Privacy-Preserving Federated Autoencoder for ECG Anomaly Detection on Edge Devices
Pith reviewed 2026-06-27 09:41 UTC · model grok-4.3
The pith
Federated learning with differential privacy and quantization matches centralized ECG anomaly detection performance on edge devices.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
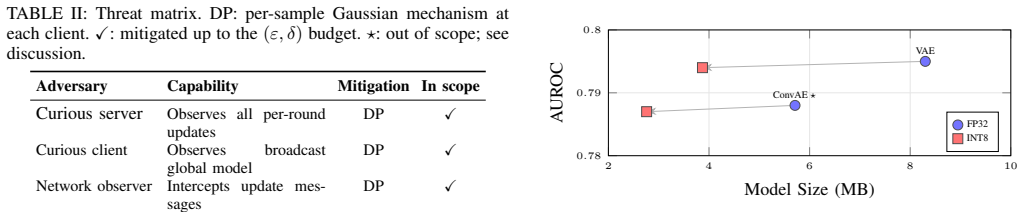
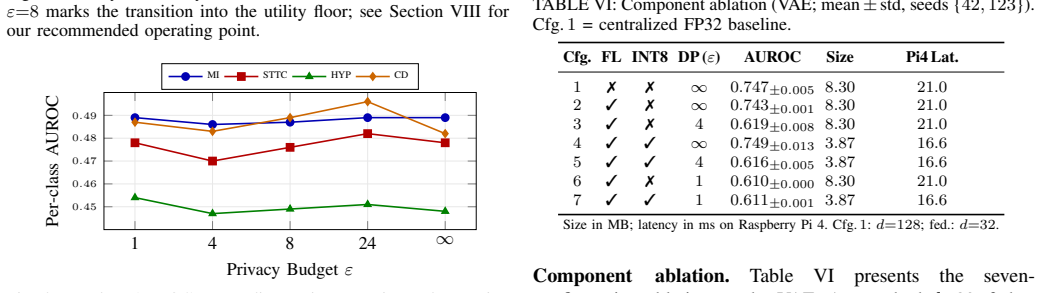
Federated learning matches or exceeds the centralized baseline across all architectures, with ConvAE federated AUROC reaching 0.782. An epsilon sweep identifies epsilon equals 4 as the recommended clinical operating point. INT8 quantization roughly halves model size and cuts Raspberry Pi 4 latency by up to 44 percent with less than 0.12 percent AUROC loss. DP and quantization penalties are empirically independent.
What carries the argument
The composition of Flower-based FedAvg across ten clients, client-side DP-SGD with a Renyi-DP accountant, and INT8 post-training quantization applied to VanillaAE, ConvAE, and VAE architectures for reconstruction-error anomaly detection on PTB-XL.
If this is right
- Strong privacy guarantees at epsilon equals 4 can be used without forcing a further reduction in model size or accuracy.
- Quantization can be applied after privacy training with additive rather than multiplicative cost.
- The same three-component pipeline can be benchmarked on other 12-lead ECG datasets to check consistency of the independence result.
- Edge deployment on AArch64 devices becomes feasible for continuous monitoring while meeting legal privacy standards.
Where Pith is reading between the lines
- The observed independence between DP noise and quantization error may generalize to other time-series sensor tasks such as EEG or blood-pressure monitoring.
- Production use would still require separate defenses against federated-specific attacks such as model poisoning that the current evaluation does not address.
- Replacing the simulated hospital partitions with actual institutional data splits would provide a stronger test of the non-IID claim.
Load-bearing premise
The ten simulated non-IID partitions of PTB-XL adequately proxy real cross-hospital data distributions and that reconstruction error serves as a reliable proxy for clinically meaningful ECG anomalies.
What would settle it
Running the same pipeline on ECG recordings collected from multiple distinct real hospitals, with anomalies labeled by cardiologists rather than derived from reconstruction error on simulated partitions.
Figures


read the original abstract
Continuous electrocardiography (ECG) monitoring could surface rhythm abnormalities before they escalate into cardiovascular events. However, a deployable system must satisfy three requirements simultaneously: legal-grade privacy (GDPR, HIPAA), real-time inference on constrained edge hardware, and detection quality under non-IID cross-hospital data. We design and evaluate an end-to-end federated system addressing all three for unsupervised 12-lead ECG anomaly detection on PTB-XL dataset, combining three autoencoder families (VanillaAE, ConvAE, VAE), Flower-based federated averaging (FedAvg) across ten simulated hospitals, client-side differentially private SGD (DP-SGD) with a R\'enyi-DP accountant, and 8-bit integer (INT8) post-training quantization with Raspberry Pi 4 benchmarking. Our main contributions are: an empirical characterization of how these mechanisms compose, practical DP-specific recommendations, and technical and security insights for a clinically sensitive setting. Federated learning matches or exceeds the centralized baseline across all architectures (ConvAE federated area under the ROC curve, AUROC, $0.782$), and an $\varepsilon$ sweep identifies $\varepsilon=4$ as the recommended clinical operating point. INT8 quantization roughly halves model size and cuts Pi 4 latency by up to $44%$ with $<0.12%$ AUROC loss. Crucially, DP and quantization penalties are empirically independent, so practitioners need not trade a strong privacy guarantee for a compact edge footprint. To our knowledge, this is the first system combining federated learning, formal $(\varepsilon,\delta)$-DP, unsupervised reconstruction-based detection, and quantized AArch64 deployment.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript describes an end-to-end federated system for unsupervised 12-lead ECG anomaly detection using autoencoders (VanillaAE, ConvAE, VAE) on the PTB-XL dataset. It integrates Flower-based FedAvg across ten simulated hospitals, client-side DP-SGD with a Rényi-DP accountant, and 8-bit post-training quantization, with Raspberry Pi 4 benchmarking. Central empirical claims are that federated ConvAE achieves AUROC 0.782 matching or exceeding the centralized baseline, DP and quantization penalties are independent, quantization halves model size with up to 44% latency reduction and <0.12% AUROC loss, and ε=4 is the recommended clinical operating point.
Significance. If the reported measurements hold under the described experimental conditions, the work supplies concrete, reproducible metrics showing that federated averaging, formal (ε,δ)-DP, and INT8 quantization can be composed for edge deployment in a medical setting without forcing a privacy-efficiency trade-off. The empirical independence finding and the explicit ε sweep provide actionable guidance beyond abstract privacy claims.
major comments (2)
- [Experimental Setup] The ten simulated non-IID partitions of PTB-XL (described in the experimental setup) are load-bearing for the non-IID performance claim, yet the manuscript supplies insufficient detail on the exact partitioning procedure, per-client label or feature distributions, and any validation that these partitions approximate real cross-hospital heterogeneity; without this, the assertion that federated learning 'matches or exceeds' centralized performance cannot be fully assessed for robustness.
- [Results] Results tables reporting AUROC values (e.g., federated ConvAE at 0.782) and latency reductions omit standard deviations across random seeds, confidence intervals, or statistical significance tests comparing federated versus centralized runs; this weakens the quantitative claim that penalties from DP and quantization are independent and that performance 'matches or exceeds' the baseline.
minor comments (3)
- [Abstract] The abstract states that 'an ε sweep identifies ε=4 as the recommended clinical operating point' without stating the precise selection criterion (e.g., maximum allowable AUROC drop or a specific (ε,δ) target); this should be clarified in the main text.
- Hyperparameters (local epochs, learning rate, batch size, DP noise multiplier, clipping norm) are referenced but not collected in a single reproducibility table; adding one would improve clarity.
- Figure captions for the Raspberry Pi 4 latency and model-size plots should explicitly note the number of inference runs averaged and any temperature or power constraints used during benchmarking.
Simulated Author's Rebuttal
We thank the referee for the constructive feedback and the recommendation for minor revision. We address each major comment below and indicate the revisions that will be incorporated.
read point-by-point responses
-
Referee: [Experimental Setup] The ten simulated non-IID partitions of PTB-XL (described in the experimental setup) are load-bearing for the non-IID performance claim, yet the manuscript supplies insufficient detail on the exact partitioning procedure, per-client label or feature distributions, and any validation that these partitions approximate real cross-hospital heterogeneity; without this, the assertion that federated learning 'matches or exceeds' centralized performance cannot be fully assessed for robustness.
Authors: We agree that additional detail on the partitioning procedure is warranted to support reproducibility and robustness assessment. In the revised manuscript we will expand the experimental setup section with: (i) the exact algorithm used to create the ten non-IID partitions (including any patient-ID or demographic stratification rules), (ii) summary tables or figures of per-client feature and label distributions, and (iii) a short discussion of how the simulated heterogeneity relates to documented cross-hospital ECG variability in the literature. These additions will allow readers to evaluate the non-IID performance claims more rigorously. revision: yes
-
Referee: [Results] Results tables reporting AUROC values (e.g., federated ConvAE at 0.782) and latency reductions omit standard deviations across random seeds, confidence intervals, or statistical significance tests comparing federated versus centralized runs; this weakens the quantitative claim that penalties from DP and quantization are independent and that performance 'matches or exceeds' the baseline.
Authors: We acknowledge that reporting variability measures would strengthen the quantitative claims. In the revision we will (i) rerun the primary configurations with at least three random seeds, (ii) add standard deviations and 95% confidence intervals to the AUROC and latency tables, and (iii) include paired statistical tests (e.g., Wilcoxon signed-rank) between federated and centralized results. These changes will provide clearer support for the reported performance matching and the empirical independence of the DP and quantization penalties. revision: yes
Circularity Check
No significant circularity identified
full rationale
This is an empirical evaluation paper reporting measured AUROC, latency, and model-size results from federated training, DP-SGD, and INT8 quantization on PTB-XL partitions. All headline claims (FL matching centralized baseline, empirical independence of DP and quantization penalties) are direct experimental outcomes on held-out data; no equation, ansatz, or uniqueness theorem is invoked that reduces the reported quantities to the inputs by construction. No self-citation chain or fitted-parameter renaming appears in the derivation of the central results.
Axiom & Free-Parameter Ledger
free parameters (2)
- epsilon =
4
- number_of_clients =
10
axioms (1)
- domain assumption PTB-XL dataset can be partitioned to represent non-IID cross-hospital distributions
Reference graph
Works this paper leans on
-
[1]
Deep Learning with Differential Privacy
M. Abadi et al. “Deep Learning with Differential Privacy”. In:ACM CCS. 2016, pp. 308–318
2016
-
[2]
Federated Learning and Differential Privacy Tech- niques on Multi-hospital Population-scale Electrocardiogram Data
V . Agrawal et al. “Federated Learning and Differential Privacy Tech- niques on Multi-hospital Population-scale Electrocardiogram Data”. In: ICMHI. 2024, pp. 143–152
2024
-
[3]
ECG De-Anonymization: Real-World Risks and a Privacy-by-Design Mitigation Strategy
H. Aguelal and P. Palmieri. “ECG De-Anonymization: Real-World Risks and a Privacy-by-Design Mitigation Strategy”. In:CBMS. 2025, pp. 449–456
2025
-
[4]
Unsupervised Transformer-Based Anomaly Detection in ECG Signals
A. Alamr and A. Artoli. “Unsupervised Transformer-Based Anomaly Detection in ECG Signals”. In:Algorithms16 (2023), p. 152
2023
-
[5]
https : / / anonymous
Anonymous.ECG-Federated-AE: Anonymous Source Code Reposi- tory. https : / / anonymous . 4open . science / r / ecg - federated - ae - DB18. 2026
2026
-
[6]
Cryptology ePrint Archive, Paper 2020/704
Bell et al.Secure Single-Server Aggregation with (Poly)Logarithmic Overhead. Cryptology ePrint Archive, Paper 2020/704. 2020
2020
-
[7]
Federated Disentangled Representation Learning for Unsupervised Brain Anomaly Detection
C. I. Bercea et al. “Federated Disentangled Representation Learning for Unsupervised Brain Anomaly Detection”. In:Nat. Mach. Intell.4 (2022), pp. 685–695
2022
-
[8]
Fusion of Personalized Federated Learning with Differential Privacy for Diagnosis of Arrhythmia Disease
S. M. Bokhari et al. “Fusion of Personalized Federated Learning with Differential Privacy for Diagnosis of Arrhythmia Disease”. In:PLOS ONE20 (2025), e0327108
2025
-
[9]
Federated Learning Strategies for Atrial Fibrillation Detection
W. Chorney and S. H. Ling. “Federated Learning Strategies for Atrial Fibrillation Detection”. In:J. Exp. Theor. Anal.3 (2025), p. 23
2025
-
[10]
Dwork and A
C. Dwork and A. Roth.The Algorithmic Foundations of Differential Privacy. V ol. 9. Found. Trends Theor. Comput. Sci., 2014
2014
-
[11]
Our Data, Ourselves: Privacy Via Distributed Noise Generation
C. Dwork et al. “Our Data, Ourselves: Privacy Via Distributed Noise Generation”. In:EUROCRYPT. Springer, 2006, pp. 486–503
2006
-
[12]
Y . Elmir et al.Federated Learning with Gramian Angular Fields for Privacy-Preserving ECG Classification on Heterogeneous IoT Devices. arXiv:2511.03753. 2025
-
[13]
Fu et al.Differentially Private Federated Learning: A Systematic Review
J. Fu et al.Differentially Private Federated Learning: A Systematic Review. arXiv:2405.08299. 2025
-
[14]
M. Garreta Basora and M. O. Mulayim.An Attention-Augmented VAE- BiLSTM Framework for Anomaly Detection in 12-Lead ECG Signals. arXiv:2510.05919. 2025
-
[15]
A. Ghazarian et al.Privacy-Preserving ECG Data Analysis with Differential Privacy: A Literature Review and A Case Study. arXiv:2406.13880. 2024
-
[16]
PhysioBank, PhysioToolkit, and PhysioNet
A. L. Goldberger et al. “PhysioBank, PhysioToolkit, and PhysioNet”. In:Circulation101 (2000), e215–e220
2000
-
[17]
Application of Federated Learning Tech- niques for Arrhythmia Classification Using 12-Lead ECG Signals
D. M. J. Gutierrez et al. “Application of Federated Learning Tech- niques for Arrhythmia Classification Using 12-Lead ECG Signals”. In:ALGOCLOUD. Springer, 2023, pp. 38–65
2023
-
[18]
Reliable ECG Anomaly Detection on Edge Devices for Internet of Medical Things Applications
M. Hizem et al. “Reliable ECG Anomaly Detection on Edge Devices for Internet of Medical Things Applications”. In:Sensors25 (2025), p. 2496
2025
-
[19]
Federated Learning-Based Privacy-Preserving ECG Signal Classification for IoMT
F. Jiang et al. “Federated Learning-Based Privacy-Preserving ECG Signal Classification for IoMT”. In:ICCC. 2025, pp. 1–6
2025
-
[20]
Secure, Privacy-Preserving and Federated Machine Learning in Medical Imaging
G. A. Kaissis et al. “Secure, Privacy-Preserving and Federated Machine Learning in Medical Imaging”. In:Nat. Mach. Intell.2 (2020), pp. 305– 311
2020
-
[21]
Cross-device Federated Unsupervised Learning for the Detection of Anomalies in Single-Lead Electrocardio- gram Signals
M. Kapsecker and S. M. Jonas. “Cross-device Federated Unsupervised Learning for the Detection of Anomalies in Single-Lead Electrocardio- gram Signals”. In:PLOS Digit. Health4 (2025)
2025
-
[22]
D. P. Kingma and M. Welling.Auto-Encoding Variational Bayes. arXiv:1312.6114. 2013
work page internal anchor Pith review Pith/arXiv arXiv 2013
-
[23]
Quantizing deep convolutional networks for efficient inference: A whitepaper
R. Krishnamoorthi.Quantizing Deep Convolutional Networks for Ef- ficient Inference: A Whitepaper. arXiv:1806.08342. 2018
work page internal anchor Pith review Pith/arXiv arXiv 2018
-
[24]
Enhanced Federated Anomaly Detection through Autoencoders Using Summary Statistics-Based Thresholding
S. Laridi et al. “Enhanced Federated Anomaly Detection through Autoencoders Using Summary Statistics-Based Thresholding”. In:Sci. Rep.14 (2024), p. 26704
2024
-
[25]
Communication-Efficient Learning of Deep Net- works from Decentralized Data
B. McMahan et al. “Communication-Efficient Learning of Deep Net- works from Decentralized Data”. In:AISTATS. 2017, pp. 1273–1282
2017
-
[26]
Learning Differentially Private Recurrent Language Models
H. B. McMahan et al. “Learning Differentially Private Recurrent Language Models”. In:ICLR. 2018
2018
-
[27]
Rényi Differential Privacy
I. Mironov. “Rényi Differential Privacy”. In:CSF. 2017, pp. 263–275
2017
-
[28]
Nardi et al.Anomaly Detection through Unsupervised Federated Learning
M. Nardi et al.Anomaly Detection through Unsupervised Federated Learning. arXiv:2209.04184. 2022
-
[29]
Unsupervised ECG Analysis: A Review
K. Nezamabadi et al. “Unsupervised ECG Analysis: A Review”. In: IEEE Rev. Biomed. Eng.16 (2023), pp. 208–224
2023
-
[30]
ECG-DPSHAP: An Approach towards Privacy- Preserving SHAP-Based Explainable AI for 12-Lead ECG Classifica- tion Model
S. Nuannimnoi et al. “ECG-DPSHAP: An Approach towards Privacy- Preserving SHAP-Based Explainable AI for 12-Lead ECG Classifica- tion Model”. In:IC4e. 2025
2025
-
[31]
PyTorch: An Imperative Style, High-Performance Deep Learning Library
A. Paszke et al. “PyTorch: An Imperative Style, High-Performance Deep Learning Library”. In:NeurIPS. 2019, pp. 8024–8035
2019
-
[32]
A Secure Multi-Modal Federated Transfer Learning System for ECG Classification
N. Phan. “A Secure Multi-Modal Federated Transfer Learning System for ECG Classification”. In:Neurocomputing(2026)
2026
-
[33]
How to DP-fy ML: A Practical Guide to Machine Learning with Differential Privacy
N. Ponomareva et al. “How to DP-fy ML: A Practical Guide to Machine Learning with Differential Privacy”. In:JAIR77 (2023), pp. 1113–1201
2023
-
[34]
Handling Data Heterogeneity in Federated Learning for Medical Imaging: A Review
L. Qu et al. “Handling Data Heterogeneity in Federated Learning for Medical Imaging: A Review”. In:Med. Image Anal.82 (2022), p. 102570
2022
-
[35]
Designing ECG Monitoring Healthcare System with Federated Transfer Learning and Explainable AI
A. Raza et al. “Designing ECG Monitoring Healthcare System with Federated Transfer Learning and Explainable AI”. In:Knowl.-Based Syst.236 (2022), p. 107763
2022
-
[36]
ECG-based Real-Time Arrhythmia Monitoring Using Quantized Deep Neural Networks: A Feasibility Study
H. Ribeiro et al. “ECG-based Real-Time Arrhythmia Monitoring Using Quantized Deep Neural Networks: A Feasibility Study”. In:Comput. Biol. Med.143 (2022), p. 105249
2022
-
[37]
Deep Learning for ECG Analysis: Benchmarks and Insights from PTB-XL
N. Strodthoff et al. “Deep Learning for ECG Analysis: Benchmarks and Insights from PTB-XL”. In:IEEE J. Biomed. Health Inform.25 (2021), pp. 1519–1528
2021
-
[38]
FEEL-ECG: Federated Edge Learning for Person- alized and Explainable ECG Monitoring with Adaptive Compression and Preprocessing
K. Swetha et al. “FEEL-ECG: Federated Edge Learning for Person- alized and Explainable ECG Monitoring with Adaptive Compression and Preprocessing”. In:INDISCON. 2025, pp. 1–7
2025
-
[39]
PTB-XL, a Large Publicly Available Electrocardio- graphy Dataset
P. Wagner et al. “PTB-XL, a Large Publicly Available Electrocardio- graphy Dataset”. In:Sci. Data7 (2020), p. 154
2020
-
[40]
Linkage Attacks Expose Identity Risks in Public ECG Data Sharing
Z. Wang et al. “Linkage Attacks Expose Identity Risks in Public ECG Data Sharing”. In:IEEE EMBC. 2025
2025
-
[41]
Federated Learning With Deep Neural Networks: A Privacy-Preserving Approach to Enhanced ECG Classification
K. Weimann and T. O. F. Conrad. “Federated Learning With Deep Neural Networks: A Privacy-Preserving Approach to Enhanced ECG Classification”. In:IEEE J. Biomed. Health Inform.28 (2024)
2024
-
[42]
World Health Organization.Cardiovascular Diseases (CVDs) – Fact Sheet. WHO. 2021
2021
-
[43]
Group Normalization
Y . Wu and K. He. “Group Normalization”. In:ECCV. 2018, pp. 3–19
2018
-
[44]
Yousefpour et al.Opacus: User-Friendly Differential Privacy Li- brary in PyTorch
A. Yousefpour et al.Opacus: User-Friendly Differential Privacy Li- brary in PyTorch. arXiv:2109.12298. 2021
-
[45]
A Two-Stage Differential Privacy Scheme for FL Based on Edge Intelligence
L. Zhang et al. “A Two-Stage Differential Privacy Scheme for FL Based on Edge Intelligence”. In:IEEE J. Biomed. Health Inform.28 (2024), pp. 3349–3360
2024
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.