was developed on 21 adults with confirmed hyperkinetic MDs and 4 healthy controls assessed under a standardized protocol. External validation was performed on an independent external cohort: a real-world pediatric sample (n=12, monogenic combined MDs). For the external dataset, the backbone was deployed without retraining; lightweight calibration adjusted only the final subject-level decision step using a small labeled subset of patients selected by clinicians as representative of the cohort's phenotypic range. Results: After local calibration of the decision layer on the clinician-selected subset, performance improved consistently on the held-out pediatric patients (n=7): Hamming accuracy rose from 0.804 to 0.839 and the Jaccard index from 0.548 to 0.633. This calibrated performance was preserved, and the Jaccard index further improved, when the evaluation was restricted to the phenomenologies with more definite clinician agreement (Hamming accuracy 0.9, Jaccard index 0.786), indicating that the gains did not rest on the least-reliable labels.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
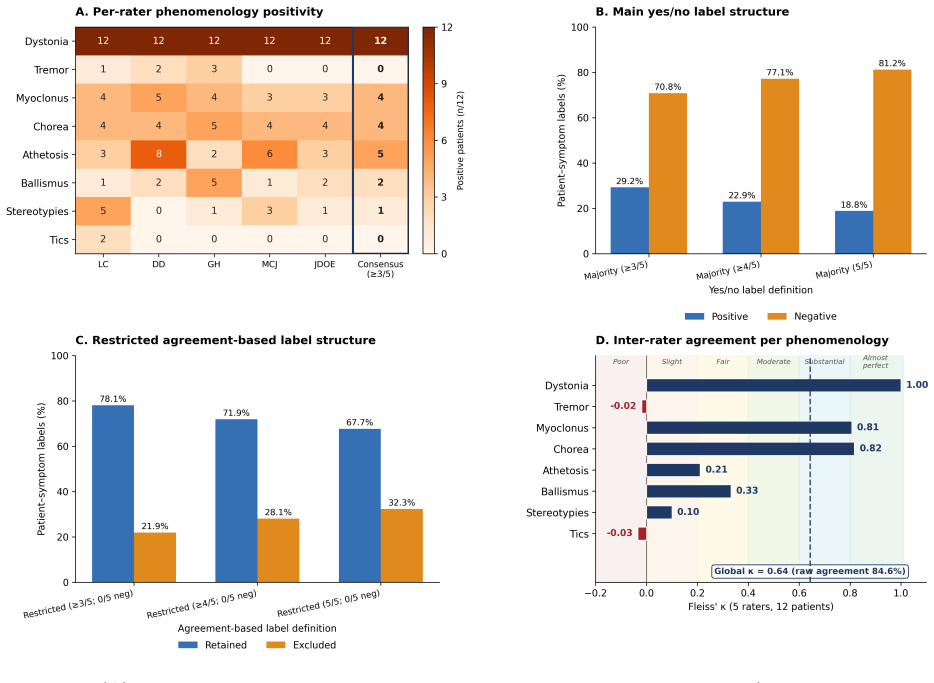
Summary. The manuscript presents a proof-of-concept video-based framework for simultaneous multi-label phenotyping of eight hyperkinetic movement disorders (dystonia, tremor, myoclonus, chorea, athetosis, ballismus, stereotypies, tics) from routine clinical recordings. It combines markerless pose estimation, kinematic descriptors, and a tabular foundation model. A shared backbone is trained on 21 adults plus 4 controls; external transfer is tested on an independent pediatric cohort (n=12 monogenic cases) by deploying the backbone without retraining and performing lightweight calibration of only the final subject-level decision layer on a clinician-selected subset, with metrics reported on the remaining n=7 held-out patients (post-calibration Hamming accuracy 0.839, Jaccard index 0.633).
Significance. If the calibration subset proves representative, the result would demonstrate feasible adult-to-pediatric transfer for rare combined movement disorders using minimal additional labels and routine videos, a practically relevant advance given data scarcity in pediatrics. The preservation of gains when restricting to high-agreement phenomenologies and the multi-label simultaneous detection are strengths that could support clinical utility if the small-sample concerns are addressed.
major comments (3)
- [Methods (external validation paragraph)] Methods (calibration and external validation): The headline performance lift (Hamming accuracy 0.804→0.839, Jaccard 0.548→0.633 on n=7) is obtained after calibration on a clinician-selected subset whose selection criteria, MD-type distribution, severity, or video-quality match to the held-out cases are not quantified or statistically compared; this leaves the improvement vulnerable to selection bias and undermines the claim of unbiased cross-cohort transfer.
- [Results (performance paragraph)] Results: No confidence intervals, p-values, or bootstrap variability estimates accompany the reported metrics despite n=12 total and n=7 test cases; the absence of these makes it impossible to determine whether the observed deltas exceed what could arise from sampling variability alone.
- [Abstract (Methods summary) and Methods (backbone description)] Abstract/Methods: No information is given on the foundation model's pretraining corpus, architecture details, or the exact set of kinematic descriptors extracted from pose estimation; these omissions are load-bearing for claims of reproducibility and for interpreting why transfer succeeded.
minor comments (2)
- [Abstract] Abstract: 'fondation model' is a typographical error and should read 'foundation model'.
- [Abstract (Results)] Abstract: The phrasing 'deployed without retraining' is accurate only for the backbone; the subsequent calibration step should be explicitly distinguished from zero-shot transfer to avoid reader confusion.
Simulated Author's Rebuttal
We thank the referee for the constructive feedback on our proof-of-concept study. We address each major comment below with honest responses and indicate revisions where the manuscript can be strengthened, while noting the constraints of small-sample rare-disease data.
read point-by-point responses
-
Referee: [Methods (external validation paragraph)] Methods (calibration and external validation): The headline performance lift (Hamming accuracy 0.804→0.839, Jaccard 0.548→0.633 on n=7) is obtained after calibration on a clinician-selected subset whose selection criteria, MD-type distribution, severity, or video-quality match to the held-out cases are not quantified or statistically compared; this leaves the improvement vulnerable to selection bias and undermines the claim of unbiased cross-cohort transfer.
Authors: We agree that the calibration subset requires fuller characterization to evaluate representativeness. In the revised manuscript we will add a supplementary table and text explicitly listing MD-type counts, clinician severity ratings, and video-quality descriptors for the calibration subset versus the n=7 held-out cases, together with any feasible descriptive comparisons. This directly addresses the selection-bias concern while preserving the proof-of-concept framing; we do not claim fully unbiased transfer but rather feasible lightweight adaptation. revision: yes
-
Referee: [Results (performance paragraph)] Results: No confidence intervals, p-values, or bootstrap variability estimates accompany the reported metrics despite n=12 total and n=7 test cases; the absence of these makes it impossible to determine whether the observed deltas exceed what could arise from sampling variability alone.
Authors: We accept that uncertainty estimates are needed. The revised Results section will report bootstrap confidence intervals (1000 resamples) for both Hamming accuracy and Jaccard index pre- and post-calibration on the held-out patients. Given n=7 we will not present p-values for the delta, as they would be under-powered and potentially misleading; instead we will frame the work as exploratory and highlight the observed variability. This provides the requested quantification without overstating statistical claims. revision: yes
-
Referee: [Abstract (Methods summary) and Methods (backbone description)] Abstract/Methods: No information is given on the foundation model's pretraining corpus, architecture details, or the exact set of kinematic descriptors extracted from pose estimation; these omissions are load-bearing for claims of reproducibility and for interpreting why transfer succeeded.
Authors: We acknowledge the reproducibility gap. The revised Methods (and a condensed Abstract sentence) will specify the tabular foundation model architecture, its pretraining corpus (large-scale public tabular datasets), and the complete list of kinematic descriptors (joint velocities, inter-joint angles, accelerations, and higher-order statistics derived from the pose keypoints). These details exist in our code and supplementary files and will be elevated to the main text. revision: yes
Circularity Check
No significant circularity in derivation chain
full rationale
The paper explicitly describes deploying the adult-trained backbone without retraining on the pediatric cohort, then performing lightweight calibration of only the final decision layer on a clinician-selected subset before reporting metrics on the separate held-out n=7 cases. This is a standard split-based calibration and evaluation procedure whose outputs are not equivalent to the inputs by construction. No self-definitional equations, fitted parameters renamed as predictions, load-bearing self-citations, uniqueness theorems, or ansatz smuggling are present in the abstract or described methods. The central transfer claim rests on external data splits rather than reducing to its own fitted values.
Axiom & Free-Parameter Ledger
free parameters (1)
- final decision layer weights
axioms (1)
- domain assumption Adult-trained backbone produces features that remain useful for pediatric cases without retraining the core model
Reference graph
Works this paper leans on
-
[1]
D., Parisi, F., Mancini, M
Stephen, C. D., Parisi, F., Mancini, M. & Artusi, C. A. Editorial: Digital biomarkers in movement disorders.Front. Neurol.16, 1600018 (2025)
2025
-
[2]
E., Tijssen, M
Brandsma, R., Van Egmond, M. E., Tijssen, M. A. J., & the Groningen Movement Disorder Expertise Centre. Diagnostic approach to paediatric movement disorders: a clinical practice guide.Dev. Med. Child Neurol.63, 252–258 (2021)
2021
-
[3]
& Edwards, M
Sadnicka, A. & Edwards, M. J. Between Nothing and Everything: Phenomenology in Move- ment Disorders.Mov. Disord.38, 1767–1773 (2023)
2023
-
[4]
Neu- rol.12, 659805 (2021)
Méneret, A.et al.Treatable Hyperkinetic Movement Disorders Not to Be Missed.Front. Neu- rol.12, 659805 (2021)
2021
-
[5]
Cif, L.et al.Deep Learning Pose Estimation for Multi-Label Recognition of Combined Hyper- kinetic Movement Disorders. Preprint at https://doi.org/10.48550/ARXIV.2602.00163 (2026)
work page internal anchor Pith review Pith/arXiv arXiv doi:10.48550/arxiv.2602.00163 2026
-
[6]
H., Azzopardi, G
Martínez-García-Peña, R., Koens, L. H., Azzopardi, G. & Tijssen, M. A. J. Video-Based Data-Driven Models for Diagnosing Movement Disorders: Review and Future Directions.Mov. Disord.40, 2046–2066 (2025)
2046
-
[7]
Tang, W., Van Ooijen, P. M. A., Sival, D. A. & Maurits, N. M. Automatic two-dimensional & three-dimensional video analysis with deep learning for movement disorders: A systematic review.Artif. Intell. Med.156, 102952 (2024)
2024
-
[8]
Nature637, 319–326 (2025)
Hollmann, N.et al.Accurate predictions on small data with a tabular foundation model. Nature637, 319–326 (2025)
2025
-
[9]
TabICLv2: A better, faster, scalable, and open tabular foundation model.arXiv:2602.11139, 2026
Qu, J., Holzmüller, D., Varoquaux, G. & Morvan, M. L. TabICLv2: A better, faster, scalable, and open tabular foundation model. Preprint at https://doi.org/10.48550/ARXIV.2602.11139 (2026)
-
[10]
TabICL: A Tabular Foundation Model for In-Context Learning on Large Data
Qu, J., Holzmüller, D., Varoquaux, G. & Morvan, M. L. TabICL: A Tab- ular Foundation Model for In-Context Learning on Large Data. Preprint at https://doi.org/10.48550/ARXIV.2502.05564 (2025)
work page internal anchor Pith review Pith/arXiv arXiv doi:10.48550/arxiv.2502.05564 2025
-
[11]
Approach to an irregular time series on the basis of the fractal theory.Phys
Higuchi, T. Approach to an irregular time series on the basis of the fractal theory.Phys. Nonlinear Phenom.31, 277–283 (1988)
1988
-
[12]
& Pompe, B
Bandt, C. & Pompe, B. Permutation Entropy: A Natural Complexity Measure for Time Series. Phys. Rev. Lett.88, 174102 (2002)
2002
-
[13]
Methods17, 261–272 (2020)
Virtanen, P.et al.SciPy 1.0: fundamental algorithms for scientific computing in Python.Nat. Methods17, 261–272 (2020). 24
2020
-
[14]
M., Marsili, L., Espay, A
Pecoraro, P. M., Marsili, L., Espay, A. J., Bologna, M. & Di Biase, L. Computer Vision Technologies in Movement Disorders: A Systematic Review.Mov. Disord. Clin. Pract.12, 1229–1243 (2025)
2025
-
[15]
A., Išgum, I
Zuluaga, M. A., Išgum, I. & Bach Cuadra, M. Trustworthy AI in medical image analysis: A unified perspective built on robustness and layers of trust.Curr. Opin. Biomed. Eng.37, 100649 (2026)
2026
-
[16]
Silva, G. F. D. S., Barcellos Filho, F. N., Wichmann, R. M., Da Silva Junior, F. C. & Chiave- gatto Filho, A. D. P. Strategies for detecting and mitigating dataset shift in machine learning for health predictions: A systematic review.J. Biomed. Inform.170, 104902 (2025)
2025
-
[17]
arXiv preprint arXiv:2507.03971 , year=
Garg, A.et al.Real-TabPFN: Improving Tabular Foundation Models via Continued Pre- training With Real-World Data. Preprint at https://doi.org/10.48550/ARXIV.2507.03971 (2025). 25
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.