What neurosurgeons need to see: synthetic intra-operative MRI from ultrasound for brain-shift compensation in brain tumour surgery
Pith reviewed 2026-06-28 07:03 UTC · model grok-4.3
The pith
A pipeline merges preoperative MRI with ultrasound-derived synthetic images to produce updated whole-brain volumes reflecting post-resection state.
A machine-rendered reading of the paper's core claim, the machinery that carries it, and where it could break.
Core claim
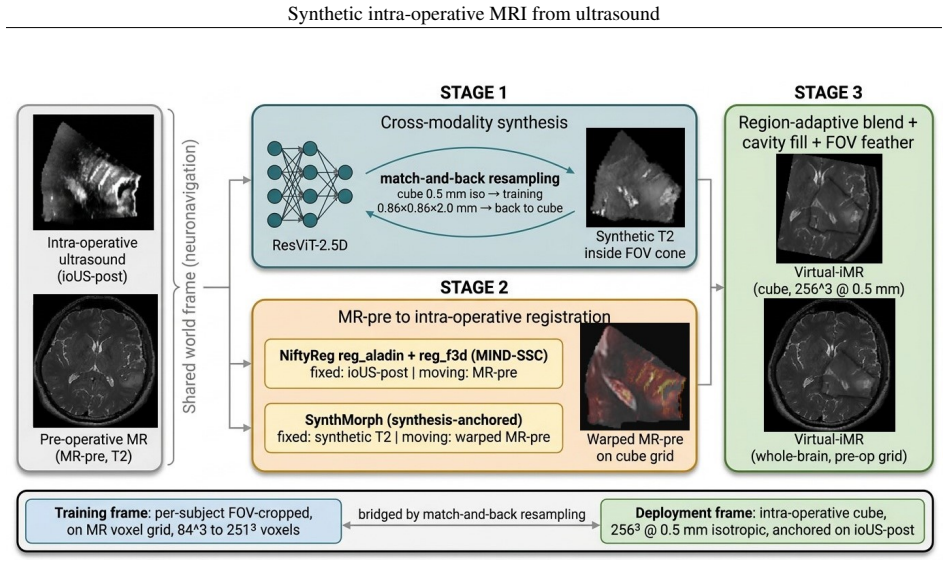
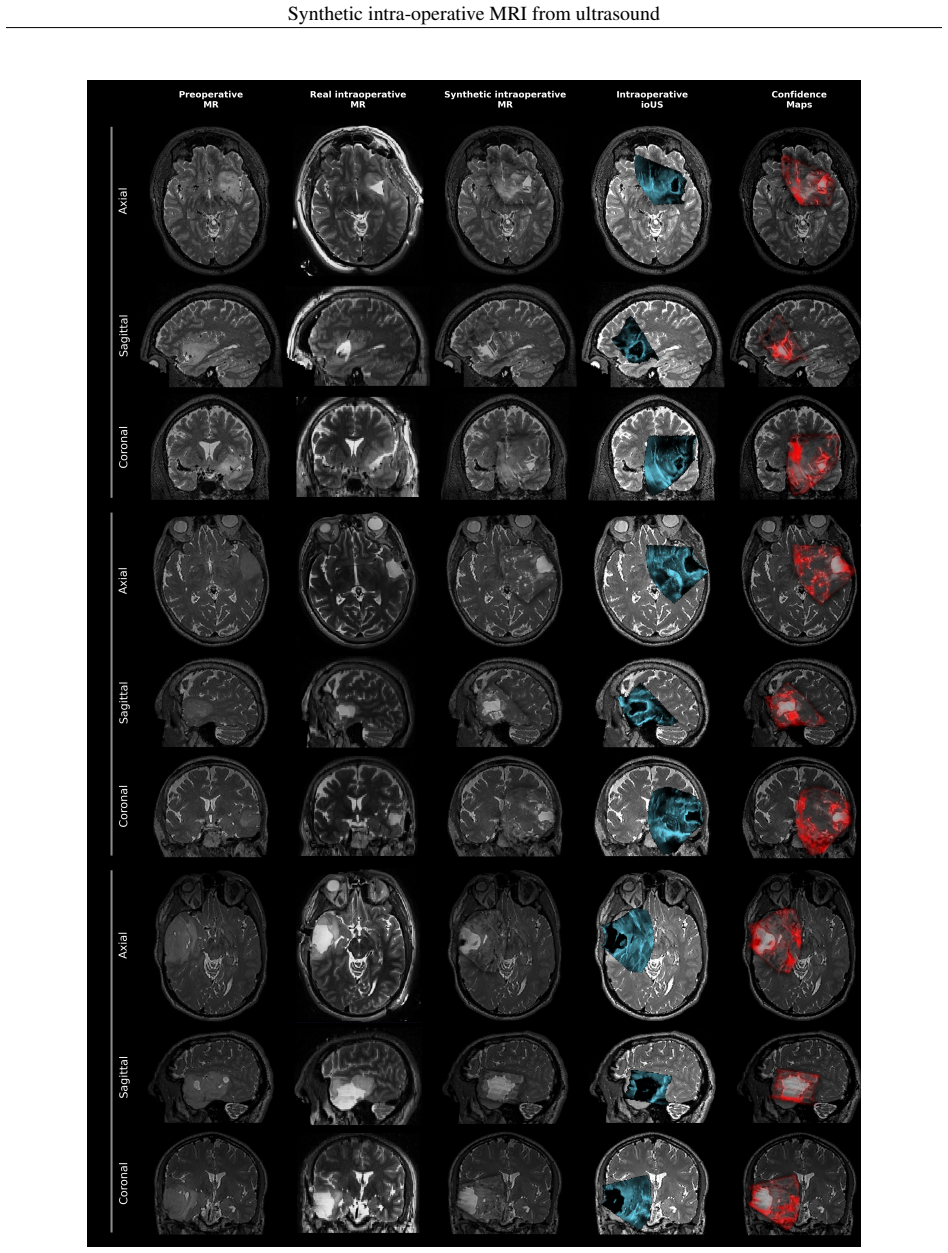
The central claim is that the integrated volume reflects the intraoperative post-resection state inside the ultrasound field of view, achieved by synthesis from ioUS followed by synthesis-anchored registration, thereby providing the surgeon with an MRI-like update of the operative field.
What carries the argument
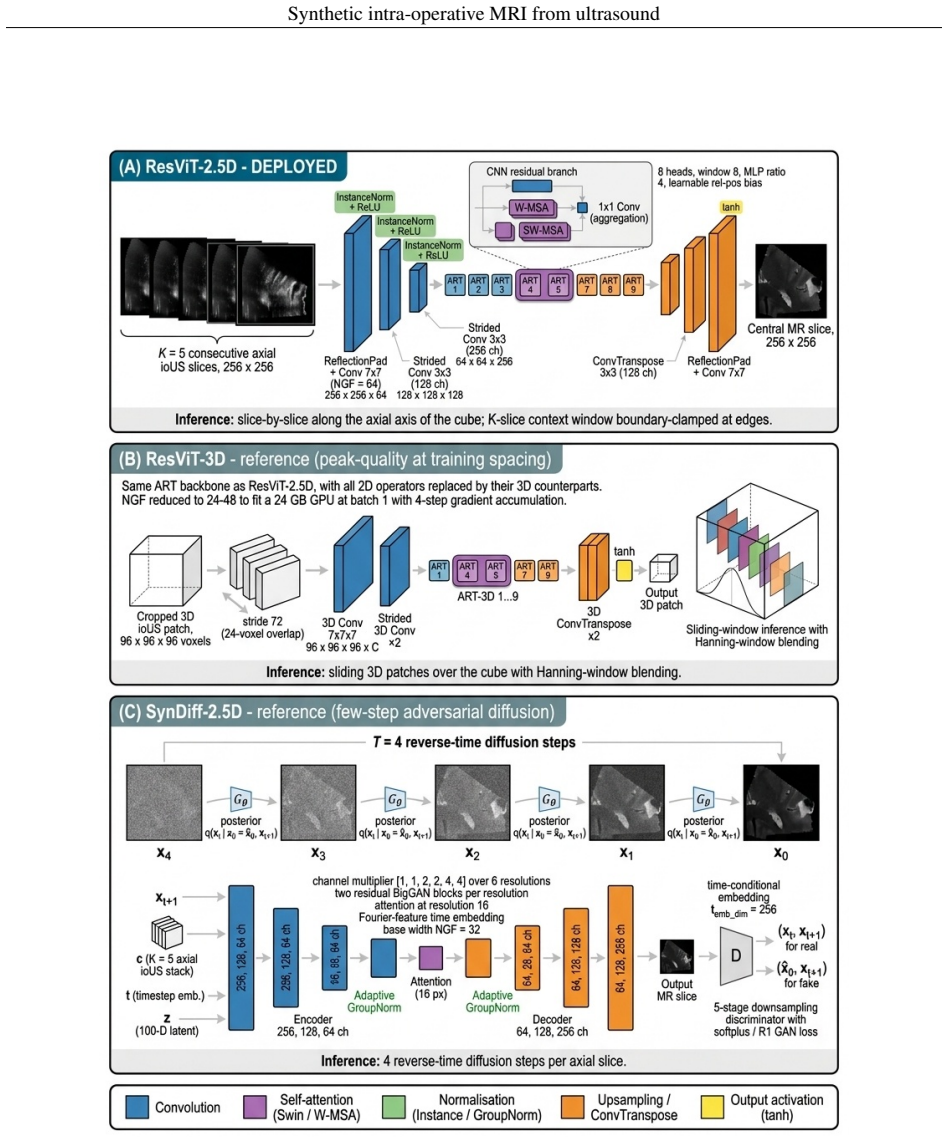
The ResViT-2.5D residual-transformer synthesis backbone that generates a synthetic MRI from ioUS to anchor subsequent deformable registration and produce the merged whole-brain volume.
If this is right
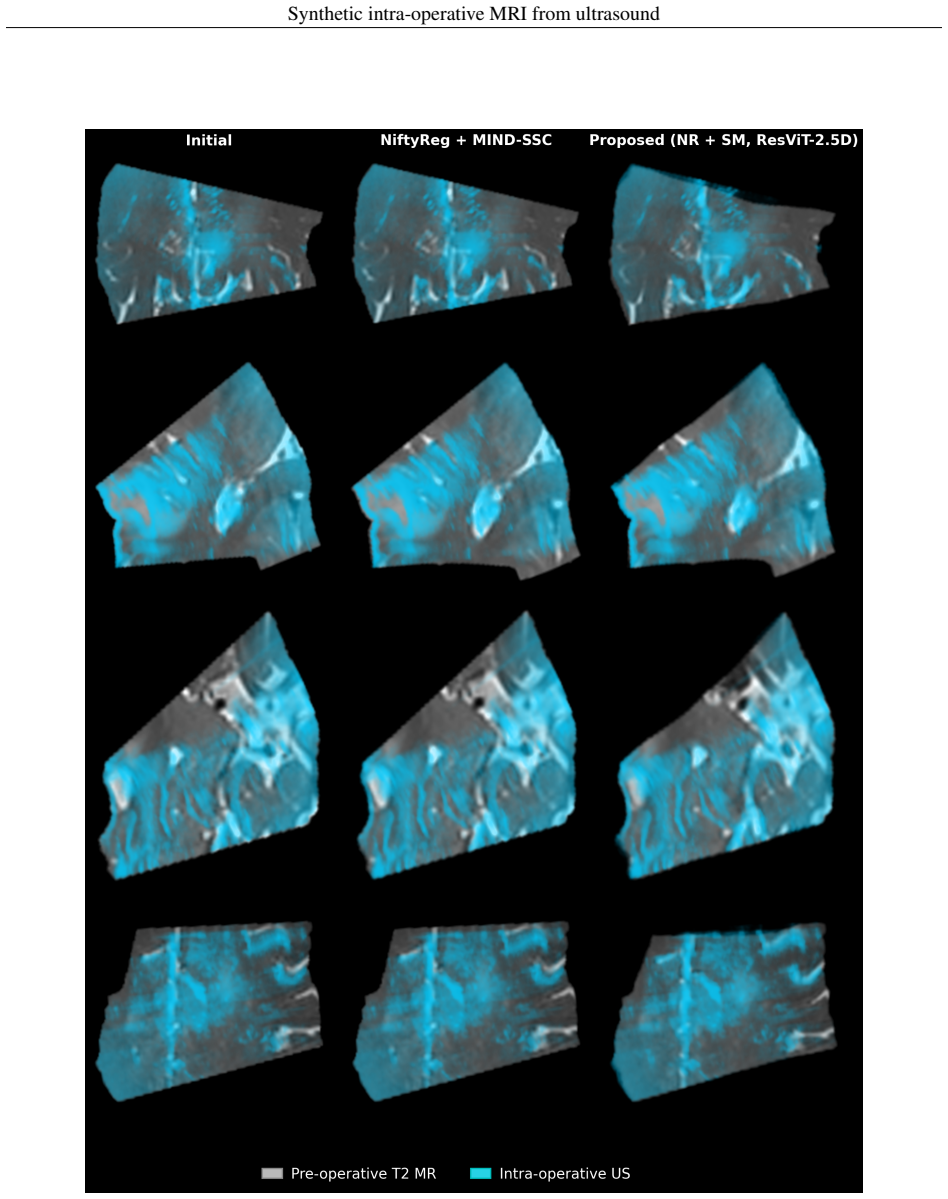
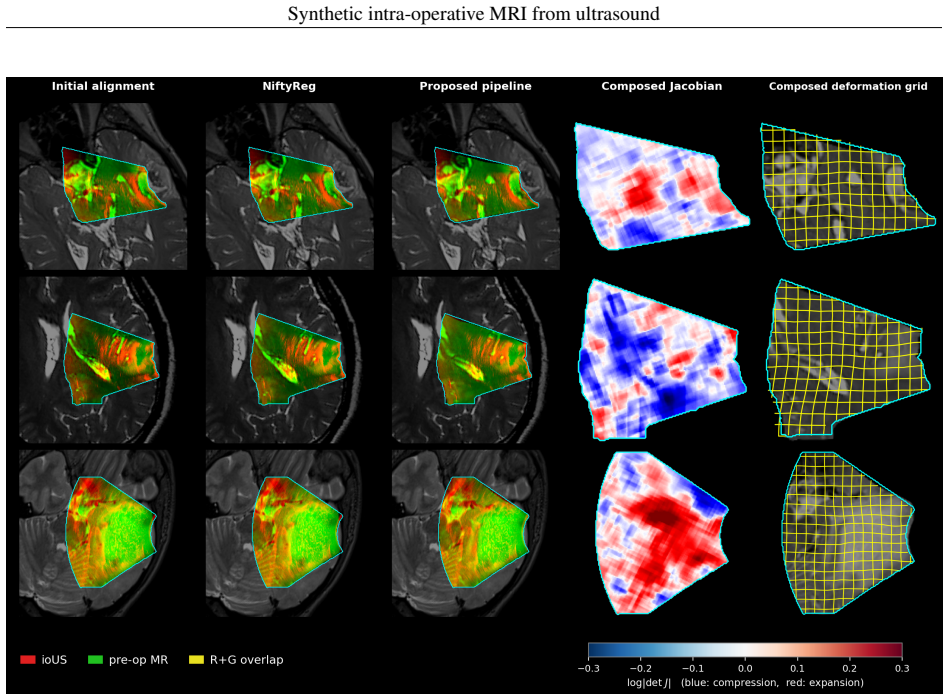
- The synthesis-anchored registration reduces mean target registration error from 6.27 mm to 5.86 mm while producing a diffeomorphic deformation field in every subject.
- The integrated volume reflects the post-resection state inside the ultrasound field of view and matches intraoperative T2 across structural, intensity, and perceptual metrics.
- The pipeline operates directly on raw scanner inputs and yields results comparable to a strong classical NiftyReg baseline.
Where Pith is reading between the lines
- The whole-brain update could allow surgeons to visualize changes outside the narrow ultrasound field of view if the synthesis extrapolates reliably.
- Real-time integration testing in the operating room would determine whether the updated volumes alter surgical decisions compared with standard neuronavigation.
- The same synthesis-plus-anchored-registration pattern might apply to other procedures where ultrasound is available but full intraoperative MRI is not.
Load-bearing premise
The synthetic MRI generated from intraoperative ultrasound accurately represents structures absent from the preoperative scan such as the resection cavity and residual tumor.
What would settle it
Direct visual or quantitative comparison of the synthetic volume against actual intraoperative MRI in additional post-resection cases focused on fidelity inside the resection cavity.
Figures
read the original abstract
Maximal safe resection is the primary objective in glioma surgery. Neuronavigation guidance is progressively degraded by brain shift after dural opening. Intraoperative MRI can compensate but needs dedicated infrastructure and is rarely available, whereas intraoperative ultrasound (ioUS) is inexpensive, repeatable, and compatible with routine workflows. Navigation systems combining ioUS with preoperative MRI usually rely on rigid registration; even deformable multimodal registration is limited by ultrasound speckle contrast, a narrow field of view, and the inability to represent structures absent from the preoperative scan, most critically the resection cavity and residual tumor. We propose an end-to-end pipeline that generates a new whole-brain MRI volume in the preoperative imaging space by merging the preoperative MRI, a synthetic MRI generated from the ioUS, and a deformable registration anchored on that synthetic image. It integrates a 2.5D residual-transformer synthesis backbone (ResViT-2.5D) and a two-stage registration coupling NiftyReg with a synthesis-anchored SynthMorph stage, operating directly on raw scanner inputs. On a post-resection ReMIND cohort, ResViT-2.5D produced synthetic images closely matching the intraoperative T2 across structural, intensity, and perceptual metrics. In 14 subjects with 215 expert landmarks, the synthesis-anchored registration reduced the mean target registration error from 6.27 to 5.86 mm, matching a strong classical NiftyReg baseline (5.85 mm) while yielding a diffeomorphic deformation field in every subject. The contribution is not a gain in registration accuracy but the integrated volume itself, which inside the ultrasound field of view it reflects the intraoperative post-resection state. This provides the surgeon with an MRI-like update of the operative field with potential for integration into surgical-navigation workflows.
Editorial analysis
A structured set of objections, weighed in public.
Referee Report
Summary. The manuscript proposes an end-to-end pipeline that synthesizes a whole-brain intraoperative MRI volume from preoperative MRI and intraoperative ultrasound (ioUS) using a ResViT-2.5D residual-transformer network, then merges it with a two-stage deformable registration (NiftyReg followed by synthesis-anchored SynthMorph) to compensate for brain shift during glioma resection. On a post-resection ReMIND cohort, the synthetic images match intraoperative T2 across structural, intensity, and perceptual metrics; in 14 subjects with 215 expert landmarks the synthesis-anchored registration yields a mean target registration error (TRE) of 5.86 mm (down from 6.27 mm), statistically equivalent to a strong classical NiftyReg baseline (5.85 mm) while producing a diffeomorphic deformation field in every case. The stated contribution is the integrated volume itself, which is claimed to reflect the post-resection state inside the ultrasound field of view.
Significance. If the synthesis accurately renders resection cavities and residual tumor (structures absent from the preoperative scan) and the deformation field extrapolates reliably outside the narrow ultrasound FOV, the method could supply MRI-like intraoperative updates using only standard ioUS hardware, removing the need for dedicated intraoperative MRI infrastructure. The equivalence of registration accuracy to the classical baseline underscores that any clinical value resides entirely in the fidelity and usability of the synthesized volume rather than in improved alignment metrics.
major comments (2)
- [Abstract] Abstract: The reported TRE reduction (6.27 mm o 5.86 mm) exactly matches the NiftyReg baseline (5.85 mm), so the central claim that the integrated volume supplies a usable whole-brain update rests solely on the untested ability of ResViT-2.5D to correctly depict resection cavity and residual tumor inside the US FOV and to support reliable extrapolation outside it; only aggregate structural/intensity/perceptual metrics are presented, with no isolated error quantification or independent ground-truth validation on these new structures.
- [Abstract] Abstract / Methods (implied): No information is supplied on training/validation splits, hyperparameter selection protocol, or the precise landmark placement and annotation procedure used for the 215 landmarks in 14 subjects; given the small cohort size, these omissions leave open the possibility that the reported matching metrics and TRE values are sensitive to post-hoc choices.
minor comments (1)
- [Abstract] Abstract: The sentence fragment 'which inside the ultrasound field of view it reflects the intraoperative post-resection state' is grammatically incomplete and should be rephrased for clarity.
Simulated Author's Rebuttal
We thank the referee for the thorough review and constructive feedback. We address each major comment below and outline the revisions we will make to the manuscript.
read point-by-point responses
-
Referee: [Abstract] Abstract: The reported TRE reduction (6.27 mm → 5.86 mm) exactly matches the NiftyReg baseline (5.85 mm), so the central claim that the integrated volume supplies a usable whole-brain update rests solely on the untested ability of ResViT-2.5D to correctly depict resection cavity and residual tumor inside the US FOV and to support reliable extrapolation outside it; only aggregate structural/intensity/perceptual metrics are presented, with no isolated error quantification or independent ground-truth validation on these new structures.
Authors: We agree that the TRE improvement is negligible and statistically equivalent to the NiftyReg baseline, consistent with our manuscript's emphasis that the primary contribution is the integrated synthetic volume rather than registration accuracy. The structural, intensity, and perceptual metrics are computed across the full image, including the resection cavity and residual tumor within the ioUS field of view. However, we acknowledge the value of more targeted validation. In the revised manuscript, we will include additional qualitative examples highlighting the synthesis of resection cavities and residual tumor, and discuss the limitations of aggregate metrics. Independent ground-truth for these structures beyond the provided intraoperative T2 is not available in the ReMIND dataset, limiting quantitative isolation. revision: partial
-
Referee: [Abstract] Abstract / Methods (implied): No information is supplied on training/validation splits, hyperparameter selection protocol, or the precise landmark placement and annotation procedure used for the 215 landmarks in 14 subjects; given the small cohort size, these omissions leave open the possibility that the reported matching metrics and TRE values are sensitive to post-hoc choices.
Authors: We apologize for these omissions in the manuscript. The revised version will explicitly detail the training/validation splits used for ResViT-2.5D, the hyperparameter selection protocol (including any cross-validation approach), and the landmark annotation procedure, including how the 215 expert landmarks were placed and verified in the 14 subjects. These details will clarify the robustness of the results despite the small cohort size. revision: yes
- Independent ground-truth validation specifically isolating error on resection cavities and residual tumor is not feasible with the current ReMIND dataset, as it lacks paired annotations for these post-resection structures beyond the aggregate image metrics.
Circularity Check
No significant circularity; empirical evaluation on held-out data is self-contained
full rationale
The paper trains ResViT-2.5D on data to synthesize MRI from ioUS, then evaluates the output against real intraoperative T2 images using structural/intensity/perceptual metrics on a post-resection ReMIND cohort. Registration performance is measured via expert landmarks (215 in 14 subjects) and compared to an external classical NiftyReg baseline. No equations or steps reduce a claimed prediction to a fitted input by construction, no self-citations are load-bearing for uniqueness or ansatzes, and the central claim (integrated volume reflecting post-resection state) rests on external empirical matches rather than internal redefinitions. This is the standard non-circular case for a learned synthesis pipeline.
Axiom & Free-Parameter Ledger
free parameters (1)
- ResViT-2.5D network weights
axioms (1)
- domain assumption Synthetic images from ioUS can serve as reliable anchors for diffeomorphic deformable registration
Reference graph
Works this paper leans on
-
[1]
Multitask weakly supervised generative network for MR-US registration
Azampour, M.F., Mach, K., Fatemizadeh, E., Demiray, B., Westenfelder, K., Steiger, K., Eiber, M., Wendler, T., Kainz, B., Navab, N., 2024. Multitask weakly supervised generative network for MR-US registration. IEEE Transactions on Medical Imaging 43, 3780–3793.https://doi.org/10.1109/TMI.2024.3400899
-
[2]
DiffUS: differentiable ultrasound rendering from volumetric imaging.https://arxiv.org/abs/2508.06768
Bertramo, N., Duguey, G., Gopalakrishnan, V ., 2025. DiffUS: differentiable ultrasound rendering from volumetric imaging.https://arxiv.org/abs/2508.06768
arXiv 2025
-
[3]
ResViT: residual vision transformers for multimodal medical image synthesis
Dalmaz, O., Yurt, M., Çukur, T., 2022. ResViT: residual vision transformers for multimodal medical image synthesis. IEEE Transactions on Medical Imaging 41, 2598–2614. https://doi.org/10.1109/TMI.2022. 3167808
-
[4]
Unified brain MR-ultrasound synthesis using multi-modal hierarchical representations
Dorent, R., Haouchine, N., Kögl, F., Joutard, S., Juvekar, P., Torio, E., Golby, A., Ourselin, S., Frisken, S., Vercauteren, T., Kapur, T., Wells, W.M., 2023. Unified brain MR-ultrasound synthesis using multi-modal hierarchical representations. In: Medical Image Computing and Computer-Assisted Intervention – MICCAI 2023, LNCS 14229. Springer, pp. 448–458....
-
[5]
The Brain Resection Multimodal Image Registration (ReMIND2Reg) 2025 challenge
Dorent, R., Rigolo, L., Galvin, C.P., Chen, J., Heinrich, M.P., Carass, A., Colliot, O., Wassermann, D., Golby, A., Kapur, T., Wells, W., 2025. The Brain Resection Multimodal Image Registration (ReMIND2Reg) 2025 challenge. https://arxiv.org/abs/2508.09649
arXiv 2025
-
[6]
Unified cross-modal medical image synthesis with hierarchical mixture of product-of-experts
Dorent, R., Haouchine, N., Golby, A., Frisken, S., Kapur, T., Wells, W., 2026. Unified cross-modal medical image synthesis with hierarchical mixture of product-of-experts. IEEE Transactions on Pattern Analysis and Machine Intelligence 48, 1641–1656.https://doi.org/10.1109/TPAMI.2025.3616632
-
[7]
Esteban-Sinovas, O., Cepeda, S., Arrese, I., Sarabia, R., 2026. A systematic benchmark of intraoperative ultrasound-to-MR synthesis for brain tumour surgery.https://arxiv.org/abs/2606.00630
Pith/arXiv arXiv 2026
-
[8]
3D Slicer as an image computing platform for the Quantitative Imaging Network
Fedorov, A., Beichel, R., Kalpathy-Cramer, J., Finet, J., Fillion-Robin, J.C., Pujol, S., Bauer, C., Jennings, D., Fennessy, F., Sonka, M., Buatti, J., Aylward, S., Miller, J.V ., Pieper, S., Kikinis, R., 2012. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magnetic Resonance Imaging 30, 1323–1341. https://doi.org/10.1016/j...
-
[9]
Gerard, I.J., Kersten-Oertel, M., Petrecca, K., Sirhan, D., Hall, J.A., Collins, D.L., 2017. Brain shift in neuronavi- gation of brain tumors: a review. Medical Image Analysis 35, 403–420. https://doi.org/10.1016/j.media. 2016.08.007. 27 Synthetic intra-operative MRI from ultrasound
-
[10]
Learn2Reg 2024: new benchmark datasets driving progress on new challenges
Hansen, L., Heyer, W., Großbröhmer, C., et al., 2025. Learn2Reg 2024: new benchmark datasets driving progress on new challenges. Journal of Machine Learning for Biomedical Imaging (MELBA) 3, 775–791. https://doi.org/10.59275/j.melba.2025-gc8c
-
[11]
Towards realtime multimodal fusion for image-guided interventions using self-similarities
Heinrich, M.P., Jenkinson, M., Papie˙z, B.W., Brady, S.M., Schnabel, J.A., 2013. Towards realtime multimodal fusion for image-guided interventions using self-similarities. In: MICCAI 2013, LNCS 8149. Springer, pp. 187–194.https://doi.org/10.1007/978-3-642-40811-3_24
-
[12]
Maximizing safe resection of low- and high-grade glioma
Hervey-Jumper, S.L., Berger, M.S., 2016. Maximizing safe resection of low- and high-grade glioma. Journal of Neuro-Oncology 130, 269–282.https://doi.org/10.1007/s11060-016-2110-4
-
[13]
Synth- Morph: learning contrast-invariant registration without acquired images
Hoffmann, M., Billot, B., Greve, D.N., Iglesias, J.E., Fischl, B., Dalca, A.V ., 2022. SynthMorph: learning contrast-invariant registration without acquired images. IEEE Transactions on Medical Imaging 41, 543–558. https://doi.org/10.1109/TMI.2021.3116879
-
[14]
Anatomy-aware and acquisition-agnostic joint registration with SynthMorph
Hoffmann, M., Hoopes, A., Greve, D.N., Fischl, B., Dalca, A.V ., 2024. Anatomy-aware and acquisition-agnostic joint registration with SynthMorph. Imaging Neuroscience 2, 1–33. https://doi.org/10.1162/imag_a_ 00197
-
[15]
Uncertainty estimates and multi-hypotheses networks for optical flow
Ilg, E., Çiçek, Ö., Galesso, S., Klein, A., Makansi, O., Hutter, F., Brox, T., 2018. Uncertainty estimates and multi-hypotheses networks for optical flow. In: Computer Vision – ECCV 2018, LNCS 11211. Springer, pp. 677–693.https://doi.org/10.1007/978-3-030-01234-2_40
-
[16]
Cross-modal conditional latent diffusion model for brain MRI to ultrasound image translation
Jiang, S., Wang, L., Li, Y ., Yang, Z., Zhou, Z., Li, B., 2025. Cross-modal conditional latent diffusion model for brain MRI to ultrasound image translation. Physics in Medicine & Biology 70, 155005. https://doi.org/10. 1088/1361-6560/adf0bc
2025
-
[17]
Jiao, J., Namburete, A.I.L., Papageorghiou, A.T., Noble, J.A., 2020. Self-supervised ultrasound to MRI fetal brain image synthesis. IEEE Transactions on Medical Imaging 39, 4413–4424. https://doi.org/10.1109/TMI. 2020.3018560
work page doi:10.1109/tmi 2020
-
[18]
ReMIND: the brain resection multimodal imaging database
Juvekar, P., Dorent, R., Kögl, F., Torio, E., Barr, C., Rigolo, L., Galvin, C., Jowkar, N., Kazi, A., Haouchine, N., Cheema, H., Navab, N., Pieper, S., Wells, W.M., Bi, W.L., Golby, A., Frisken, S., Kapur, T., 2024. ReMIND: the brain resection multimodal imaging database. Scientific Data 11, 494. https://doi.org/10.1038/ s41597-024-03295-z
2024
-
[19]
Registration of 3D fetal neurosonography and MRI
M. Kuklisova-Murgasova, A. Cifor, R. Napolitano, A. Papageorghiou, G. Quaghebeur, M. A. Rutherford, J. V . Hajnal, J. A. Noble, and J. A. Schnabel. Registration of 3D fetal neurosonography and MRI. Medical Image Analysis, 17(8):1137–1150, 2013.https://10.1016/j.media.2013.07.004
-
[20]
Machado, I., Toews, M., Luo, J., Unadkat, P., Essayed, W., George, E., Teodoro, P., Carvalho, H., Martins, J., Golland, P., Pieper, S., Frisken, S., Golby, A., Wells, W.M., 2018. Non-rigid registration of 3D ultrasound for neurosurgery using automatic feature detection and matching. International Journal of Computer Assisted Radiology and Surgery 13, 1525...
-
[21]
NeuroImage 202, 116094.https://doi.org/10.1016/j.neuroimage.2019.116094
Machado, I., Toews, M., George, E., Unadkat, P., Essayed, W., Luo, J., Teodoro, P., Carvalho, H., Martins, J., Golland, P., Pieper, S., Frisken, S., Golby, A., Wells, W., Ou, Y ., 2019. Deformable MRI-ultrasound registration using correlation-based attribute matching for brain shift correction: accuracy and generality in multi-site data. NeuroImage 202, 1...
-
[22]
Least squares generative adversarial networks
Mao, X., Li, Q., Xie, H., Lau, R.Y .K., Wang, Z., Smolley, S.P., 2017. Least squares generative adversarial networks. In: IEEE International Conference on Computer Vision (ICCV). pp. 2794–2802. https://doi.org/ 10.1109/ICCV.2017.304
-
[23]
Fast free-form deformation using graphics processing units
Modat, M., Ridgway, G.R., Taylor, Z.A., Lehmann, M., Barnes, J., Hawkes, D.J., Fox, N.C., Ourselin, S., 2010. Fast free-form deformation using graphics processing units. Computer Methods and Programs in Biomedicine 98, 278–284.https://doi.org/10.1016/j.cmpb.2009.09.002
-
[24]
Global image registration using a symmetric block-matching approach
Modat, M., Cash, D.M., Daga, P., Winston, G.P., Duncan, J.S., Ourselin, S., 2014. Global image registration using a symmetric block-matching approach. Journal of Medical Imaging 1, 024003. https://doi.org/10.1117/1. JMI.1.2.024003
work page doi:10.1117/1 2014
-
[25]
Morozov, D., Dorent, R., Haouchine, N., 2025. A 3D cross-modal keypoint descriptor for MR-US matching and registration.https://arxiv.org/abs/2507.18551
arXiv 2025
-
[26]
Serial intraoperative magnetic resonance imaging of brain shift
Nabavi, A., Black, P.M., Gering, D.T., Westin, C.F., Mehta, V ., Pergolizzi, R.S., Ferrant, M., Warfield, S.K., Hata, N., Schwartz, R.B., Wells, W.M., Kikinis, R., Jolesz, F.A., 2001. Serial intraoperative magnetic resonance imaging of brain shift. Neurosurgery 48, 787–798.https://doi.org/10.1097/00006123-200104000-00019. 28 Synthetic intra-operative MRI ...
-
[27]
Reconstructing a 3D structure from serial histological sections
Ourselin, S., Roche, A., Subsol, G., Pennec, X., Ayache, N., 2001. Reconstructing a 3D structure from serial histological sections. Image and Vision Computing 19, 25–31. https://doi.org/10.1016/S0262-8856(00) 00052-4
-
[28]
Unsupervised medical image translation with adversarial diffusion models
Özbey, M., Dalmaz, O., Dar, S.U.H., Bedel, H.A., Öztürk, ¸ S., Güngör, A., Çukur, T., 2023. Unsupervised medical image translation with adversarial diffusion models. IEEE Transactions on Medical Imaging 42, 3524–3539. https://doi.org/10.1109/TMI.2023.3290149
-
[29]
Salmanpour, M.R., Mousavi, A., Xu, Y ., Weeks, W.B., Hacihaliloglu, I., 2026. Influence of high-performance image-to-image translation networks on clinical visual assessment and outcome prediction: utilizing ultrasound to MRI translation in prostate cancer. International Journal of Computer Assisted Radiology and Surgery 21, 125–135.https://doi.org/10.100...
-
[30]
Glioma extent of resection and its impact on patient outcome
Sanai, N., Berger, M.S., 2008. Glioma extent of resection and its impact on patient outcome. Neurosurgery 62, 753–764.https://doi.org/10.1227/01.neu.0000318159.21731.cf
-
[31]
Shetty, P., Yeole, U., Singh, V ., Moiyadi, A., 2021. Navigated ultrasound-based image guidance during resection of gliomas: practical utility in intraoperative decision-making and outcomes. Neurosurgical Focus 50, E14. https://doi.org/10.3171/2020.10.FOCUS20550
-
[32]
ConvexAdam: self- configuring dual-optimization-based 3D multitask medical image registration
Siebert, H., Großbröhmer, C., Hansen, L., Heinrich, M.P., 2025. ConvexAdam: self-configuring dual-optimization- based 3D multitask medical image registration. IEEE Transactions on Medical Imaging 44, 738–748. https: //doi.org/10.1109/TMI.2024.3462248
-
[33]
Silverstein, N., Beloosesky, R., Leibowitz, E., Azhari, H., 2025. Translation of fetal brain ultrasound images into pseudo-MRI images using artificial intelligence.https://arxiv.org/abs/2504.02408
arXiv 2025
-
[34]
Singh, S., Bewoor, M., Ranapurwala, A., Rai, S., Patil, S., 2023. BrainV oxGen: deep learning framework for synthesis of ultrasound to MRI.https://arxiv.org/abs/2310.08608
arXiv 2023
-
[35]
Ability of navigated 3D ultrasound to delineate gliomas and metastases: comparison of image interpretations with histopathology
Unsgård, G., Selbekk, T., Brostrup Müller, T., Ommedal, S., Torp, S.H., Myhr, G., Bang, J., Nagelhus Hernes, T.A., 2005. Ability of navigated 3D ultrasound to delineate gliomas and metastases: comparison of image interpretations with histopathology. Acta Neurochirurgica 147, 1259–1269. https://doi.org/10.1007/ s00701-005-0624-1
2005
-
[36]
Wang, G., Li, W., Aertsen, M., Deprest, J., Ourselin, S., Vercauteren, T., 2019. Aleatoric uncertainty estimation with test-time augmentation for medical image segmentation with convolutional neural networks. Neurocomputing 338, 34–45.https://doi.org/10.1016/j.neucom.2019.01.103
-
[37]
Image quality as- sessment: from error visibility to structural similarity
Wang, Z., Bovik, A.C., Sheikh, H.R., Simoncelli, E.P., 2004. Image quality assessment: from error visibility to structural similarity. IEEE Transactions on Image Processing 13, 600–612. https://doi.org/10.1109/TIP. 2003.819861
work page doi:10.1109/tip 2004
-
[38]
High-resolution image synthesis and semantic manipulation with conditional GANs
Wang, T.C., Liu, M.Y ., Zhu, J.Y ., Tao, A., Kautz, J., Catanzaro, B., 2018. High-resolution image synthesis and semantic manipulation with conditional GANs. In: IEEE Conference on Computer Vision and Pattern Recognition (CVPR). pp. 8798–8807.https://doi.org/10.1109/CVPR.2018.00917
-
[39]
Wang, J., Chen, X., Zhang, Y ., Liu, M., Zhang, H., 2024. Unsupervised multimodal 3D medical image registration with multilevel correlation balanced optimization. https://arxiv.org/abs/2409.05040. Learn2Reg 2024 challenge submission
arXiv 2024
-
[40]
Wang, J., Liu, Z., Liu, M., Chen, X., Yu, X., Wang, Y ., Zhang, H., 2026. Unsupervised MR-US multimodal image registration with multilevel correlation pyramidal optimization.https://arxiv.org/abs/2602.06288
arXiv 2026
-
[41]
Global registration of ultrasound to MRI using the LC2 metric for enabling neurosurgical guidance
Wein, W., Ladikos, A., Fuerst, B., Shah, A., Sharma, K., Navab, N., 2013. Global registration of ultrasound to MRI using the LC2 metric for enabling neurosurgical guidance. In: MICCAI 2013, LNCS 7908. Springer, pp. 34–41.https://doi.org/10.1007/978-3-642-40811-3_5
-
[42]
Xiao, Y ., Rivaz, H., Chabanas, M., Fortin, M., Machado, I., Ou, Y ., Heinrich, M.P., Schnabel, J.A., Zhong, X., Maier, A., Wein, W., Shams, R., Kadoury, S., Drobny, D., Modat, M., Reinertsen, I., 2020. Evaluation of MRI to ultrasound registration methods for brain shift correction: the CuRIOUS2018 challenge. IEEE Transactions on Medical Imaging 39, 777–7...
-
[43]
Zhang, R., Isola, P., Efros, A.A., Shechtman, E., Wang, O., 2018. The unreasonable effectiveness of deep features as a perceptual metric. In: IEEE Conference on Computer Vision and Pattern Recognition (CVPR). pp. 586–595. https://doi.org/10.1109/CVPR.2018.00068. 29
discussion (0)
Sign in with ORCID, Apple, or X to comment. Anyone can read and Pith papers without signing in.