ReTAMamba: Reliability-Aware Temporal Aggregation with Mamba for Irregular Clinical Time Series Prediction
Pith reviewed 2026-05-20 22:08 UTC · model grok-4.3
The pith
ReTAMamba improves irregular clinical time series prediction by estimating observation reliability and temporal freshness.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
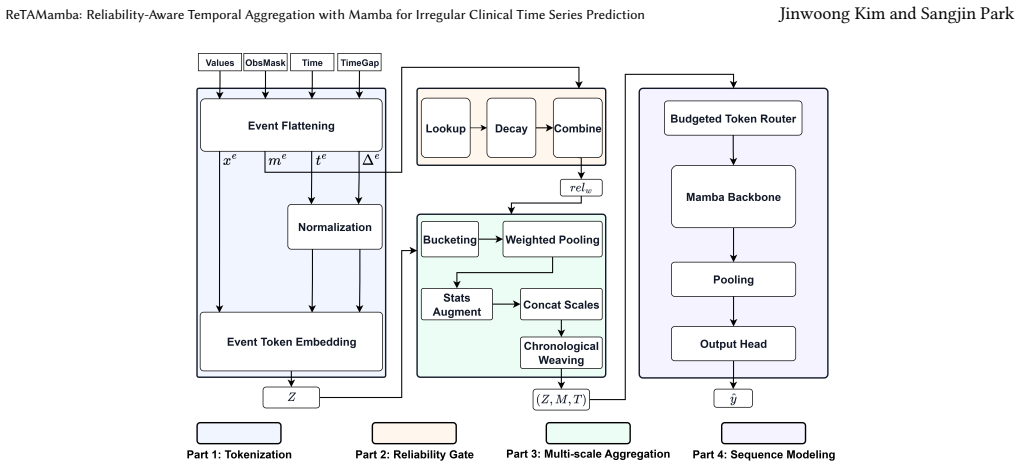
ReTAMamba reconstructs clinical time series as time-variable token sequences, estimates observation reliability from missingness and elapsed time, augments interval summaries with statistical descriptors, integrates short- and long-term temporal information using Chronological Weaving, and applies a budgeted token router to constrain sequence length. On MIMIC-IV, eICU, and PhysioNet 2012 this produces average relative AUPRC gains of 7.51 percent, 7.80 percent, and 10.15 percent respectively. The learned mean decay for dynamic signals such as heart rate and blood pressure is 24.3 percent larger than for relatively static laboratory variables.
What carries the argument
Reliability-aware temporal aggregation inside a Mamba backbone, driven by Chronological Weaving that merges multi-resolution temporal summaries while respecting observation age and completeness.
If this is right
- Prediction performance rises when models explicitly track information freshness and observation timeliness in addition to the measured values themselves.
- Learned decay rates differ systematically, being larger for dynamic vital signs than for static laboratory results.
- Reconstructing irregular series as token sequences with reliability estimates outperforms conventional mask-and-gap methods.
- A budgeted token router allows the approach to handle long clinical records without excessive memory cost.
Where Pith is reading between the lines
- The same reliability and weaving structure could be tested on irregular sensor streams outside medicine, such as environmental or industrial monitoring.
- The per-variable decay parameters might be inspected by clinicians to decide how often to repeat measurements for fast-changing versus stable signals.
- Prospective deployment on live hospital data streams would reveal whether the gains persist without periodic retraining.
Load-bearing premise
The reliability scores derived from missingness and elapsed time, together with Chronological Weaving, capture the clinically relevant temporal dynamics without creating new biases in the learned decay rates.
What would settle it
Reproduce the experiments on a fresh hold-out cohort from the same data sources and find no statistically significant AUPRC improvement over strong baselines, or find that the estimated decay rates show no consistent difference between dynamic and static clinical variables.
Figures


read the original abstract
Clinical time-series data are difficult to model with methods designed for regular sequences because they exhibit irregular sampling, frequent missing values, and heterogeneous observation patterns across variables. Existing approaches commonly use observation masks and time-gap information, but they do not continuously capture the decaying reliability of past observations or consistently organize multi-resolution information within a coherent temporal context during aggregation. To address these limitations, we propose Reliability-aware Temporal Aggregation with Mamba (ReTAMamba), which reconstructs clinical time series as time-variable token sequences, estimates observation reliability from missingness and elapsed time, and augments interval summaries with statistical descriptors. Chronological Weaving is used to integrate short- and long-term temporal information within a coherent temporal context, and a budgeted token router is applied to constrain sequence length while preserving informative summaries. Experiments on MIMIC-IV, eICU, and PhysioNet 2012 show that ReTAMamba consistently improves AUPRC over strong baselines, with average relative gains of 7.51%, 7.80%, and 10.15%, respectively. Cohort-level and patient-level analyses on eICU further showed that the learned mean decay for more dynamic signals, such as heart rate and blood pressure, was 24.3% larger than that for relatively static signals, such as laboratory test variables. These findings suggest that effective prediction in irregular clinical time series requires modeling not only what was measured, but also when and how it was observed, including information freshness and observation timeliness.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The paper proposes ReTAMamba for irregular clinical time series prediction. It reconstructs series as time-variable token sequences, estimates observation reliability from missingness and elapsed time, augments interval summaries with statistical descriptors, applies Chronological Weaving to integrate short- and long-term context, and uses a budgeted token router to constrain length. Experiments on MIMIC-IV, eICU, and PhysioNet 2012 report relative AUPRC gains of 7.51%, 7.80%, and 10.15% over baselines, plus a post-hoc finding that learned mean decay is 24.3% larger for dynamic signals (e.g., HR, BP) than static lab variables.
Significance. If the AUPRC gains can be causally attributed to the reliability estimation and Chronological Weaving rather than the Mamba backbone or token router, the work would usefully extend mask-and-gap methods by explicitly modeling observation freshness and timeliness in clinical data. The multi-dataset evaluation and cohort-level decay analysis provide a starting point for such claims, though current evidence remains correlational.
major comments (2)
- [Experiments] Experiments section: No ablation studies isolate the reliability estimation (from missingness and elapsed time) or Chronological Weaving while holding the Mamba backbone and budgeted router fixed. Without these, the headline relative AUPRC gains cannot be attributed to the proposed components rather than the sequence model or summarization, directly undermining the central contrast with existing mask-and-gap approaches.
- [Abstract and results] Abstract and results: The reported AUPRC improvements lack error bars, statistical significance tests, or variance across runs. This makes it impossible to assess whether the 7.51–10.15% relative gains are robust or could arise from random variation, which is load-bearing for any claim of consistent improvement.
minor comments (2)
- [Abstract] The abstract refers to 'strong baselines' without naming them or citing their original papers; this should be expanded in the experimental setup for reproducibility.
- [Cohort-level analysis] The post-hoc decay-rate analysis on eICU is presented without controls for optimization dynamics or dataset-specific artifacts, weakening its interpretive value even as supporting evidence.
Simulated Author's Rebuttal
We thank the referee for the constructive comments and the opportunity to strengthen the manuscript. We address each major comment below, clarifying our experimental design and committing to revisions that directly respond to the concerns about attribution and statistical robustness.
read point-by-point responses
-
Referee: [Experiments] Experiments section: No ablation studies isolate the reliability estimation (from missingness and elapsed time) or Chronological Weaving while holding the Mamba backbone and budgeted router fixed. Without these, the headline relative AUPRC gains cannot be attributed to the proposed components rather than the sequence model or summarization, directly undermining the central contrast with existing mask-and-gap approaches.
Authors: We agree that isolating the contributions of reliability estimation and Chronological Weaving is essential for causal attribution. The current experiments compare against strong mask-and-gap baselines that use different sequence models, but do not hold the Mamba backbone and router fixed while ablating only the proposed components. In the revision we will add targeted ablation studies that disable reliability decay modeling and Chronological Weaving individually (and jointly) while retaining the identical Mamba architecture and budgeted token router. These results will be reported in a new subsection of the Experiments section with corresponding tables, allowing direct quantification of each component's impact and a clearer contrast to prior mask-and-gap methods. revision: yes
-
Referee: [Abstract and results] Abstract and results: The reported AUPRC improvements lack error bars, statistical significance tests, or variance across runs. This makes it impossible to assess whether the 7.51–10.15% relative gains are robust or could arise from random variation, which is load-bearing for any claim of consistent improvement.
Authors: We acknowledge that the absence of error bars and significance testing limits the strength of the reported gains. The manuscript currently presents single-run point estimates. In the revised version we will rerun all experiments across at least five random seeds, report mean AUPRC with standard deviations and error bars in all tables and the abstract, and include statistical significance tests (paired t-tests or Wilcoxon signed-rank tests with p-values) comparing ReTAMamba against each baseline. These additions will be placed in the Results section and reflected in the abstract summary of relative gains. revision: yes
Circularity Check
No circularity in empirical performance claims
full rationale
The paper advances an empirical architecture (ReTAMamba) for irregular clinical time series and reports relative AUPRC gains on three public benchmarks. No closed-form derivation, uniqueness theorem, or fitted-parameter prediction is presented that reduces to its own inputs by construction. The post-hoc decay-rate observation is a correlational analysis performed after training and does not constitute a load-bearing prediction. Any self-citations are incidental and not required to justify the central empirical result, which remains falsifiable against external baselines.
Axiom & Free-Parameter Ledger
Lean theorems connected to this paper
-
IndisputableMonolith/Cost/FunctionalEquation.leanwashburn_uniqueness_aczel echoes?
echoesECHOES: this paper passage has the same mathematical shape or conceptual pattern as the Recognition theorem, but is not a direct formal dependency.
reliability weight ... rel_w,i = m_e_i + (1-m_e_i) exp(-λ_v_e_i Δ_e_i) ... variable-specific decay rate
What do these tags mean?
- matches
- The paper's claim is directly supported by a theorem in the formal canon.
- supports
- The theorem supports part of the paper's argument, but the paper may add assumptions or extra steps.
- extends
- The paper goes beyond the formal theorem; the theorem is a base layer rather than the whole result.
- uses
- The paper appears to rely on the theorem as machinery.
- contradicts
- The paper's claim conflicts with a theorem or certificate in the canon.
- unclear
- Pith found a possible connection, but the passage is too broad, indirect, or ambiguous to say the theorem truly supports the claim.
Reference graph
Works this paper leans on
-
[1]
Idar Johan Brekke, Lars Håland Puntervoll, Peter Bank Pedersen, John Kellett, and Mikkel Brabrand. 2019. The Value of Vital Sign Trends in Predicting and Monitoring Clinical Deterioration: A Systematic Review.PloS One14, 1 (2019), e0210875
work page 2019
-
[2]
Zhengping Che, Sanjay Purushotham, Kyunghyun Cho, David Sontag, and Yan Liu. 2018. Recurrent Neural Networks for Multivariate Time Series with Missing Values.Scientific Reports8, 1 (2018), 6085
work page 2018
-
[3]
Tianqi Chen and Carlos Guestrin. 2016. XGBoost: A Scalable Tree Boosting System. InProceedings of the 22nd ACM SIGKDD International Conference on Knowledge Discovery and Data Mining. 785–794
work page 2016
-
[4]
Matthew M Churpek, Richa Adhikari, and Dana P Edelson. 2016. The Value of Vital Sign Trends for Detecting Clinical Deterioration on the Wards.Resuscitation 102 (2016), 1–5
work page 2016
-
[5]
Marzyeh Ghassemi, Marco Pimentel, Tristan Naumann, Thomas Brennan, David Clifton, Peter Szolovits, and Mengling Feng. 2015. A Multivariate Timeseries Modeling Approach to Severity of Illness Assessment and Forecasting in ICU with Sparse, Heterogeneous Clinical Data. InProceedings of the AAAI Conference on Artificial Intelligence, Vol. 29
work page 2015
-
[6]
Rolf HH Groenwold. 2020. Informative Missingness in Electronic Health Record Systems: The Curse of Knowing.Diagnostic and Prognostic Research4, 1 (2020), 8
work page 2020
-
[7]
Albert Gu and Tri Dao. 2024. Mamba: Linear-Time Sequence Modeling with Selective State Spaces. InFirst Conference on Language Modeling
work page 2024
-
[8]
Hrayr Harutyunyan, Hrant Khachatrian, David C Kale, Greg Ver Steeg, and Aram Galstyan. 2019. Multitask Learning and Benchmarking with Clinical Time Series Data.Scientific Data6, 1 (2019), 96
work page 2019
-
[9]
Sepp Hochreiter and Jürgen Schmidhuber. 1997. Long Short-Term Memory. Neural Computation9, 8 (1997), 1735–1780
work page 1997
-
[10]
Max Horn, Michael Moor, Christian Bock, Bastian Rieck, and Karsten Borgwardt
-
[11]
InInternational Conference on Machine Learning
Set Functions for Time Series. InInternational Conference on Machine Learning. PMLR, 4353–4363
-
[12]
Alistair EW Johnson, Lucas Bulgarelli, Lu Shen, Alvin Gayles, Ayad Shammout, Steven Horng, Tom J Pollard, Sicheng Hao, Benjamin Moody, and Brian Gow
-
[13]
MIMIC-IV, a Freely Accessible Electronic Health Record Dataset.Scientific Data10, 1 (2023), 1
work page 2023
- [14]
-
[15]
Eric Kipnis, Davinder Ramsingh, Maneesh Bhargava, Erhan Dincer, Maxime Cannesson, Alain Broccard, Benoit Vallet, Karim Bendjelid, and Ronan Thibault
-
[16]
Monitoring in the Intensive Care.Critical Care Research and Practice2012, 1 (2012), 473507
work page 2012
-
[17]
Sangho Lee, Kyeongseo Min, Youngdoo Son, and Hyungrok Do. 2025. Adaptive Time Encoding for Irregular Multivariate Time-Series Classification. InThe Thirty-Ninth Annual Conference on Neural Information Processing Systems
work page 2025
-
[18]
Zekun Li, Shiyang Li, and Xifeng Yan. 2023. Time series as images: Vision transformer for irregularly sampled time series.Advances in Neural Information Processing Systems36 (2023), 49187–49204
work page 2023
-
[19]
Zachary C Lipton, David C Kale, Charles Elkan, and Randall Wetzel. 2015. Learning to Diagnose with LSTM Recurrent Neural Networks.arXiv preprint arXiv:1511.03677(2015)
work page internal anchor Pith review Pith/arXiv arXiv 2015
-
[20]
Jiexi Liu, Meng Cao, and Songcan Chen. 2026. Beyond Observations: Reconstruc- tion Error-Guided Irregularly Sampled Time Series Representation Learning. In Proceedings of the AAAI Conference on Artificial Intelligence, Vol. 40. 23712–23720
work page 2026
-
[21]
Junchao Ma, Donald KK Lee, Michael E Perkins, Margaret A Pisani, and Edieal Pinker. 2019. Using the Shapes of Clinical Data Trajectories to Predict Mortality in ICUs.Critical Care Explorations1, 4 (2019), e0010
work page 2019
-
[22]
Tom J Pollard, Alistair EW Johnson, Jesse D Raffa, Leo A Celi, Roger G Mark, and Omar Badawi. 2018. The eICU Collaborative Research Database, a Freely Available Multi-Center Database for Critical Care Research.Scientific Data5, 1 (2018), 180178
work page 2018
-
[23]
Sarah Pungitore and Vignesh Subbian. 2023. Assessment of Prediction Tasks and Time Window Selection in Temporal Modeling of Electronic Health Record Data: A Systematic Review.Journal of Healthcare Informatics Research7, 3 (2023), 313–331
work page 2023
-
[24]
Hiroaki Sakoe and Seibi Chiba. 1978. Dynamic Programming Algorithm Opti- mization for Spoken Word Recognition.IEEE Transactions on Acoustics, Speech, and Signal Processing26, 1 (1978), 43–49
work page 1978
-
[25]
Pavel Senin. 2008. Dynamic Time Warping Algorithm Review.Information and Computer Science Department, University of Hawaii at Manoa855, 1-23 (2008), 40
work page 2008
-
[26]
Junming Shi, Alan E Hubbard, Nicholas Fong, and Romain Pirracchio. 2025. Implicit Bias in ICU Electronic Health Record Data: Measurement Frequencies and Missing Data Rates of Clinical Variables.BMC Medical Informatics and Decision Making25, 1 (2025), 241
work page 2025
- [27]
- [28]
-
[29]
Ikaro Silva, George Moody, Daniel J Scott, Leo A Celi, and Roger G Mark. 2012. Predicting In-Hospital Mortality of ICU Patients: The PhysioNet/Computing in Cardiology Challenge 2012. In2012 Computing in Cardiology. IEEE, 245–248
work page 2012
-
[30]
Rose Sisk, Lijing Lin, Matthew Sperrin, Jessica K Barrett, Brian Tom, Karla Diaz-Ordaz, Niels Peek, and Glen P Martin. 2021. Informative Presence and Observation in Routine Health Data: A Review of Methodology for Clinical Risk Prediction.Journal of the American Medical Informatics Association28, 1 (2021), 155–166
work page 2021
-
[31]
Amelia LM Tan, Emily J Getzen, Meghan R Hutch, Zachary H Strasser, Alba Gutiérrez-Sacristán, Trang T Le, Arianna Dagliati, Michele Morris, David A Hanauer, and Bertrand Moal. 2023. Informative Missingness: What Can We Learn from Patterns in Missing Laboratory Data in the Electronic Health Record? Journal of Biomedical Informatics139 (2023), 104306
work page 2023
-
[32]
Ashish Vaswani, Noam Shazeer, Niki Parmar, Jakob Uszkoreit, Llion Jones, Aidan N Gomez, Łukasz Kaiser, and Illia Polosukhin. 2017. Attention Is All You Need. InAdvances in Neural Information Processing Systems, Vol. 30
work page 2017
-
[33]
Jiawen Zhang, Shun Zheng, Wei Cao, Jiang Bian, and Jia Li. 2023. Warpformer: A Multi-Scale Modeling Approach for Irregular Clinical Time Series. InProceedings of the 29th ACM SIGKDD Conference on Knowledge Discovery and Data Mining. 3273–3285
work page 2023
-
[34]
Shuai Zhang, Yin Yin Quan, and Juanhong Chen. 2024. Construction and Appli- cation of an ICU Nursing Electronic Medical Record Quality Control System in a Chinese Tertiary Hospital: A Prospective Controlled Trial.BMC Nursing23, 1 (2024), 493
work page 2024
- [35]
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.