MetaboNet: The Largest Publicly Available Consolidated Dataset for Type 1 Diabetes Management
Pith reviewed 2026-05-16 13:17 UTC · model grok-4.3
The pith
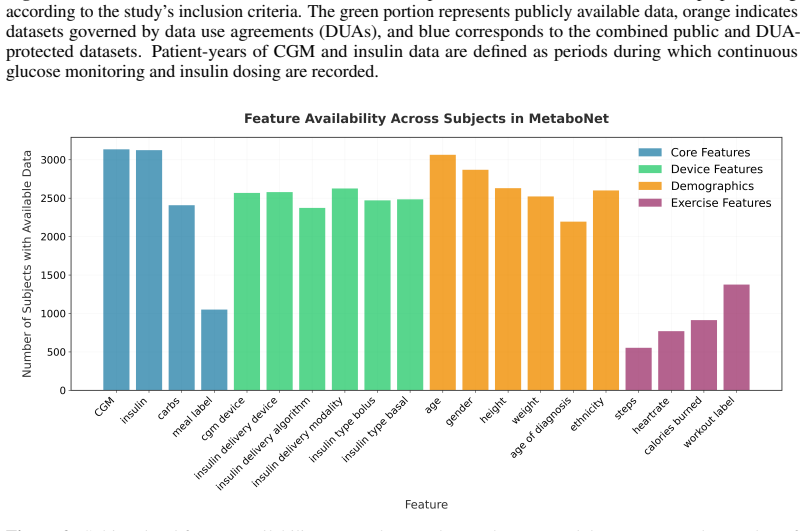
MetaboNet consolidates multiple type 1 diabetes datasets into one resource with 3135 subjects and 1228 patient-years of CGM and insulin data.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
By consolidating multiple publicly available T1D datasets that contain overlapping CGM and insulin pump dosing records into a unified format, the resulting MetaboNet dataset reaches a scale of 3135 subjects and 1228 patient-years while preserving auxiliary information such as carbohydrate intake and physical activity, with access provided through both direct public download and standardized pipelines for restricted components.
What carries the argument
The MetaboNet dataset formed by consolidating T1D datasets that supply both CGM and insulin records into one standardized structure.
If this is right
- Algorithms can be developed and tested on a larger and more demographically varied patient population than any single prior dataset allows.
- Standardized formatting removes the repeated preprocessing work that previously hindered cross-dataset comparisons.
- Broad coverage of glycemic profiles supports claims of improved generalizability for new management tools.
- Public availability of the main subset enables faster iteration by any researcher without application delays.
- Processing pipelines for restricted data maintain inclusion while satisfying original data-use requirements.
Where Pith is reading between the lines
- Closed-loop insulin delivery systems could be trained and validated against this common large-scale resource before clinical trials.
- Future observational studies may adopt the same data schema to allow automatic merging with MetaboNet.
- Statistical power for detecting rare events such as nocturnal hypoglycemia increases with the combined patient-years.
- Benchmarking platforms for machine-learning glucose predictors can now use a single reference dataset instead of multiple incompatible ones.
Load-bearing premise
Data collected under different protocols and devices can be merged into a single format without introducing meaningful biases or losing clinically important details.
What would settle it
An experiment showing that predictive models trained on the consolidated MetaboNet data produce measurably worse glycemic control outcomes than models trained on the original unmerged datasets.
Figures




read the original abstract
Progress in Type 1 Diabetes (T1D) algorithm development is limited by the fragmentation and lack of standardization across existing T1D management datasets. Current datasets differ substantially in structure and are time-consuming to access and process, which impedes data integration and reduces the comparability and generalizability of algorithmic developments. This work aims to establish a unified and accessible data resource for T1D algorithm development. Multiple publicly available T1D datasets were consolidated into a unified resource, termed the MetaboNet dataset. Inclusion required the availability of both continuous glucose monitoring (CGM) data and corresponding insulin pump dosing records. Additionally, auxiliary information such as reported carbohydrate intake and physical activity was retained when present. The MetaboNet dataset comprises 3135 subjects and 1228 patient-years of overlapping CGM and insulin data, making it substantially larger than existing standalone benchmark datasets. The resource is distributed as a fully public subset available for immediate download at https://metabo-net.org/ , and with a Data Use Agreement (DUA)-restricted subset accessible through their respective application processes. For the datasets in the latter subset, processing pipelines are provided to automatically convert the data into the standardized MetaboNet format. A consolidated public dataset for T1D research is presented, and the access pathways for both its unrestricted and DUA-governed components are described. The resulting dataset covers a broad range of glycemic profiles and demographics and thus can yield more generalizable algorithmic performance than individual datasets.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript presents MetaboNet, a consolidated dataset formed by aggregating multiple publicly available Type 1 Diabetes (T1D) management sources that contain overlapping continuous glucose monitoring (CGM) and insulin pump dosing records. Inclusion requires both CGM and insulin data, with auxiliary fields (carbohydrate intake, activity) retained when available. The resulting resource comprises 3135 subjects and 1228 patient-years, distributed as a fully public subset plus DUA-restricted components with provided conversion pipelines to a unified format. The central claim is that this unified, substantially larger dataset will support more generalizable T1D algorithm development than existing standalone benchmarks.
Significance. If the consolidation preserves data integrity across heterogeneous sources, the dataset would constitute a valuable, large-scale public resource for T1D research, exceeding the scale of current benchmarks and enabling broader algorithmic validation. The explicit access pathways and processing pipelines add immediate practical utility for the community.
major comments (2)
- [Abstract] Abstract: The headline size metrics (3135 subjects, 1228 patient-years) rest on successful unification, yet no quantitative validation is supplied for the consolidation pipeline, such as alignment success rates, handling of mismatched CGM sampling intervals (5-min vs 15-min), insulin unit standardization, or the fraction of records dropped due to missing overlap. This directly affects the claim that the dataset yields improved generalizability.
- [Abstract] Abstract and processing description: No post-consolidation metrics or bias checks (e.g., comparison of glycemic distributions or temporal correlations before/after unification) are reported, leaving open the possibility that protocol differences systematically alter the data and undermine the asserted advantage over standalone datasets.
minor comments (2)
- [Abstract] The manuscript should explicitly list the source datasets consolidated and their individual sizes to allow readers to assess the contribution of each.
- [Abstract] Verify that the provided download link (https://metabo-net.org/) remains functional and that the public subset description matches the final release.
Simulated Author's Rebuttal
We thank the referee for the constructive feedback and the recommendation of minor revision. We agree that additional quantitative details on the consolidation pipeline will strengthen the manuscript and will incorporate them in the revised version.
read point-by-point responses
-
Referee: [Abstract] Abstract: The headline size metrics (3135 subjects, 1228 patient-years) rest on successful unification, yet no quantitative validation is supplied for the consolidation pipeline, such as alignment success rates, handling of mismatched CGM sampling intervals (5-min vs 15-min), insulin unit standardization, or the fraction of records dropped due to missing overlap. This directly affects the claim that the dataset yields improved generalizability.
Authors: We agree that explicit quantitative validation of the unification steps is needed to support the reported scale and generalizability claims. In the revised manuscript we will add a new subsection to the Methods that reports alignment success rates across source datasets, the resampling procedure used to standardize CGM intervals to 5 minutes, the mapping applied for insulin unit standardization, and the exact fraction of records excluded because of insufficient temporal overlap between CGM and insulin streams. These metrics will be presented both in aggregate and broken down by source to allow readers to assess the robustness of the consolidation. revision: yes
-
Referee: [Abstract] Abstract and processing description: No post-consolidation metrics or bias checks (e.g., comparison of glycemic distributions or temporal correlations before/after unification) are reported, leaving open the possibility that protocol differences systematically alter the data and undermine the asserted advantage over standalone datasets.
Authors: We acknowledge that post-consolidation bias diagnostics would further substantiate that the unified dataset preserves the statistical properties of the original sources. In the revision we will include a new Results subsection that compares key glycemic statistics (mean glucose, time-in-range, coefficient of variation) and selected temporal correlation measures before and after unification, stratified by source. Any observed shifts will be discussed with respect to known protocol differences, thereby addressing the concern that systematic alterations may have occurred. revision: yes
Circularity Check
No circularity: descriptive aggregation of existing datasets only
full rationale
The paper performs no derivations, predictions, or parameter fitting. It aggregates publicly available T1D datasets into a unified format, reports the resulting subject count and patient-years as direct sums after processing, and provides access pipelines. No equations, self-citations as load-bearing premises, uniqueness theorems, or ansatzes appear. The size figures are empirical tallies from source data, not outputs that reduce to the paper's own inputs by construction. The work is self-contained against external benchmarks.
Axiom & Free-Parameter Ledger
axioms (1)
- domain assumption Data from different sources can be standardized without loss of critical information
Forward citations
Cited by 1 Pith paper
-
A unified data format for managing diabetes time-series data: DIAbetes eXchange (DIAX)
DIAX is a standardized JSON format that unifies diabetes time-series data including CGM, insulin, and meal signals to enable better interoperability and reproducibility across datasets.
Reference graph
Works this paper leans on
-
[1]
E. M. Aiello, S. Deshpande, B. Ozaslan, et al. “Review of Automated Insulin Delivery Systems for Individuals with Type 1 Diabetes: Tailored Solutions for Subpopulations”. In:Current Opinion in Biomedical Engineering19 (2021), p. 100312.DOI: 10.1016/j.cobme.2021. 100312
-
[2]
E. M. Aiello, M. Jaloli, and M. Cescon. “Model Predictive Control (MPC) of an artificial pancreas with data-driven learning of multi-step-ahead blood glucose predictors”. In:Control Engineering Practice144 (2024), p. 105810.DOI: 10.1016/j.conengprac.2023.105810
-
[3]
E. M. Aiello, C. Toffanin, M. C. Riddell, et al. “A hierarchical network model for the estimate of the energy expenditure in individuals with type 1 diabetes”. In:Engineering Applications of Artificial Intelligence159 (2025), p. 111758.DOI:10.1016/j.engappai.2025.111758
-
[4]
A Longitudinal Multimodal Dataset of Type 1 Diabetes
A. Alsuhaymi, A. Bilal, D. G. García, et al. “A Longitudinal Multimodal Dataset of Type 1 Diabetes”. In:Scientific Data12.1 (2025), p. 1379.DOI:10.1038/s41597-025-05695-1
-
[5]
Tadej Battelino, Thomas Danne, Richard M. Bergenstal, et al. “Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range”. In:Diabetes Care42.8 (2019), pp. 1593–1603.DOI: 10.2337/dci19- 0028
-
[6]
R. W. Beck, D. Raghinaru, P. Calhoun, et al. “A Comparison of Continuous Glucose Monitoring-Measured Time-in-Range 70-180 mg/dL Versus Time-in-Tight-Range 70-140 mg/dL”. In:Diabetes Technology & Therapeutics26.3 (2024), pp. 151–155.DOI: 10.1089/ dia.2023.0380. 20 APREPRINT- JANUARY19, 2026
-
[7]
Giulia Cappon, Francesco Prendin, Andrea Facchinetti, et al. “Individualized Models for Glucose Prediction in Type 1 Diabetes: Comparing Black-Box Approaches to a Physiological White-Box One”. In:IEEE Transactions on Biomedical Engineering70.11 (2023), pp. 3105– 3115.DOI:10.1109/TBME.2023.3276193
-
[8]
Event-Triggered Model Predictive Control For Embedded Artificial Pancreas Systems
Ankush Chakrabarty, Styliani Zavitsanou, Francis J. Doyle, et al. “Event-Triggered Model Predictive Control For Embedded Artificial Pancreas Systems”. In:IEEE Transactions on Biomedical Engineering65.3 (2018), pp. 575–586.DOI:10.1109/TBME.2017.2707344
-
[9]
Ten years after ImageNet: a 360° perspective on artificial intelligence
S. Chawla, P. Nakov, A. Ali, et al. “Ten years after ImageNet: a 360° perspective on artificial intelligence”. In:Royal Society Open Science10.3 (2023), p. 221414.DOI: 10.1098/rsos. 221414
-
[10]
S. Cho, E. M. Aiello, B. Ozaslan, et al. “Design of a Real-Time Physical Activity Detection and Classification Framework for Individuals With Type 1 Diabetes”. In:Journal of Diabetes Science and Technology18.5 (2024), pp. 1146–1156.DOI:10.1177/19322968231153896
-
[11]
Evaluating clinical accuracy of systems for self-monitoring of blood glucose
W. L. Clarke, D. Cox, L. A. Gonder-Frederick, et al. “Evaluating clinical accuracy of systems for self-monitoring of blood glucose”. In:Diabetes Care10.5 (1987), pp. 622–628.DOI: 10.2337/diacare.10.5.622
-
[12]
D. Cooper, B. Reinhold, A. Shahid, et al. “Glucose Variability Analysis in Two Large- Scale and Real-World Data Sets of Open-Source Automated Insulin Delivery Systems”. In:Journal of Diabetes Science and Technology19.3 (2025), pp. 649–657.DOI: 10.1177/ 19322968231198871
work page 2025
-
[13]
Availability of Open Dynamic Glycemic Data in the Field of Diabetes Research: A Scoping Review
L. L. Del Giudice, A. Piersanti, C. Göbl, et al. “Availability of Open Dynamic Glycemic Data in the Field of Diabetes Research: A Scoping Review”. In:Journal of Diabetes Science and Technology(2025), p. 19322968251316896.DOI:10.1177/19322968251316896
-
[14]
J. Deng, W. Dong, R. Socher, et al. “ImageNet: A Large-Scale Hierarchical Image Database”. In:Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition (CVPR). 2009.DOI:10.1109/CVPR.2009.5206848
-
[15]
M. Dhaliwal, K. Tang, E. M. Aiello, et al. “Variation in Hypoglycemia Risk During Real-World Physical Activity in Adults with Type 1 Diabetes: Insights from the Type 1 Diabetes Exercise Initiative”. In:Diabetes Technology & Therapeutics(2025), p. 15209156251400209.DOI: 10.1177/15209156251400209
-
[16]
T. C. Dunn, R. A. Ajjan, R. M. Bergenstal, et al. “Is It Time to Move Beyond TIR to TITR? Real-World Data from Over 20,000 Users of Continuous Glucose Monitoring in Patients with Type 1 and Type 2 Diabetes”. In:Diabetes Technology & Therapeutics26.3 (2024), pp. 203–210.DOI:10.1089/dia.2023.0565
-
[17]
Offline reinforcement learning for safer blood glucose control in people with type 1 diabetes
H. Emerson, M. Guy, and R. McConville. “Offline reinforcement learning for safer blood glucose control in people with type 1 diabetes”. In:Journal of Biomedical Informatics142 (2023), p. 104376.DOI:10.1016/j.jbi.2023.104376
-
[18]
RSSDI consensus recommendations on insulin therapy in the management of diabetes
Expert panel (extended), R. Chawla, B. M. Makkar, et al. “RSSDI consensus recommendations on insulin therapy in the management of diabetes”. In:International Journal of Diabetes in Developing Countries39.S2 (2019), pp. 43–92.DOI:10.1007/s13410-019-00783-6
-
[19]
J. Fu, M. Norouzi, O. Nachum, et al.Benchmarks for Deep Off-Policy Evaluation. 2021.DOI: 10.48550/arXiv.2103.16596. arXiv:2103.16596
-
[20]
H. Hameed and S. Kleinberg. “Comparing Machine Learning Techniques for Blood Glucose Forecasting Using Free-living and Patient Generated Data”. In:Proceedings of Machine Learning Research. V ol. 126. 2020, pp. 871–894
work page 2020
-
[21]
Trevor Hastie, Robert Tibshirani, and Jerome Friedman.The Elements of Statistical Learning. Springer Series in Statistics. New York, NY: Springer, 2009.DOI: 10.1007/978-0-387- 84858-7
-
[22]
jaeb.org/datasets/diabetes(visited on 10/26/2025)
JAEB Center for Health Research.Diabetes Datasets and Documents.URL: https://public. jaeb.org/datasets/diabetes(visited on 10/26/2025)
work page 2025
-
[23]
Control-Relevant Models for Glucose Control Using A Priori Patient Characteristics
K. van Heusden, E. Dassau, H. C. Zisser, et al. “Control-Relevant Models for Glucose Control Using A Priori Patient Characteristics”. In:IEEE Transactions on Biomedical Engineering 59.7 (2012), pp. 1839–1849.DOI:10.1109/TBME.2011.2176939
-
[24]
J. I. Hidalgo, J. Alvarado, M. Botella, et al. “HUPA-UCM diabetes dataset”. In:Data in Brief 55 (2024), p. 110559.DOI:10.1016/j.dib.2024.110559. 21 APREPRINT- JANUARY19, 2026
-
[25]
Peter G. Jacobs, Pau Herrero, Andrea Facchinetti, et al. “Artificial intelligence and machine learning for improving glycemic control in diabetes: best practices, pitfalls and opportunities”. In:IEEE Reviews in Biomedical Engineering(2023). Early Access.DOI: 10.1109/RBME. 2023.3331297
-
[26]
JAEB Center for Health Research.A Multi-Center Study of the Control-IQ Closed Loop Control System in Children with Type 1 Diabetes (DCLP5). n.d.URL: https://public. jaeb.org/dataset/535(visited on 01/12/2026)
work page 2026
-
[27]
n.d.URL:https://public.jaeb.org/dataset/546(visited on 01/12/2026)
JAEB Center for Health Research.A Randomized Trial Comparing Continuous Glucose Monitoring With and Without Routine Blood Glucose Monitoring in Adults with Type 1 Diabetes. n.d.URL:https://public.jaeb.org/dataset/546(visited on 01/12/2026)
work page 2026
-
[28]
JAEB Center for Health Research.An Observational Study of Individuals with Type 1 Diabetes Using the Loop System for Automated Insulin Delivery. n.d.URL: https://public.jaeb. org/dataset/560(visited on 01/12/2026)
work page 2026
-
[29]
PID + Fuzzy Logic) in Individuals with Type 1 Diabetes
JAEB Center for Health Research.FLAIR — Fuzzy Logic Automated Insulin Regulation: A Crossover Study Comparing Two Automated Insulin Delivery System Algorithms (PID vs. PID + Fuzzy Logic) in Individuals with Type 1 Diabetes. n.d.URL: https://public.jaeb.org/ dataset/566(visited on 01/12/2026)
work page 2026
-
[30]
n.d.URL: https://public.jaeb.org/ dataset/581(visited on 01/12/2026)
JAEB Center for Health Research.Pilot Study 3 of Outpatient Control-to-Range: Safety and Efficacy with Day-and-Night In-Home Use (CTR3). n.d.URL: https://public.jaeb.org/ dataset/581(visited on 01/12/2026)
work page 2026
-
[31]
n.d.URL: https://public.jaeb.org/ dataset/579(visited on 01/12/2026)
JAEB Center for Health Research.The Insulin-Only Bionic Pancreas Pivotal Trial: Testing the iLet in Adults and Children with Type 1 Diabetes. n.d.URL: https://public.jaeb.org/ dataset/579(visited on 01/12/2026)
work page 2026
-
[32]
n.d.URL: https://public.jaeb.org/dataset/573 (visited on 01/12/2026)
JAEB Center for Health Research.The International Diabetes Closed Loop (iDCL) Trial: Clinical Acceptance of the Artificial Pancreas - A Pivotal Study of t:Slim X2 with Control-IQ Technology (DCLP3). n.d.URL: https://public.jaeb.org/dataset/573 (visited on 01/12/2026)
work page 2026
-
[33]
JAEB Center for Health Research.The Pediatric Artificial Pancreas (PEDAP) Trial of Control- IQ Technology in Young Children in Type 1 Diabetes. n.d.URL: https://public.jaeb. org/dataset/599(visited on 01/12/2026)
work page 2026
-
[34]
Sam Gordon James.BrisT1D-Open Dataset. 2025.DOI: 10 . 5523 / bris . 33z5jc8fa6tob21ptrugzqog08
work page 2025
-
[35]
S. Khamesian, A. Arefeen, B. M. Thompson, et al.AZT1D: A Real-World Dataset for Type 1 Diabetes. Version 1. 2025.DOI:10.17632/gk9m674wcx.1
-
[36]
B. P. Kovatchev, A. C. Frasquet, E. C. Pryor, et al. “Neural-Net Artificial Pancreas: A Random- ized Crossover Trial of a First-in-Class Automated Insulin Delivery Algorithm”. In:Diabetes Technology & Therapeutics(2024).DOI:10.1089/dia.2023.0469
-
[37]
L. M. Laffel, J. L. Sherr, J. Liu, et al. “Limitations in Achieving Glycemic Targets From CGM Data and Persistence of Severe Hypoglycemia in Adults With Type 1 Diabetes Regardless of Insulin Delivery Method”. In:Diabetes Care48.2 (2025), pp. 273–278.DOI: 10.2337/dc24- 1474
-
[38]
Offline Reinforcement Learning: Tutorial, Review, and Perspectives on Open Problems
S. Levine, A. Kumar, G. Tucker, et al.Offline Reinforcement Learning: Tutorial, Review, and Perspectives on Open Problems. 2020.DOI: 10.48550/arXiv.2005.01643 . arXiv: 2005.01643
work page internal anchor Pith review Pith/arXiv arXiv doi:10.48550/arxiv.2005.01643 2020
-
[39]
GluNet: A Deep Learning Framework for Accurate Glucose Forecasting
K. Li, C. Liu, T. Zhu, et al. “GluNet: A Deep Learning Framework for Accurate Glucose Forecasting”. In:IEEE Journal of Biomedical and Health Informatics24.2 (2020), pp. 414– 423.DOI:10.1109/JBHI.2019.2931842
-
[40]
Artificial intelligence for diabetes management – a review
S. Maheshwari, A. Kalia, J. Tewari, et al. “Artificial intelligence for diabetes management – a review”. In:JDMDC12.1 (2025), pp. 24–32.DOI:10.15406/jdmdc.2025.12.00292
-
[41]
The OhioT1DM Dataset for Blood Glucose Level Prediction: Update 2020
C. Marling and R. Bunescu. “The OhioT1DM Dataset for Blood Glucose Level Prediction: Update 2020”. In:CEUR Workshop Proceedings. V ol. 2675. 2020, pp. 71–74
work page 2020
-
[42]
A. Neinstein, J. Wong, H. Look, et al. “A case study in open source innovation: developing the Tidepool Platform for interoperability in type 1 diabetes management”. In:Journal of the American Medical Informatics Association23.2 (2016), pp. 324–332.DOI: 10.1093/jamia/ ocv104. 22 APREPRINT- JANUARY19, 2026
-
[43]
Nudge BG.Babelbetes.URL: https://nudgebg.github.io/babelbetes/ (visited on 10/26/2025)
work page 2025
-
[44]
C. Piona, E. M. Aiello, V . Mancioppi, et al. “An Exploratory Analysis of Continuous Glu- cose Monitoring Metrics in Relation to Prediabetes in Youths with Obesity”. In:Diabetes Technology & Therapeutics(2025).DOI:10.1177/15209156251407959
-
[45]
T. Prioleau, A. Bartolome, R. Comi, et al. “DiaTrend: A dataset from advanced diabetes technology to enable development of novel analytic solutions”. In:Scientific Data10.1 (2023), p. 556.DOI:10.1038/s41597-023-02469-5
-
[46]
Replica Health.MetaboNet. Accessed 2025-11-07. n.d.URL: https://metabo-net.org/ data-dictionary
work page 2025
-
[47]
Replica Health.MetaboNet Processor. Accessed 2025-10-26. n.d.URL: https://github. com/replicahealth/metabonet_processor
work page 2025
-
[48]
M. C. Riddell, Z. Li, R. L. Gal, et al. “Examining the Acute Glycemic Effects of Different Types of Structured Exercise Sessions in Type 1 Diabetes in a Real-World Setting: The Type 1 Diabetes and Exercise Initiative (T1DEXI)”. In:Diabetes Care46.4 (2023), p. 704.DOI: 10.2337/dc22-1721
-
[49]
A. Shahid and D. M. Lewis. “Large-Scale Data Analysis for Glucose Variability Outcomes with Open-Source Automated Insulin Delivery Systems”. In:Nutrients14.9 (2022), p. 1906. DOI:10.3390/nu14091906
-
[50]
Hypoglycemia Early Alarm Systems Based On Multivariable Models
K. Turksoy, E. S. Bayrak, L. Quinn, et al. “Hypoglycemia Early Alarm Systems Based On Multivariable Models”. In:Industrial & Engineering Chemistry Research52.35 (2013), pp. 12329–12336.DOI:10.1021/ie3034015
-
[51]
Hierarchical Amortized GAN for 3D High Resolution Medical Image Synthesis,
K. Turksoy, S. Samadi, J. Feng, et al. “Meal Detection in Patients With Type 1 Diabetes: A New Module for the Multivariable Adaptive Artificial Pancreas Control System”. In:IEEE Journal of Biomedical and Health Informatics20.1 (2016), pp. 47–54.DOI: 10.1109/JBHI. 2015.2446413
-
[52]
A perspective on harmonizing diabetes management datasets
M. K. Wolff, S. Royston, A. L. Fougner, et al. “A perspective on harmonizing diabetes management datasets”. In:Data in Brief59 (2025), p. 111399.DOI: 10.1016/j.dib.2025. 111399
-
[53]
GluPredKit: A Python Package for Blood Glucose Prediction and Evaluation
M. K. Wolff, S. Royston, and R. V olden. “GluPredKit: A Python Package for Blood Glucose Prediction and Evaluation”. In:Journal of Open Source Software9.101 (2024), p. 6904.DOI: 10.21105/joss.06904
-
[54]
Blood Glucose Prediction Algorithms Require Clinically Relevant Performance Criteria Beyond Accuracy
M. K. Wolff, H. G. Schaathun, S. Gros, et al. “Blood Glucose Prediction Algorithms Require Clinically Relevant Performance Criteria Beyond Accuracy”. In:Diabetes Technology & Therapeutics27.10 (2025), pp. 858–870.DOI:10.1089/dia.2025.0074
-
[55]
J. Xie and Q. Wang. “Benchmarking Machine Learning Algorithms on Blood Glucose Pre- diction for Type I Diabetes in Comparison With Classical Time-Series Models”. In:IEEE Transactions on Biomedical Engineering67.11 (2020), pp. 3101–3124.DOI: 10.1109/TBME. 2020.2975959
-
[56]
Chinese diabetes datasets for data-driven machine learning
Q. Zhao, J. Zhu, X. Shen, et al. “Chinese diabetes datasets for data-driven machine learning”. In:Scientific Data10.1 (2023), p. 35.DOI:10.1038/s41597-023-01940-7
-
[57]
T. Zhu, K. Li, and P. Georgiou. “Offline Deep Reinforcement Learning and Off-Policy Evalua- tion for Personalized Basal Insulin Control in Type 1 Diabetes”. In:IEEE Journal of Biomedical and Health Informatics27.10 (2023), pp. 5087–5098.DOI:10.1109/JBHI.2023.3303367. 23
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.