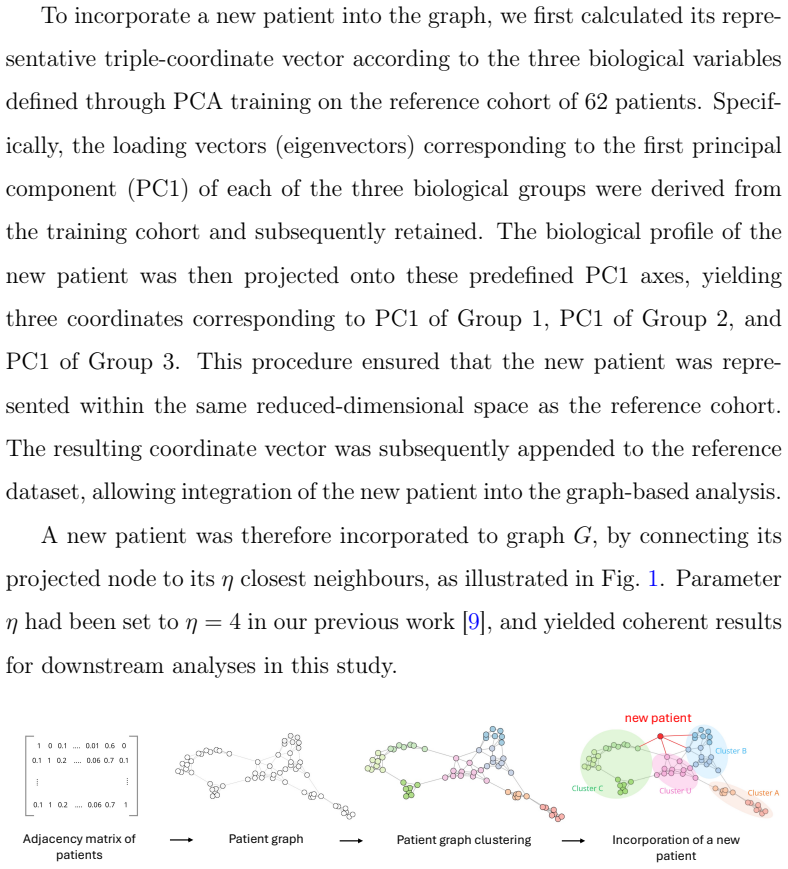
Graph-based analysis of inflammatory profiles in New Onset Refractory Status Epilepticus (NORSE)
Pith reviewed 2026-06-25 21:56 UTC · model grok-4.3
The pith
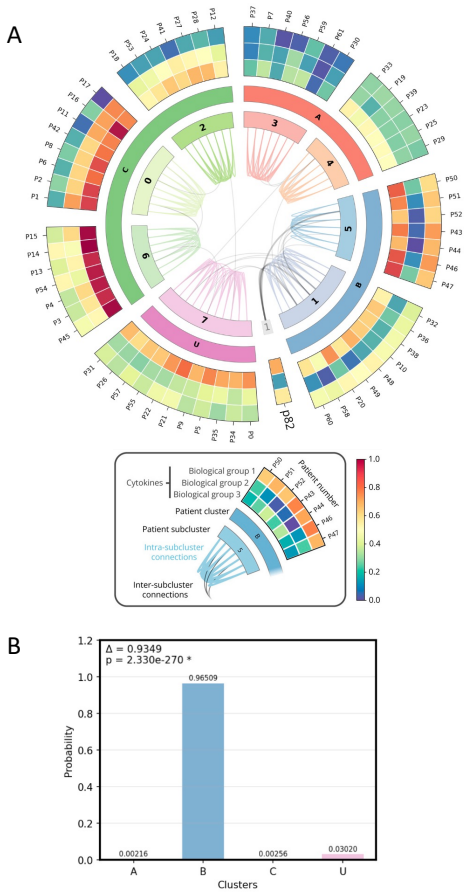
Graph clustering of 96-cytokine profiles from 62 cNORSE patients creates stable inflammatory groups that new cases can be assigned to with probability and confidence scores.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
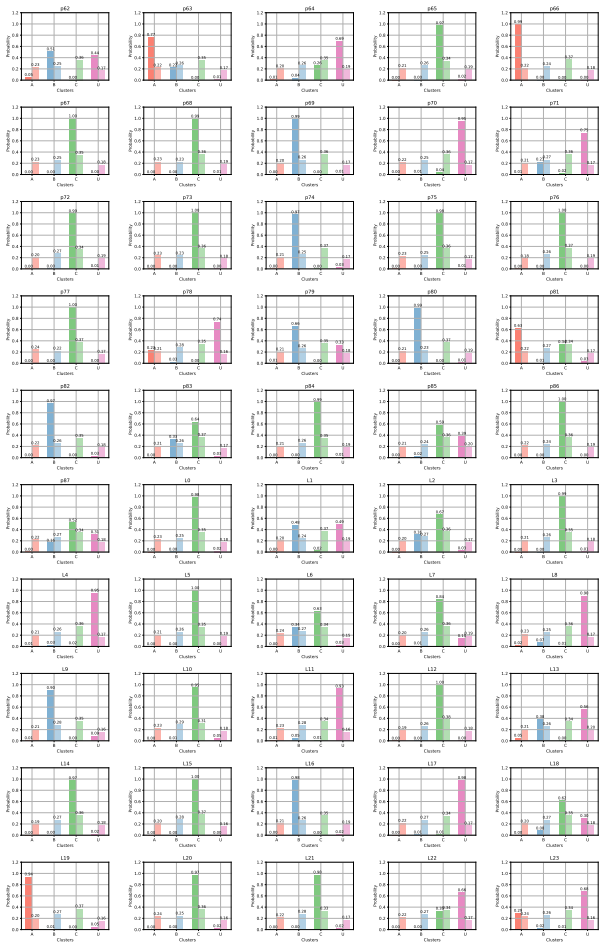
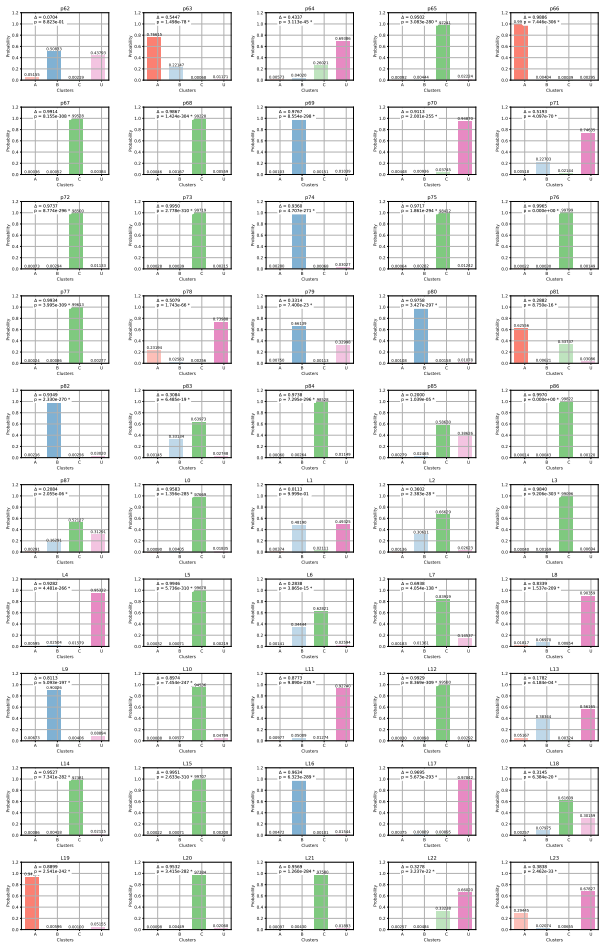
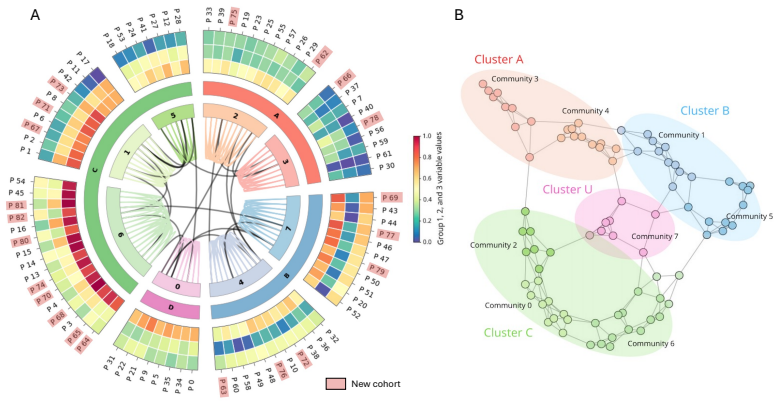
Building on graph clustering that identified biologically validated inflammatory groups in a 62-patient cohort with 96-cytokine serum profiles, the authors construct attribution models that assign new profiles to these groups while supplying probability and confidence values; Monte-Carlo simulations and parametric tests quantify the reliability of each assignment, and the framework is packaged as a clinician-friendly interface that supports both single-timepoint classification and longitudinal trajectory tracking.
What carries the argument
Graph clustering on 96-cytokine profiles followed by tailored attribution models that compute group membership probability and statistical confidence via Monte-Carlo simulations and custom parametric tests.
If this is right
- Clinicians receive a most-likely inflammatory cluster, attribution probability, and confidence score for each new cytokine panel within seconds.
- Longitudinal cytokine measurements can be mapped onto the same clusters to monitor how a patient's inflammatory state evolves.
- The framework supplies a concrete route toward matching individual patients to specific immunomodulatory therapies based on cluster membership.
Where Pith is reading between the lines
- If the clusters prove reproducible across centers, the same attribution machinery could be applied to other cryptogenic inflammatory encephalopathies that also show cytokine heterogeneity.
- The method supplies a ready-made stratification variable that future clinical trials of immunotherapy in status epilepticus could use to enrich for likely responders.
- Because the output includes explicit confidence values, the approach naturally supports a 'watch-and-wait' strategy for borderline cases rather than immediate treatment escalation.
Load-bearing premise
The inflammatory clusters found by graph clustering in the original 62-patient cohort are biologically distinct and stable enough that new, unseen profiles can be reliably assigned to them.
What would settle it
An independent cohort of cNORSE patients whose cytokine profiles are run through the attribution model yields low probabilities or confidence scores for every cluster, or the clusters themselves change when the original cohort is re-clustered after adding new data.
Figures
read the original abstract
Background and Objectives: Cryptogenic new-onset refractory status epilepticus (cNORSE) represents one of the most severe forms of status epilepticus, occurring in patients without prior neurological disease, and remaining of unknown aetiology despite extensive diagnostic evaluation. Emerging evidence supports a role for immune dysregulation in cNORSE; however, marked heterogeneity in inflammatory signatures has been reported, complicating the selection of targeted immunotherapies. Therefore, a critical need for tools facilitating the interpretation of cytokine panels exists. Methods: Building on the identification of distinct inflammatory groups of cNORSE patients using a graph clustering approach applied to a cohort of 62 patients with serum profiling of 96 cytokines, we tailored new models to quantify attribution probability to biologically validated clusters. Statistical assessment of the most informative model involved Monte-Carlo simulations and custom-developed parametric tests. Ultimately, we applied our framework to the implementation of a clinician-friendly interface for inflammatory profiling. Results: Our approach enables quick processing of several cytokine profiles, providing the most likely inflammatory cluster, associated attribution probability, and statistical confidence. For longitudinal assessments, the proposed method may also allow tracking the evolution of inflammatory trajectories over time. Conclusion: Systematic statistical characterization of the inflammatory heterogeneity in cNORSE requires the development of clinically actionable support tools. Our study offers a framework that may support personalized immunomodulatory strategies in cNORSE patients through clustering-based cytokine profiling.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript applies graph clustering to serum profiles of 96 cytokines from a 62-patient cNORSE cohort to identify inflammatory subgroups, develops attribution models that assign new profiles to these clusters together with probability and statistical-confidence estimates, validates the models via Monte-Carlo simulations and custom parametric tests, and implements a clinician-facing interface for rapid profiling and longitudinal tracking.
Significance. If the clusters are shown to be stable and the attribution generalizable, the framework could supply a concrete, statistically grounded tool for interpreting the marked inflammatory heterogeneity in cNORSE and thereby support individualized immunomodulatory decisions. The explicit use of Monte-Carlo simulations and parametric tests for the attribution step is a methodological strength that supplies quantifiable performance measures conditional on the discovered partition.
major comments (2)
- [Methods (graph clustering subsection)] Methods (graph clustering subsection): no cluster-stability diagnostics (bootstrap resampling, adjusted Rand index across resamples, or leave-one-out reproducibility) are reported for the 62-patient, 96-cytokine graph partition. With n=62 in a high-dimensional space, the absence of such checks directly undermines the assumption that the clusters are biologically fixed rather than sample-specific, which is load-bearing for any claim of reliable out-of-sample attribution.
- [Results (statistical assessment of attribution model)] Results (statistical assessment of attribution model): the Monte-Carlo simulations and parametric tests evaluate model performance conditional on the fixed clusters obtained from the full cohort; they do not test whether the underlying partition itself reappears under resampling. Consequently the reported attribution probabilities and confidence intervals for unseen profiles rest on an unverified premise.
minor comments (1)
- [Abstract] Abstract: the phrase 'biologically validated clusters' is used without stating the external criteria or independent data employed for that validation.
Simulated Author's Rebuttal
We thank the referee for the detailed and constructive review. The two major comments both concern the lack of explicit cluster-stability assessment. We agree that this is a substantive methodological gap for claims of generalizable attribution and will add the requested diagnostics in revision.
read point-by-point responses
-
Referee: [Methods (graph clustering subsection)] Methods (graph clustering subsection): no cluster-stability diagnostics (bootstrap resampling, adjusted Rand index across resamples, or leave-one-out reproducibility) are reported for the 62-patient, 96-cytokine graph partition. With n=62 in a high-dimensional space, the absence of such checks directly undermines the assumption that the clusters are biologically fixed rather than sample-specific, which is load-bearing for any claim of reliable out-of-sample attribution.
Authors: We acknowledge that the original Methods section did not include formal cluster-stability diagnostics. Although the graph construction and Louvain partitioning followed standard practice, the referee is correct that stability under resampling is required to support the downstream attribution claims. In the revised manuscript we will add a dedicated subsection describing (i) 1000 bootstrap resamples of the 62-patient cohort, (ii) computation of adjusted Rand indices between each resampled partition and the original partition, and (iii) leave-one-out reproducibility of cluster membership. These results, together with a stability summary table, will be reported in a new Results subsection. revision: yes
-
Referee: [Results (statistical assessment of attribution model)] Results (statistical assessment of attribution model): the Monte-Carlo simulations and parametric tests evaluate model performance conditional on the fixed clusters obtained from the full cohort; they do not test whether the underlying partition itself reappears under resampling. Consequently the reported attribution probabilities and confidence intervals for unseen profiles rest on an unverified premise.
Authors: The Monte-Carlo and parametric tests were intentionally conditioned on the observed partition because the immediate clinical goal was to assign new cytokine profiles to the clusters discovered in the present cohort. Nevertheless, the referee correctly notes that this leaves the stability of the partition itself untested. The bootstrap stability analysis described in response to the first comment will be used to quantify how often the same partition structure re-emerges; attribution probabilities and confidence intervals will then be reported both conditionally on the original partition and as averages across stable resamples, with the difference discussed explicitly. revision: yes
Circularity Check
No significant circularity detected
full rationale
The paper performs graph clustering on the 62-patient, 96-cytokine cohort to discover inflammatory groups, then constructs separate attribution models whose performance is evaluated via Monte-Carlo simulations and parametric tests. These steps are data-driven and externally assessed; the attribution probabilities are not shown to be equivalent to the clustering inputs by construction, nor do any load-bearing claims reduce to self-citations or fitted parameters renamed as predictions. The derivation chain is therefore self-contained against the described benchmarks.
Axiom & Free-Parameter Ledger
Reference graph
Works this paper leans on
-
[1]
Trinka, H
E. Trinka, H. Cock, D. Hesdorffer, A. O. Rossetti, I. E. Scheffer, S. Shin- nar, S. Shorvon, D. H. Lowenstein, A definition and classification of status epilepticus–report of the ilae task force on classification of status epilepticus, Epilepsia 56 (10) (2015) 1515–1523
2015
-
[2]
L. J. Hirsch, N. Gaspard, A. van Baalen, R. Nabbout, S. Demeret, T. Loddenkemper, V. Navarro, N. Specchio, L. Lagae, A. O. Rossetti, et al., Proposed consensus definitions for new-onset refractory status epilepticus (norse), febrile infection-related epilepsy syndrome (fires), and related conditions, Epilepsia 59 (4) (2018) 739–744
2018
-
[3]
Périn, W
B. Périn, W. Szurhaj, New onset refractory status epilepticus: state of the art, Revue Neurologique 178 (1-2) (2022) 74–83
2022
-
[4]
Carson, C
R. Carson, C. M. Stredny, Severe, refractory seizures: new-onset refrac- tory status epilepticus and febrile infection-related epilepsy syndrome, Medical Clinics 108 (1) (2024) 201–213
2024
-
[5]
Tharmaraja, J
T. Tharmaraja, J. S. Y. Ho, A. Neligan, S. Rajakulendran, The etiol- ogy and mortality of new-onset refractory status epilepticus (norse) in 31 adults: a systematic review and meta-analysis, Epilepsia 64 (5) (2023) 1113–1124
2023
-
[6]
Wickström, O
R. Wickström, O. Taraschenko, R. Dilena, E. T. Payne, N. Specchio, R. Nabbout, S. Koh, N. Gaspard, L. J. Hirsch, I. N. C. Group, et al., International consensus recommendations for management of new onset refractory status epilepticus (norse) including febrile infection-related epilepsy syndrome (fires): summary and clinical tools, Epilepsia 63 (11) (2022...
2022
-
[7]
Hanin, E
A. Hanin, E. Muscal, L. J. Hirsch, Second-line immunotherapy in new onset refractory status epilepticus, Epilepsia 65 (5) (2024) 1203–1223
2024
-
[8]
Hanin, J
A. Hanin, J. Cespedes, K. Dorgham, Y. Pulluru, M. Gopaul, G. Goro- chov, D. A. Hafler, V. Navarro, N. Gaspard, L. J. Hirsch, Cytokines in new-onset refractory status epilepticus predict outcomes, Annals of Neurology 94 (1) (2023) 75–90
2023
-
[9]
Guillemaud, M
M. Guillemaud, M. Chavez, F. Kobeissy, A. Vezzani, A. D. Jimenez, M. M. Basha, A. Batra, S. Demeret, O. Eka, K. Eschbach, et al., Iden- tification of distinct biological groups of patients with cryptogenic norse via inflammatory profiling, Neurology: Neuroimmunology & Neuroin- flammation 12 (4) (2025) e200403
2025
-
[10]
S. F. Seys, H. Scheers, P. Van den Brande, G. Marijsse, E. Dilissen, A. Van Den Bergh, P. C. Goeminne, P. W. Hellings, J. L. Ceuppens, L. J. Dupont, et al., Cluster analysis of sputum cytokine-high profiles 32 reveals diversity in t (h) 2-high asthma patients, Respiratory Research 18 (1) (2017) 39
2017
-
[11]
Y. Wang, R. B. Meagher, S. Ambati, H. Cheng, P. Ma, B. G. Phillips, Patients with obstructive sleep apnea have altered levels of four cy- tokines associated with cardiovascular and kidney disease, but near nor- mal levels with airways therapy, Nature and Science of Sleep (2021) 457–466
2021
-
[12]
Bañales-Méndez, M
L.Barrera, E.Montes-Servín, A.Barrera, L.Ramírez-Tirado, F.Salinas- Parra, J. Bañales-Méndez, M. Sandoval-Ríos, Ó. Arrieta, Cytokine pro- file determined by data-mining analysis set into clusters of non-small-cell lung cancer patients according to prognosis, Annals of Oncology 26 (2) (2015) 428–435
2015
-
[13]
J. H. Turner, R. K. Chandra, P. Li, K. Bonnet, D. G. Schlundt, Identifi- cation of clinically relevant chronic rhinosinusitis endotypes using cluster analysis of mucus cytokines, Journal of Allergy and Clinical Immunology 141 (5) (2018) 1895–1897
2018
-
[14]
J. Bai, C. Wu, D. Zhong, D. Xu, Q. Wang, X. Zeng, Hierarchical clus- ter analysis of cytokine profiles reveals a cutaneous vasculitis-associated subgroup in dermatomyositis, Clinical Rheumatology 40 (3) (2021) 999– 1008
2021
-
[15]
Tomassen, G
P. Tomassen, G. Vandeplas, T. Van Zele, L.-O. Cardell, J. Arebro, H. Olze, U. Förster-Ruhrmann, M. L. Kowalski, A. Olszewska-Ziąber, G. Holtappels, et al., Inflammatory endotypes of chronic rhinosinusitis 33 based on cluster analysis of biomarkers, Journal of Allergy and Clinical Immunology 137 (5) (2016) 1449–1456
2016
-
[16]
J. C. Morse, M. H. Shilts, K. A. Ely, P. Li, Q. Sheng, L.-C. Huang, T. J. Wannemuehler, N. I. Chowdhury, R. K. Chandra, S. R. Das, et al., Patterns of olfactory dysfunction in chronic rhinosinusitis identified by hierarchical cluster analysis and machine learning algorithms, Interna- tional Forum of Allergy & Rhinology 9 (3) (2019) 255–264
2019
-
[17]
V. D. Blondel, J.-L. Guillaume, R. Lambiotte, E. Lefebvre, Fast unfold- ing of communities in large networks, Journal of statistical mechanics: theory and experiment 2008 (10) (2008) P10008
2008
-
[18]
Girvan, M
M. Girvan, M. E. Newman, Community structure in social and biologi- cal networks, Proceedings of the National Academy of Sciences 99 (12) (2002) 7821–7826
2002
-
[19]
M. E. Newman, M. Girvan, Finding and evaluating community structure in networks, Physical Review E 69 (2) (2004) 026113
2004
-
[20]
P. Pons, M. Latapy, Computing communities in large networks using random walks, Journal of Graph Algorithms and Applications 10 (2) (2006) 191–218
2006
-
[21]
M. E. Newman, Finding community structure in networks using the eigenvectors of matrices, Physical Review E 74 (3) (2006) 036104
2006
-
[22]
S. S. Meena, P. C. Sharma, Y. P. Singh, M. P. Singh, Graph embedding based label propagation for community detection in social networks, Scientific Reports 15 (1) (2025) 41817. 34
2025
-
[23]
R. C. Wang, Z. Wang, Precision medicine: disease subtyping and tai- lored treatment, Cancers 15 (15) (2023) 3837
2023
-
[24]
Lambert, A.-L
J. Lambert, A.-L. Leutenegger, A.-S. Jannot, A. Baudot, Tracking clus- ters of patients over time enables extracting information from medico- administrative databases, Journal of Biomedical Informatics 139 (2023) 104309
2023
-
[25]
Greene, D
D. Greene, D. Doyle, P. Cunningham, Tracking the evolution of com- munities in dynamic social networks, in: 2010 international conference on advances in social networks analysis and mining, IEEE, 2010, pp. 176–183
2010
-
[26]
Irani, N
J. Irani, N. Pise, M. Phatak, Clustering techniques and the similarity measures used in clustering: A survey, International Journal of Com- puter Applications 134 (7) (2016) 9–14
2016
-
[27]
Hanin, J
A. Hanin, J. Cespedes, Y. Pulluru, M. Gopaul, E. Aronica, D. De- campo, I. Helbig, C. L. Howe, A. Huttner, S. Koh, et al., Review and standard operating procedures for collection of biospecimens and anal- ysis of biomarkers in new onset refractory status epilepticus, Epilepsia 64 (6) (2023) 1444–1457
2023
-
[28]
D. J. Polley, P. Latham, M. Y. Choi, K. A. Buhler, M. J. Fritzler, M. L. Fritzler, Identification of novel clusters of co-expressing cytokines in a diagnostic cytokine multiplex test, Frontiers in Immunology 14 (2023) 1223817. 35
2023
-
[29]
Kothur, S
K. Kothur, S. Bandodkar, L. Wienholt, S. Chu, A. Pope, D. Gill, R. C. Dale, Etiology is the key determinant of neuroinflammation in epilepsy: elevation of cerebrospinal fluid cytokines and chemokines in febrile infection-related epilepsy syndrome and febrile status epilepti- cus, Epilepsia 60 (8) (2019) 1678–1688
2019
-
[30]
Fang, et al., Circulating cytokine profiling and clustering identify biomarker predicting efficacy of ici in combination with chemotherapy, Cancer Letters 631 (2025) 217918
X.Xu, Y.Li, S.Sun, X.Lin, W.Zhang, Y.Wu, B.Wei, D.Xu, C.Zheng, H. Fang, et al., Circulating cytokine profiling and clustering identify biomarker predicting efficacy of ici in combination with chemotherapy, Cancer Letters 631 (2025) 217918. 36 Appendix A. Supplementary Methods The CN model To attribute clusters to a newly added patient to graph eG=G∪(V N+1...
2025
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.