From Full and Partial Intraoral Scans to Crown Proposal: A Classification-Guided Restoration Assistance Pipeline
Pith reviewed 2026-05-19 16:10 UTC · model grok-4.3
The pith
A classification-guided pipeline produces patient-specific crown proposals from partial intraoral scans in 2.5-3.5 minutes.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
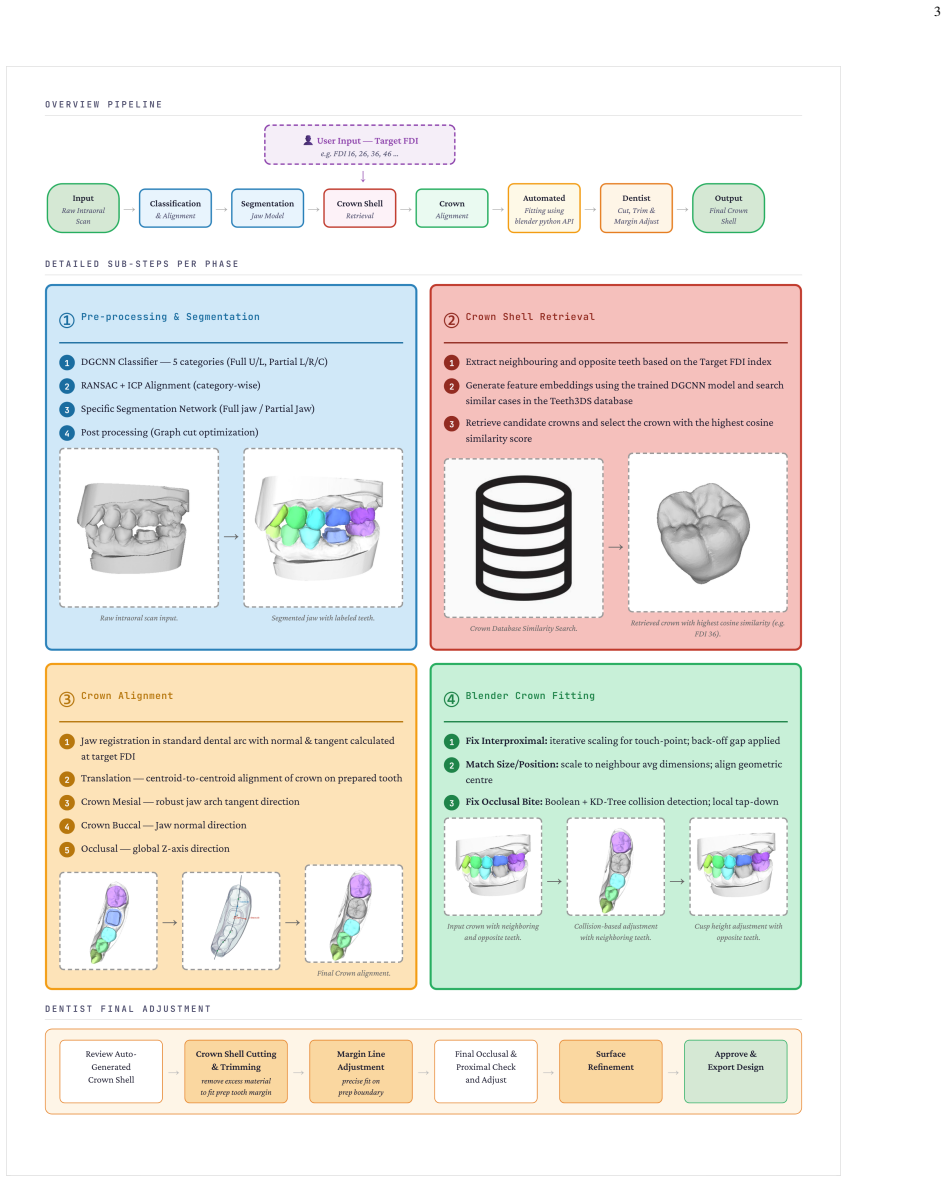
The pipeline takes a raw intraoral scan and FDI tooth number as input and outputs an initial crown proposal. By routing segmentation through a classify-then-align strategy for partial scans and using DGCNN-based retrieval over neighboring teeth embeddings, it achieves macro-average DSC 0.9249 across 17 classes on 1,958 partial scans and generates the crown shell in 2.5-3.5 minutes.
What carries the argument
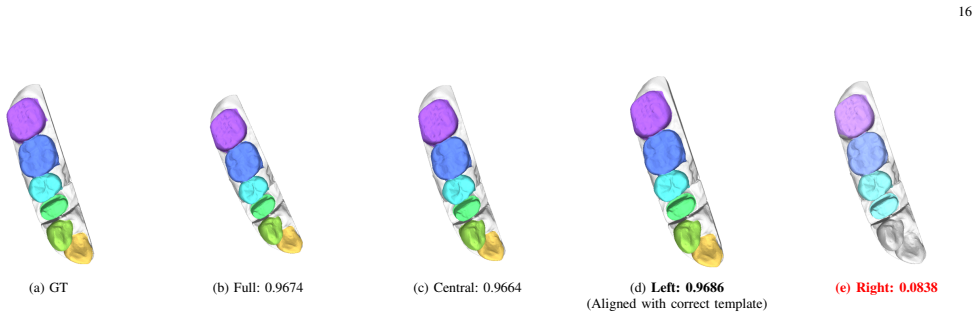
The classify-then-align segmentation strategy that first categorizes the scan into one of five anatomical types with DGCNN, applies coarse-to-fine RANSAC+ICP registration, and refines boundaries with graph-cut, followed by the context-aware retrieval using cosine similarity on DGCNN embeddings of neighboring and opposing teeth.
If this is right
- Partial scans achieve macro-average DSC 0.9249 with sub-millimeter centroid errors of 0.2666-0.2774 mm for the prepared tooth and neighbors.
- The pipeline supplies a fast, practical alternative to generative approaches that lose occlusal detail.
- High segmentation precision and recall support reliable downstream crown fitting in CAD/CAM workflows.
- The method works on the partial scans preferred for single-unit cases to avoid stitching errors.
Where Pith is reading between the lines
- The embedding-retrieval approach could extend to other single-tooth restorations such as inlays or onlays.
- Adding a lightweight generative step after retrieval might further refine occlusal surfaces while retaining speed.
- Expanding the candidate library or testing on underrepresented anatomies would clarify limits of the similarity-based selection.
Load-bearing premise
Cosine similarity over DGCNN embeddings of neighboring and opposing teeth will surface geometrically suitable crown candidates that match the specific patient anatomy.
What would settle it
A test set of partial scans where retrieved crowns repeatedly fail to match occlusal contacts or proximal surfaces accurately, forcing extensive manual edits, would show the retrieval step does not deliver clinically usable proposals.
Figures












read the original abstract
Single-unit crown restoration is among the most common procedures in clinical dentistry, with CAD/CAM workflows now designing crowns directly from intraoral scans. Partial scans are often preferred over full-arch scans for single-unit cases due to fewer stitching errors, yet most segmentation networks trained on full arches fail on partial scans, while end-to-end generative crown methods often produce over-smoothed surfaces that lose occlusal detail. We propose an end-to-end pipeline that takes a raw intraoral scan and target FDI tooth number as input and outputs an initial, patient-specific crown proposal for clinician refinement. The pipeline has three phases: (I) data preparation and pose standardization; (II) segmentation routed by scan type; and (III) crown proposal generation via context-aware retrieval and Blender-based fitting. We address partial-scan segmentation through a classify-then-align strategy: a DGCNN classifier categorizes the scan into one of five anatomical types, then coarse-to-fine RANSAC+ICP registration standardizes the jaw coordinate frame, followed by graph-cut optimization to refine tooth-gingival boundaries. Trained on 1,958 partial scans, the pipeline achieves macro-average DSC 0.9249, Recall 0.8919, and Precision 0.9615 across 17 semantic classes; a fine-tuned full-arch model reaches DSC 0.9347. The prepared tooth and its mesial and distal neighbors achieve DSC 0.9468-0.9569 with sub-millimeter Centroid Errors (0.2666-0.2774 mm). These centroids anchor a retrieval module using DGCNN embeddings and cosine similarity over neighboring and opposing teeth, followed by spline-guided alignment and Blender Python API refinement. The pipeline produces a preliminary crown shell in 2.5-3.5 minutes, offering a practical alternative to end-to-end generative approaches.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript proposes an end-to-end pipeline that accepts a raw intraoral scan and target FDI tooth number and outputs a preliminary patient-specific crown shell. Phase I standardizes pose; Phase II classifies the scan into one of five anatomical types with DGCNN, applies coarse-to-fine RANSAC+ICP registration, and refines tooth-gingival boundaries via graph-cut; Phase III retrieves library crowns via cosine similarity on DGCNN embeddings of neighboring and opposing teeth, then performs spline-guided alignment and Blender Python API fitting. On 1,958 partial scans the segmentation stage reports macro-average DSC 0.9249, recall 0.8919, precision 0.9615 across 17 classes, with prepared-tooth and neighbor DSC 0.9468-0.9569 and centroid errors 0.2666-0.2774 mm; total runtime is stated as 2.5-3.5 minutes.
Significance. The segmentation results on partial scans are quantitatively grounded and address a documented clinical pain point where full-arch models degrade. The classify-then-align strategy and reported sub-millimeter centroid accuracy constitute a concrete, reproducible contribution. If the retrieval step can be shown to select anatomically suitable crowns, the pipeline would supply a practical, controllable alternative to end-to-end generative crown methods; the absence of any surface-distance, occlusion, or expert-comparison metrics for the final proposals, however, prevents a full assessment of clinical utility.
major comments (2)
- [Abstract / crown proposal generation] Abstract and crown-proposal section: no quantitative evaluation (surface-to-surface distance, Hausdorff distance, occlusion contact area, or expert rating versus ground-truth clinical crowns) is supplied for the output of the DGCNN-embedding retrieval, spline alignment, and Blender fitting steps. Because the headline claim of a “clinically usable preliminary crown shell” rests on the premise that cosine similarity over neighboring/opposing embeddings surfaces appropriate library candidates, this omission is load-bearing for the central contribution.
- [Abstract] Abstract: the claim that the pipeline offers a “practical alternative to end-to-end generative approaches” is not supported by any baseline comparison or ablation that isolates the contribution of the context-aware retrieval module versus a naïve nearest-neighbor or random selection from the library.
minor comments (2)
- The manuscript should report the size and diversity of the crown library used for retrieval and any inclusion/exclusion criteria applied to the 1,958-scan training set.
- Train/test split details, cross-validation strategy, and whether the 1,958 partial scans are patient-disjoint should be stated explicitly.
Simulated Author's Rebuttal
We thank the referee for the constructive feedback and for recognizing the quantitative grounding of the segmentation results on partial scans. We address the two major comments below regarding the crown-proposal stage. Where the comments correctly identify gaps in the current evaluation, we commit to revisions that strengthen the manuscript without overstating what has been demonstrated.
read point-by-point responses
-
Referee: [Abstract / crown proposal generation] Abstract and crown-proposal section: no quantitative evaluation (surface-to-surface distance, Hausdorff distance, occlusion contact area, or expert rating versus ground-truth clinical crowns) is supplied for the output of the DGCNN-embedding retrieval, spline alignment, and Blender fitting steps. Because the headline claim of a “clinically usable preliminary crown shell” rests on the premise that cosine similarity over neighboring/opposing embeddings surfaces appropriate library candidates, this omission is load-bearing for the central contribution.
Authors: We agree that the absence of surface-distance and occlusion metrics for the retrieved and fitted crowns limits assessment of the final output. The manuscript currently demonstrates the retrieval and fitting pipeline through the embedding similarity mechanism and qualitative examples, while providing detailed quantitative results only for the upstream segmentation. In the revised version we will add surface-to-surface distance and Hausdorff distance metrics computed against available ground-truth clinical crowns on a subset of cases. Occlusion contact area and formal expert ratings would require a separate clinical validation protocol; we will explicitly note this as a limitation and future direction rather than claim full clinical usability at present. revision: partial
-
Referee: [Abstract] Abstract: the claim that the pipeline offers a “practical alternative to end-to-end generative approaches” is not supported by any baseline comparison or ablation that isolates the contribution of the context-aware retrieval module versus a naïve nearest-neighbor or random selection from the library.
Authors: We accept that an explicit ablation would better isolate the benefit of context-aware retrieval over simpler baselines. The current text motivates the approach via the use of neighboring and opposing tooth embeddings but does not report a direct comparison. In the revision we will insert a quantitative ablation that compares the proposed cosine-similarity retrieval against both random library selection and nearest-neighbor selection in the same embedding space, using embedding similarity scores and qualitative fit assessment as proxies. This addition will support the claim more rigorously while remaining within the scope of the existing library and embedding model. revision: yes
- Formal expert clinical ratings of the crown proposals, which would require a new IRB-approved reader study outside the current dataset and experimental design.
Circularity Check
No circularity: empirical metrics on held-out scans and standard retrieval components do not reduce to inputs by construction
full rationale
The paper's central results are measured performance numbers (macro DSC 0.9249, centroid errors 0.2666-0.2774 mm) obtained by training and evaluating DGCNN and registration modules on 1,958 held-out partial scans. The crown proposal step invokes DGCNN embeddings + cosine similarity for retrieval followed by spline alignment and Blender fitting; these are methodological choices whose clinical suitability is an external assumption, not a quantity defined by the paper's own equations or prior self-citations. No self-definitional loops, fitted-input-as-prediction, or load-bearing self-citations appear in the derivation chain. The pipeline is therefore self-contained against external benchmarks.
Axiom & Free-Parameter Ledger
free parameters (1)
- Number of anatomical scan types
axioms (2)
- domain assumption DGCNN produces embeddings that capture clinically relevant tooth geometry for retrieval
- domain assumption RANSAC+ICP registration followed by graph-cut yields accurate tooth-gingival boundaries on partial scans
Lean theorems connected to this paper
-
IndisputableMonolith/Cost/FunctionalEquation.leanwashburn_uniqueness_aczel unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
context-aware crown retrieval module that uses DGCNN feature embeddings and cosine similarity search over neighboring and opposing teeth
-
IndisputableMonolith/Foundation/AbsoluteFloorClosure.leanabsolute_floor_iff_bare_distinguishability unclear?
unclearRelation between the paper passage and the cited Recognition theorem.
classify-then-align preprocessing strategy: a DGCNN classifier first categorizes the input scan into one of five anatomical types
What do these tags mean?
- matches
- The paper's claim is directly supported by a theorem in the formal canon.
- supports
- The theorem supports part of the paper's argument, but the paper may add assumptions or extra steps.
- extends
- The paper goes beyond the formal theorem; the theorem is a base layer rather than the whole result.
- uses
- The paper appears to rely on the theorem as machinery.
- contradicts
- The paper's claim conflicts with a theorem or certificate in the canon.
- unclear
- Pith found a possible connection, but the passage is too broad, indirect, or ambiguous to say the theorem truly supports the claim.
Reference graph
Works this paper leans on
-
[1]
L. Samaranayake, N. Tuygunov, F. Schwendicke, T. Osathanon, Z. Khurshid, S. A. Boymuradov, and A. Cahyanto, “The transformative role of artificial intelligence in dentistry: A comprehensive overview. Part 1: Fundamentals of AI, and its contemporary applications in dentistry,”International Dental Journal, vol. 75, no. 2, pp. 383– 396, 2025. [Online]. Avail...
work page 2025
-
[2]
Dilated dynamic graph CNN for efficient point cloud learning,
Y . Xu, X. Li, C. Wang, and S. Wen, “Dilated dynamic graph CNN for efficient point cloud learning,”IEEE Transactions on Image Processing, vol. 31, pp. 4468–4481, 2022. [Online]. Available: https://link.springer.com/article/10.1007/s10278-024-01061-6
-
[3]
A. Jana, A. Maiti, and D. N. Metaxas, “A critical analysis of the limitation of deep learning based 3D dental mesh segmentation methods in segmenting partial scans,” in2023 45th Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), 2023, accepted to IEEE EMBC 2023. [Online]. Available: https://arxiv.org/abs/2305.002...
-
[4]
A. Ender and A. Mehl, “Effect of intraoral scanner and fixed partial denture situation on the scan accuracy of multiple implants: an in vitro study,”Clinical Oral Implants Research, vol. 27, no. 10, pp. 1309–1316, 2016
work page 2016
-
[5]
Effect of scanned area and operator on the accuracy of dentate arch scans with a single implant,
J.-M. Park, “Effect of scanned area and operator on the accuracy of dentate arch scans with a single implant,”The Journal of Prosthetic Dentistry, vol. 116, no. 4, pp. 534–540, 2016
work page 2016
-
[6]
Accuracy of four intraoral scanners in oral implantology: a comparative in vitro study,
M. Imburgia, S. Logozzo, U. Hauschild, G. Veronesi, C. Mangano, and F. G. Mangano, “Accuracy of four intraoral scanners in oral implantology: a comparative in vitro study,”BMC Oral Health, vol. 17, no. 1, p. 92, 2017
work page 2017
-
[7]
F. G. Mangano, G. Veronesi, U. Hauschild, E. Mijiritsky, and C. Mangano, “Trueness and precision of 5 intraoral scanners in the impressions of single and multiple implants: a comparative in vitro study,”BMC Oral Health, vol. 19, no. 1, p. 101, 2019
work page 2019
-
[8]
MeshSNet: Deep multi-scale mesh feature learning for end-to-end tooth segmentation,
C. Lian, L. Wang, T.-H. Wu, M. Liu, F. Durran, D. Chambers, D. Wang, and D. Shen, “MeshSNet: Deep multi-scale mesh feature learning for end-to-end tooth segmentation,”IEEE Transactions on Medical Imaging, vol. 39, no. 11, pp. 3635–3645, 2020
work page 2020
-
[9]
DArch: Dental arch prior-assisted 3D tooth instance segmentation,
L. Qiu, Y . Zhang, E. Adeli, Q. Yu, K. Yan, G. Wang, X. Liu, L. Lu, D. Xu, and X. Xiang, “DArch: Dental arch prior-assisted 3D tooth instance segmentation,” inProceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition (CVPR), 2022, pp. 20 718– 20 727
work page 2022
-
[10]
Dynamic Graph CNN for Learning on Point Clouds
Y . Wang and J. M. Solomon, “Dynamic graph CNN for learning on point clouds,” inProceedings of the ACM SIGGRAPH Asia Conference. ACM, 2019. [Online]. Available: https://arxiv.org/abs/1801.07829
work page internal anchor Pith review Pith/arXiv arXiv 2019
-
[11]
PointNet++: Deep hierarchical feature learning on point sets in a metric space,
C. R. Qi, L. Yi, H. Su, and L. J. Guibas, “PointNet++: Deep hierarchical feature learning on point sets in a metric space,” inAdvances in Neural Information Processing Systems (NeurIPS), 2017
work page 2017
-
[12]
Tooth segmentation using generative adversarial networks,
J.-H. Hwang, D.-Y . Kim, and B.-S. Shin, “Tooth segmentation using generative adversarial networks,”Pattern Recognition Letters, vol. 145, pp. 39–45, 2021
work page 2021
-
[13]
TFormer: 3D tooth segmentation in mesh scans with geometry guided transformer,
H. Xiong, K. Li, K. Tan, Y . Feng, J. T. Zhou, J. Hao, and Z. Liu, “TFormer: 3D tooth segmentation in mesh scans with geometry guided transformer,”arXiv preprint arXiv:2210.16627, 2022. [Online]. Available: https://arxiv.org/abs/2210.16627
-
[14]
TeethNet: Dual-stream attention network for 3D tooth segmentation,
Z. Cui, C. Li, N. Chen, G. Wei, R. Run, X. Liu, and D. Ren, “TeethNet: Dual-stream attention network for 3D tooth segmentation,”Computers in Biology and Medicine, vol. 136, p. 104670, 2021
work page 2021
-
[15]
Robust segmentation of partial and imperfect dental arches,
A. A. Alsheghri, Y . Zhang, G. Hosseinimanesh, J. Keren, F. Cheriet, and F. Guibault, “Robust segmentation of partial and imperfect dental arches,”Applied Sciences, vol. 14, no. 23, p. 10784, 2024. [Online]. Available: https://www.mdpi.com/2076-3417/14/23/10784
work page 2024
-
[16]
CAD/CAM in dentistry — a critical review,
A. P. B. Samra, E. C. C. de Morais, R. F. Mazur, S. R. Vieira, and R. N. Rached, “CAD/CAM in dentistry — a critical review,”Revista Odonto Ciˆencia, vol. 31, no. 3, pp. 140–144, 2016
work page 2016
-
[17]
S. Yang, J. Han, S.-H. Lim, J.-Y . Yoo, S. Kim, D. Song, S. Kim, J.- M. Kim, and W.-J. Yi, “DCrownFormer: Morphology-aware point-to- mesh generation transformer for dental crown prosthesis from 3D scan data of antagonist and preparation teeth,” inMedical Image Computing and Computer Assisted Intervention – MICCAI 2024. Springer Nature Switzerland, 2024, p...
work page 2024
-
[18]
From mesh completion to AI-designed crown,
G. Hosseinimanesh, F. Ghadiri, F. Guibault, F. Cheriet, and J. Keren, “From mesh completion to AI-designed crown,”arXiv preprint arXiv:2501.04914, 2025
-
[19]
Personalized dental crown design: Point- to-mesh generation,
G. Hosseinimaneshet al., “Personalized dental crown design: Point- to-mesh generation,”Polytechnique Montr ´eal Publications, 2025. [Online]. Available: https://www.sciencedirect.com/science/article/pii/ S1361841524003645
work page 2025
-
[20]
H. Dinget al., “Morphology and fracture behavior of lithium disilicate dental crowns designed by human and knowledge-based AI,”Journal of Dentistry, vol. 122, p. 104146, 2022
work page 2022
-
[21]
IntelliDent: an AI-based online automated framework for dental crown generation,
I. Chafi, G. Hosseinimaneshet al., “IntelliDent: an AI-based online automated framework for dental crown generation,”ResearchGate Pub- lication, 2025
work page 2025
-
[22]
Automated tooth crown design with optimized shape and biomechanics properties,
S. Tianet al., “Automated tooth crown design with optimized shape and biomechanics properties,”Frontiers in Bioengineering and Biotechnol- ogy, 2023
work page 2023
-
[23]
Model adaptive tooth segmentation,
R. Chen, J. Yang, Y . Feng, J. Hao, and Z. Liu, “Model adaptive tooth segmentation,” inMedical Imaging with Deep Learning, ser. Proceedings of Machine Learning Research, I. Oguz, J. Noble, X. Li, M. Styner, C. Baumgartner, M. Rusu, T. Heinmann, D. Kontos, B. Landman, and B. Dawant, Eds., vol. 227. PMLR, 2024, pp. 775–798. [Online]. Available: https://proc...
work page 2024
-
[24]
Unsupervised pre-training improves tooth segmentation in 3-dimensional intraoral mesh scans,
X. He, H. Wang, H. Hu, J. Yang, Y . Feng, G. Wang, and Z. Liu, “Unsupervised pre-training improves tooth segmentation in 3-dimensional intraoral mesh scans,” inProceedings of The 5th International Conference on Medical Imaging with Deep Learning, ser. Proceedings of Machine Learning Research, E. Konukoglu, B. Menze, A. Venkataraman, C. Baumgartner, Q. Dou...
work page 2022
-
[25]
A fast point clouds registration algorithm for laser scanners,
G. Xu, Y . Pang, Z. Bai, Y . Wang, and Z. Lu, “A fast point clouds registration algorithm for laser scanners,”Applied Sciences, vol. 11, no. 8, p. 3426, 2021
work page 2021
-
[26]
Automated monitoring of tooth wear progression using AI on intraoral scans,
N. van Nistelrooij, E. Maier, H. Bronkhorst, L. Crins, T. Xi, B. A. C. Loomans, and S. Vinayahalingam, “Automated monitoring of tooth wear progression using AI on intraoral scans,”Journal of Dentistry, vol. 150, p. 105323, 2024. [Online]. Available: https://doi.org/10.1016/j.jdent.2024.105323
-
[27]
Teeth3DS: A benchmark for teeth segmentation and labeling from intra-oral 3D scans,
A. Ben-Hamadou, N. Neifar, A. Rekik, O. Smaoui, F. Bouzguenda, S. Pujades, E. Boyer, and E. Ladroit, “Teeth3DS: A benchmark for teeth segmentation and labeling from intra-oral 3D scans,” arXiv preprint arXiv:2210.06094, 2022. [Online]. Available: https: //arxiv.org/abs/2210.06094
-
[28]
Fast point feature histograms (FPFH) for 3D registration,
R. B. Rusu, N. Blodow, and M. Beetz, “Fast point feature histograms (FPFH) for 3D registration,” inIEEE International Conference on Robotics and Automation (ICRA), 2009, pp. 3212–3217
work page 2009
-
[29]
Object modelling by registration of multiple range images,
Y . Chen and G. Medioni, “Object modelling by registration of multiple range images,” inImage and Vision Computing, vol. 10, no. 3, 1991, pp. 145–155
work page 1991
-
[30]
Open3D: A Modern Library for 3D Data Processing
Q.-Y . Zhou, J. Park, and V . Koltun, “Open3D: A modern library for 3D data processing,”arXiv preprint arXiv:1801.09847, 2018
work page internal anchor Pith review Pith/arXiv arXiv 2018
-
[32]
Available: https://arxiv.org/abs/2603.04771
[Online]. Available: https://arxiv.org/abs/2603.04771
-
[33]
I. Sailer, G. I. Benic, V . Fehmer, C. H. F. H¨ammerle, and S. M¨uhlemann, “Randomized controlled within-subject evaluation of digital and conven- tional workflows for the fabrication of lithium disilicate single crowns. Part II: CAD-CAM versus conventional laboratory procedures,”Journal of Prosthetic Dentistry, vol. 118, no. 1, pp. 43–48, 2017
work page 2017
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.